- Hemangioma
-
Hemangioma of Infancy Classification and external resources 
A small hemangioma of infancyICD-10 D18.0 (ILDS D18.010) ICD-9 228.0 ICD-O: M9120/0 DiseasesDB 30033 MedlinePlus 001459 eMedicine derm/201 MeSH D006391 A hemangioma of infancy is a benign self-involuting tumor (swelling or growth) of endothelial cells, the cells that line blood vessels. It usually appears during the first weeks of life and sometimes resolves by age 10. In more severe case hemangioma may have permanency, if not treated by a physician. Laser surgery is the most proactive way of removal in cases where patients are older than 10 years of age. In infancy, it is the most common tumor.[1] The word "hemangioma" comes from the Greek haema- (αίμα), "blood"; angeio (αγγείο), "vessel"; -oma (-ωμα), "tumor".
Contents
Terminology
The terminology used to define, describe and categorize vascular anomalies, abnormal lumps made up of blood vessels, has changed. The term hemangioma was originally used to describe any vascular tumor-like structure, whether it was present at or around birth or appeared later in life. Mulliken et al. categorized these conditions into two families: a family of self-involuting tumors, growing lesions that eventually disappear, and another family of malformations, enlarged or abnormal vessels present at birth and essentially permanent. The importance of this distinction is that it makes it possible for early-in-life differentiation between lesions that will resolve versus those that are permanent. Examples of permanent malformations include port-wine stains (capillary vascular malformation) and masses of abnormal swollen veins (venous malformations).[2]
Signs and symptoms
Hemangiomas are connected to the circulatory system and filled with blood. The appearance depends on location. If they are on the surface of the skin, they are reminiscent of a ripe strawberry (hence, they are sometimes referred to as "strawberry hemangiomas"); however, if they are just under the skin they present as a bluish swelling. Sometimes they grow in internal organs such as the liver or larynx. In most cases, hemangiomas will disappear over time. Some are formed during gestation; the most common are not congenital, but appear during the first few weeks of life. They are often initially misdiagnosed as a scratch or bruise; but the correct diagnosis becomes obvious with further growth. Typically, at the earliest phase in a superficial lesion, one will see a bluish red area with obvious blood vessels and surrounding pallor. Sometimes they present as a flat red or pink area. Hemangiomas are the most common childhood tumor, occurring in approximately ten percent of Caucasians, and are less prevalent in other ethnicities. Females are three to five times as likely to have hemangiomas as males. Hemangiomas are also more common in twin pregnancies. Approximately 80% are located on the face and neck, with the next most prevalent location being the liver.
-

Hemangioma on forehead showing signs of early regression
-

Hemangioma on the scalp of a two year old female, in the "rest stage"
-

Hemangioma of the liver as seen on ultrasound
-

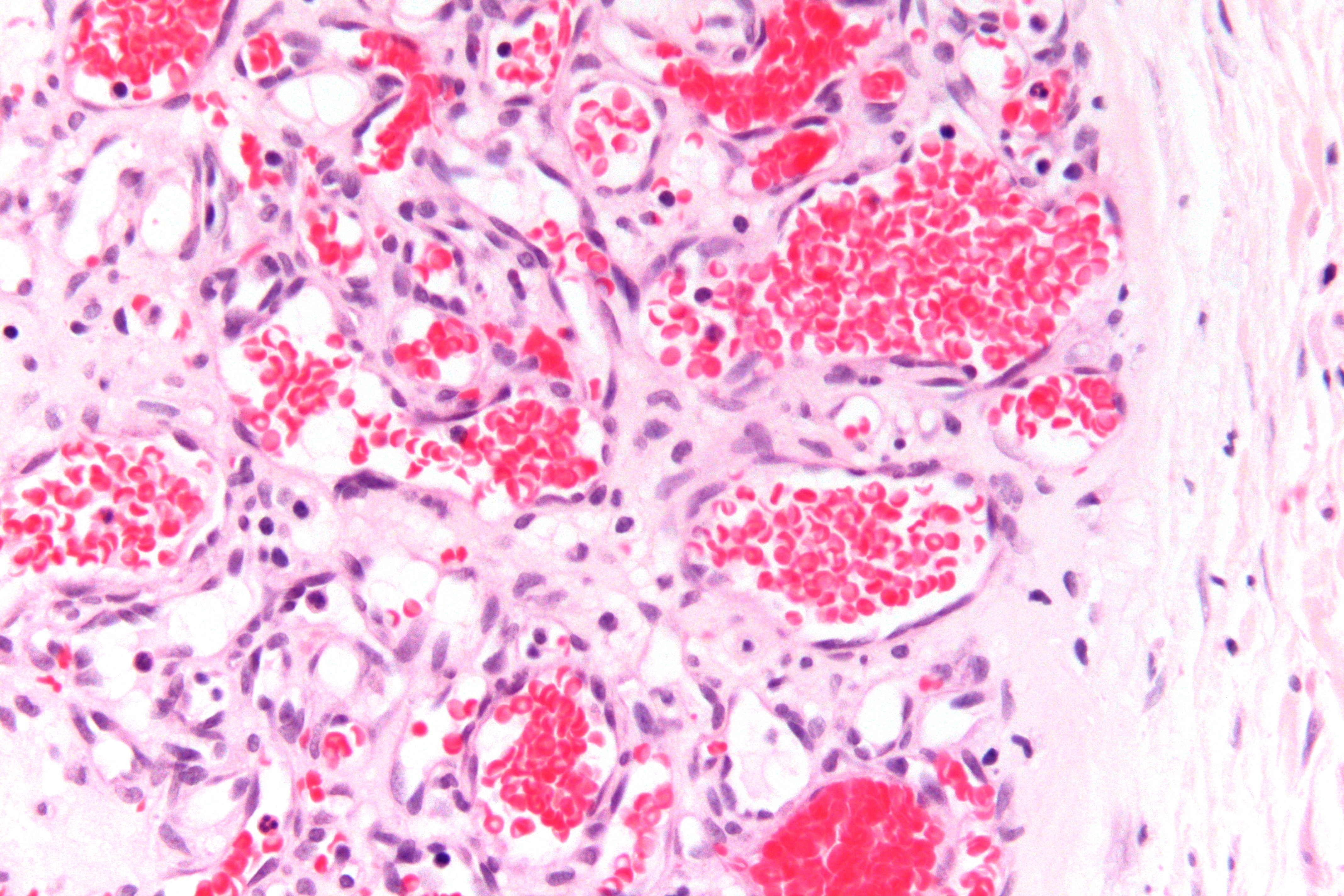
Micrograph of a capillary hemangioma. H&E stain.
Causes
The cause of hemangioma is currently unknown; however, several studies have suggested the importance of estrogen signaling in hemangioma proliferation. In 2007, a paper from the Stanford Children's Surgical Laboratory revealed that localized soft tissue hypoxia coupled with increased circulating estrogen after birth may be the stimulus.[3] There is also a hypothesis presented by researchers at Harvard and the University of Arkansas that maternal placenta embolizes to the fetal dermis during gestation resulting in hemangiomagenesis,.[4][5] However, researchers at Duke University conducted genetic analyses of single-nucleotide polymorphism in hemangioma tissue compared to the mother's DