- Scabies
-
Scabies Classification and external resources 
A photomicrograph of an itch mite (Sarcoptes scabiei).ICD-10 B86 ICD-9 133.0 DiseasesDB 11841 MedlinePlus 000830 eMedicine derm/382 emerg/517 ped/2047 MeSH D012532 Scabies (from Latin: scabere, "to scratch"),[1] known colloquially as the seven-year itch,[2] is a contagious skin infection that occurs among humans and other animals. It is caused by a tiny and usually not directly visible parasite, the mite Sarcoptes scabiei, which burrows under the host's skin, causing intense allergic itching. The infection in animals (caused by different but related mite species) is called sarcoptic mange.
The disease may be transmitted from objects but is most often transmitted by direct skin-to-skin contact, with a higher risk with prolonged contact. Initial infections require four to six weeks to become symptomatic. Reinfection, however, may manifest symptoms within as little as 24 hours. Because the symptoms are allergic, their delay in onset is often mirrored by a significant delay in relief after the parasites have been eradicated. Crusted scabies, formerly known as Norwegian scabies, is a more severe form of the infection often associated with immunosuppression.
The disease can be effectively treated with a number of medications. Permethrin cream is the most effective, but expensive compared to other treatments. Crotamiton is less effective, but also nontoxic and soothing. Ivermectin may be used orally and topically. Treatment with lindane preparations has fallen out of favor due to high toxicity and parasite resistance. In order to prevent re-infection, the host's contacts are also often treated.
Contents
Signs and symptoms
The characteristic symptoms of a scabies infection include intense itching and superficial burrows.[3] The burrow tracks are often linear, to the point that a neat "line" of four or more closely placed and equally developed mosquito-like "bites," is almost diagnostic of the disease.
Itching
In the classic scenario, the itch is made worse by warmth and is usually experienced as being worse at night, possibly because there are fewer distractions.[3] As a symptom it is less common in the elderly.[3]
Rash
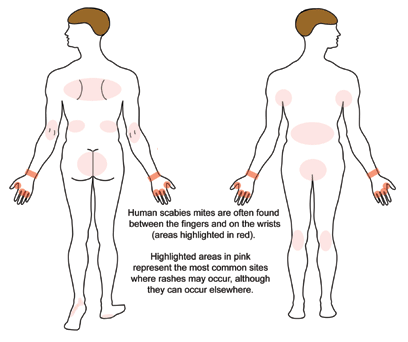
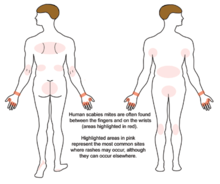 Commonly involved sites of rashes of scabies.[4]
Commonly involved sites of rashes of scabies.[4]
The superficial burrows of scabies usually occur in the area of the hands, feet, wrists, elbows, back, buttocks, and external genitals.[3] The burrows are created by excavation of the adult mite in the epidermis.[3]
In most people, the trails of the burrowing mites show as linear or s-shaped tracks in the skin, often accompanied by what appear as rows of small pimple-like mosquito, or insect bites. These signs are often found in crevices of the body, such as on the webs of fingers and toes, around the genital area, and under the breasts of women.[5]
Symptoms typically appear 2–6 weeks after infestation for individuals never before exposed to scabies. For those having been previously exposed, the symptoms can appear within several days after infestation. However, it is not unknown for symptoms to appear after several months or years.[6]Acropustulosis, or blisters and pustules on the palms and soles of the feet, are characteristic symptoms of scabies in infants.[5]
-

Scabies of the foot
-

Scabies of the arm
-

Scabies of the hand
-

Scabies of the finger
Crusted scabies
 Crusted scabies in a person with AIDS
Crusted scabies in a person with AIDSThe elderly and people with an impaired immune system, such as HIV and cancer sufferers or transplant patients on immunosuppressive drugs, are susceptible to crusted scabies (formerly called "Norwegian scabies").[3][6][7] On those with a weaker immune system, the host becomes a more fertile breeding ground for the mites, which spread over the host's body, except the face. Sufferers of crusted scabies exhibit scaly rashes, slight itching, and thick crusts of skin that contain thousands of mites.[8] Such areas make eradication of mites particularly difficult, as the crusts protect the mites from topical miticides, necessitating prolonged treatment of these areas.
Cause
Main article: Sarcoptes scabieiVideo of the sarcoptes scabiei mite. Life cycle of scabies.[4]
Life cycle of scabies.[4]In the 18th century, Italian biologist Diacinto Cestoni (1637–1718) described the mite now called Sarcoptes scabiei, variety hominis, as the cause of scabies. Sarcoptes is a genus of skin parasites and part of the larger family of mites collectively known as "scab mites". These organisms have 8 legs as adults, and are placed in the same phylogenetic class (Arachnida) as spiders and ticks.
Sarcoptes scabiei are microscopic, but sometimes are visible as pinpoints of white. Pregnant females tunnel into the dead, outermost layer (stratum corneum) of a host's skin and deposit eggs in the shallow burrows. The eggs hatch into larvae in 3–10 days. These young mites move about on the skin and molt into a "nymphal" stage, before maturing as adults, which live 3–4 weeks in the host's skin. Males roam on top of the skin, occasionally burrowing into the skin. In general, there are usually few mites on a healthy hygienic person infested with non-crusted scabies; approximately 11 females in burrows can be found on such a person.[9]
The movement of mites within and on the skin produces an intense itch, which has the characteristics of a delayed cell-mediated inflammatory response to allergens. IgE antibodies are present in the serum and the site of infection, which react to multiple protein allergens the body of the mite. Some of these cross-react to allergens from house-dust mites. Immediate antibody-mediated allergic reactions (wheals) have been elicited in infected persons, but not in healthy persons; immediate hypersensitivity of this type is thought to explain the observed far more rapid allergic skin response to reinfection seen in persons having been previously infected (especially having been infected within the previous year or two).[10] Because the host develops the symptoms as a reaction to the mites' presence over time, there is usually a 4– to 6-week incubation period after the onset of infestation. As noted, those previously infected with scabies and cured may exhibit the symptoms of a new infection in a much shorter period, as little as 1–4 days.[11]
Scabies is contagious, and can be spread by scratching an infected area, thereby picking up the mites under the fingernails, or through physical contact with a scabies-infected person for a prolonged period of time.[12] Scabies is usually transmitted by direct skin-to-skin physical contact. It can also be spread through contact with other objects, such as clothing, bedding, furniture, or surfaces with which a person infected with scabies might have come in contact.[13] Scabies mites can survive without a human host for 24 to 36 hours.[14] As with lice, scabies can be transmitted through sexual intercourse even if a latex condom is used, because it is transmitted from skin-to-skin at sites other than sex organs.[15]
Pathophysiology
The symptoms are caused by an allergic reaction of the host's body to mite proteins, though exactly which proteins remains a topic of study. The mite proteins are also present from the gut, in mite feces, which are deposited under the skin. The allergic reaction is both of the delayed (cell-mediated) and immediate (antibody-mediated) type, and involves IgE (antibodies, it is presumed, mediate the very rapid symptoms on re-infection).[9] The allergy-type symptoms (itching) continue for some days, and even several weeks, after all mites are killed. New lesions may appear for a few days after mites are eradicated. Nodular lesions from scabies may continue to be symptomatic for weeks after the mites have been killed.[9]
Diagnosis
 Magnified view of a burrowing trail of the scabies mite. The scaly patch on the left was caused by the scratching and marks the mite's entry point into the skin. The mite has burrowed to the top-right, where it can be seen as a dark spot at the end.
Magnified view of a burrowing trail of the scabies mite. The scaly patch on the left was caused by the scratching and marks the mite's entry point into the skin. The mite has burrowed to the top-right, where it can be seen as a dark spot at the end.Scabies may be diagnosed clinically in geographical areas where it is common when diffuse itching presents along with either lesions in two typical spots or there is itchiness of another household member.[16] The classical sign of scabies is the burrows made by the mites within the skin.[16] To detect the burrow the suspected area is rubbed with ink from a fountain pen or a topical tetracycline solution, which glows under a special light. The skin is then wiped with an alcohol pad. If the person is infected with scabies, the characteristic zigzag or "S" pattern of the burrow will appear across the skin; however, interpreting this test may be difficult, as the burrows are scarce and may be obscured by scratch marks.[16] A definitive diagnosis is made by finding either the scabies mites or their eggs and fecal pellets.[16] Searches for these signs involve either scraping a suspected area, mounting the sample in potassium hydroxide, and examining it under a microscope, or using dermoscopy to examine the skin directly.[3]
Differential diagnosis
Symptoms of early scabies infestation mirror other skin diseases, including dermatitis, syphilis, various urticaria-related syndromes, allergic reactions, and other ectoparasites such as lice and fleas.[17]
Prevention
Mass treatment programs that use topical permethrin or oral ivermectin have been effective in reducing the prevalence of scabies in a number of populations.[16] There is no vaccine available for scabies. The simultaneous treatment of all close contacts is recommended, even if they show no symptoms of infection (asymptomatic), to reduce rates of recurrence.[16] Asymptomatic infection is relatively common.[16] Objects in the environment pose little risk of transmission except in the case of crusted scabies, thus cleaning is of little importance.[16] Rooms used by those with crusted scabies require thorough cleaning.[18]
Management
A number of medications are effective in treating scabies, however treatment must often involve the entire household or community to prevent re-infection.[16] Options to improve itchiness include antihistamines.[19]
Permethrin
Permethrin is the most effective treatment for scabies,[20] and the treatment of choice.[16][21] It is applied from the neck down usually before bedtime and left on for about 8 to 14 hours, then showered off in the morning.[16] One application is normally sufficient for mild infections. For moderate to severe cases, another dose is applied 7–14 days later.[16][21][22] Permethrin causes slight irritation of the skin, but the sensation is tolerable.[3] The medication, however, is the most costly of topical treatments.[3]
Ivermectin
Ivermectin is an oral medication shown by many clinical studies to be effective in eradicating scabies, often in a single dose.[16][23] It is the treatment of choice for crusted scabies, and is often used in combination with a topical agent.[3][16] It has not been tested on infants and is not recommended for children under six years of age.[3]
Topical ivermectin preparations have been found to be effective for scabies in adults, and are attractive due to their low cost, ease of preparation, and low toxicity.[24] It has also been useful for sarcoptic mange (the veterinary analog of human scabies).[25]
Others
Other treatments include lindane, benzyl benzoate, crotamiton, malathion, and sulfur preparations.[3][16] Lindane is effective; however, concerns over potential neurotoxicity has limited its availability in many countries.[3] It is approved in the United States for use as a second-line treatment.[26] Sulfur ointments or benzyl benzoate are often used in the developing world due to their low cost;[3] 10% sulfur solutions have been shown to be effective,[27] and sulfur ointments are typically used for at least a week.[3] Crotamiton in limited studies has been found to be less effective than permethrin.[3] Crotamiton or a sulfur preparation is often recommended instead of permethrin for children, due to concerns over dermal absorption of permethrin.[16]
-

Day 4
-

Day 8 (treatment begins)
-

Day 12 (under treatment)
-

Healed
Epidemiology
Scabies is one of the three most common skin disorders in children, along with tinea and pyoderma.[16] The mites are distributed around the world and equally infect all ages, races, and socioeconomic classes in different climates.[8] Scabies is more often seen in crowded areas with unhygienic living conditions.[28] Globally as of 2009, it is estimated that 300 million cases of scabies occur each year, although various parties claim the figure is either over- or underestimated.[6][29] About 1–10% of the global population is estimated to be infected with scabies, but in certain populations, the infection rate may be as high as 50–80%.[30] Scabies is one of the three most common dermatological disorders in children.[30]
History
Scabies is an ancient disease. Archeological evidence from Egypt and the Middle East suggests that scabies was present as early as 494 BC.[11][31][clarification needed] The first recorded reference to scabies is believed to be from the Bible (Leviticus, the third book of Moses) ca. 1200 BC.[32] Later in fourth century BC, the ancient Greek philosopher Aristotle reported on "lice" that "escape from little pimples if they are pricked";[33] scholars believe this was actually a reference to scabies.[who?]
Nevertheless, it was Roman physician Celsus who is credited with naming the disease "scabies" and describing its characteristic features.[33] The parasitic etiology of scabies was later documented by the Italian physician Giovanni Cosimo Bonomo (1663–99 AD) in his famous 1687 letter, "Observations concerning the fleshworms of the human body."[33] With this (disputed) discovery,[clarification needed] scabies became one of the first diseases with a known cause.[11][31]
In other animals
Main articles: Sarcoptic mange and AcariasisScabies may occur in a number of domestic and wild animals; the mites that cause these infestations are of different scabies subspecies.[3] These subspecies can infest animals or humans that are not their usual hosts, but such infections do not last long.[3] Scabies-infected animals suffer severe itching and secondary skin infections. They often lose weight and become frail.[9]
The most frequently diagnosed form of scabies in domestic animals is sarcoptic mange, which is found on dogs. The scab mite Psoroptes is the mite responsible for mange. Scabies-infected domestic fowl suffer what is known as "scabies leg".[citation needed] Domestic animals that have gone feral and have no veterinary care are frequently afflicted with scabies and a host of other ailments.[34] Non-domestic animals have also been observed to suffer from scabies. Gorillas, for instance, are known to be susceptible to infection via contact with items used by humans.[35]
References
- ^ Mosby’s Medical, Nursing and Allied Health Dictionary, Fourth Edition, Mosby-Year Book Inc., 1994, p. 1395
- ^ Gates, Robert H. (2003). Infectious disease secrets (2. ed.). Philadelphia: Elsevier, Hanley Belfus. pp. 355. ISBN 9781560535430. http://books.google.com/?id=hYdw4vnanR0C&pg=PA355.
- ^ a b c d e f g h i j k l m n o p q r Hay RJ (2009). "Scabies and pyodermas—diagnosis and treatment". Dermatol Ther 22 (6): 466–74. doi:10.1111/j.1529-8019.2009.01270.x. PMID 19889132.
- ^ a b CDC web site > DPDx - Laboratory Identification of Parasites of Public Health Concern > Scabies [1]
- ^ a b "Scabies". DermNet NZ. New Zealand Dermatological Society Incorporated. http://www.dermnetnz.org/arthropods/pdf/scabies-dermnetnz.pdf.
- ^ a b c Bouvresse, S.; Chosidow, O. (Apr 2010). "Scabies in healthcare settings". Curr Opin Infect Dis 23 (2): 111–8. doi:10.1097/QCO.0b013e328336821b. PMID 20075729.
- ^ Hicks MI, Elston DM (2009). "Scabies". Dermatol Ther 22 (4): 279–92. doi:10.1111/j.1529-8019.2009.01243.x. PMID 19580575.
- ^ a b "DPDx—Scabies". Laboratory Identification of Parasites of Public Health Concern. CDC. http://www.dpd.cdc.gov/dpdx/HTML/Scabies.htm.
- ^ a b c d Walton S. F., Currie B. J. (April 2007). "Problems in Diagnosing Scabies, a Global Disease in Human and Animal Populations". Clinical Microbiology Reviews 20 (2): 268–79. doi:10.1128/CMR.00042-06. PMC 1865595. PMID 17428886. http://cmr.asm.org/cgi/content/full/20/2/268?view=long.
- ^ Clinical Microbiology Reviews, April 2007, p. 268-279, Vol. 20, No. 2 0893-8512/07/$08.00+0 doi:10.1128/CMR.00042-06 Problems in Diagnosing Scabies, a Global Disease in Human and Animal Populations online reference PMID 17428886
- ^ a b c Markell, Edward K.; John, David C.; Petri, William H. (2006). Markell and Voge's medical parasitology (9th ed.). St. Louis, Mo: Elsevier Saunders. ISBN 0-7216-4793-6.
- ^ Carol Turkington and Jeffrey S. Dover, M.D. (2006). The Encyclopedia of Skin and Skin Disorders. New York: Facts on File inc. ISBN 978-0-8160-6403-8.
- ^ Causes "Scabies Causes". WebMD. October 2010. http://www.emedicinehealth.com/scabies/page2_em.htm#Scabies Causes. Retrieved 2010-10-09.
- ^ Chosidow O (April 2006). "Clinical practices. Scabies". N. Engl. J. Med. 354 (16): 1718–27. doi:10.1056/NEJMcp052784. PMID 16625010.
- ^ "Scabies—Fast Facts". American Social Health Association. http://www.ashastd.org/learn/learn_scabies_facts.cfm. Retrieved 2010-10-09.
- ^ a b c d e f g h i j k l m n o p q Andrews RM, McCarthy J, Carapetis JR, Currie BJ (December 2009). "Skin disorders, including pyoderma, scabies, and tinea infections". Pediatr. Clin. North Am. 56 (6): 1421–40. doi:10.1016/j.pcl.2009.09.002. PMID 19962029.
- ^ Arlian LG (1989). "Biology, host relations, and epidemiology of Sarcoptes scabiei". Annu. Rev. Entomol. 34: 139–61. doi:10.1146/annurev.en.34.010189.001035. PMID 2494934. http://arjournals.annualreviews.org/doi/abs/10.1146/annurev.en.34.010189.001035?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dncbi.nlm.nih.gov.
- ^ "CDC—Prevention and Control—Scabies". Center for Disease Control and Prevention. http://www.cdc.gov/scabies/prevent.html. Retrieved 2010-10-09.
- ^ doi: 10.3949/ccjm.75.7.474 Cleveland Clinic Journal of Medicine July 2008 vol. 75 7 474–478 online link
- ^ Strong M, Johnstone PW (2007). Strong, Mark. ed. "Interventions for treating scabies". Cochrane Database Syst Rev (3): CD000320. doi:10.1002/14651858.CD000320.pub2. PMID 17636630.
- ^ a b "Scabies". Illinois Department of Public Health. January 2008. http://www.idph.state.il.us/public/hb/hbscab.htm. Retrieved 2010-10-07.
- ^ The Pill Book. Bantam Books. 2010. pp. 867–869. ISBN 978-0-553-59340-2.
- ^ "WHO -Water-related Disease". World Health Organization. http://www.who.int/water_sanitation_health/diseases/scabies/en/. Retrieved 2010-10-10.
- ^ Victoria J, Trujillo R (2001). "Topical ivermectin: a new successful treatment for scabies". Pediatr Dermatol 18 (1): 63–5. doi:10.1046/j.1525-1470.2001.018001063.x. PMID 11207977.
- ^ "Parasitology Research, Volume 78, Number 2". SpringerLink. http://www.springerlink.com/content/v84881343215g085/. Retrieved 2010-11-14.
- ^ "FDA Public Health Advisory: Safety of Topical Lindane Products for the Treatment of Scabies and Lice". Fda.gov. 2009-04-30. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm110845.htm. Retrieved 2010-11-14.
- ^ Jin-Gang A, Sheng-Xiang X, Sheng-Bin X, et al. (March 2010). "Quality of life of patients with scabies". J Eur Acad Dermatol Venereol 24 (10): 1187. doi:10.1111/j.1468-3083.2010.03618.x. PMID 20236379.
- ^ Green MS (1989). "Epidemiology of scabies". Epidemiol Rev 11 (1): 126–50. PMID 2509232. http://epirev.oxfordjournals.org/cgi/reprint/11/1/126.
- ^ Hicks, MI; Elston, DM (2009 Jul-Aug). "Scabies". Dermatologic therapy 22 (4): 279–92. doi:10.1111/j.1529-8019.2009.01243.x. PMID 19580575.
- ^ a b Andrews, RM.; McCarthy, J.; Carapetis, JR.; Currie, BJ. (Dec 2009). "Skin disorders, including pyoderma, scabies, and tinea infections". Pediatr Clin North Am 56 (6): 1421–40. doi:10.1016/j.pcl.2009.09.002. PMID 19962029.
- ^ a b "SCABIES HOMEPAGE". Stanford University. http://www.stanford.edu/group/parasites/ParaSites2005/Scabies/SCABIES.html. Retrieved 2010-10-09.
- ^ Leviticus 13:29-13:37
- ^ a b c Roncalli RA (July 1987). "The history of scabies in veterinary and human medicine from biblical to modern times". Vet. Parasitol. 25 (2): 193–8. doi:10.1016/0304-4017(87)90104-X. PMID 3307123. http://linkinghub.elsevier.com/retrieve/pii/0304-4017(87)90104-X.
- ^ "Bali Animal Welfare Association". http://www.bawabali.com/. Retrieved 2009-07-28.
- ^ [Uganda: Out of the Wild]. Transcript.
External links
- American Academy of Dermatology pamphlet on Scabies
- Scabies FAQ from the National Pediculosis Association
Infectious diseases – Parasitic disease: ectoparasitic infestation / arthropod (B85–B89, 132–134) Insecta Pediculus humanus corporis/Pediculus humanus capitis (Pediculosis, Head-louse infestation, Pediculosis corporis)Cimex (Cimicosis)Tunga penetrans (Tungiasis)Arachnida Trombidiformes: Trombicula (Trombiculosis, Chigger bite) · Demodex brevis/Demodex folliculorum (Demodicosis, Demodex mite bite) · Pyemotes herfsi · Cheyletiella (Cheyletiellosis)Sarcoptiformes: Sarcoptes scabiei (Scabies)Dermanyssus gallinae · Liponyssoides sanguineusTick infestationCrustacea Linguatula serrata (Linguatulosis) · Porocephalus crotali/Armillifer armillatus (Porocephaliasis)M: IFT
helm,arth (acar)
helm, arth (lice), zoon
helm, arth
Categories:- Parasitic infestations, stings, and bites of the skin
- Arthropod infestations
-













Wikimedia Foundation. 2010.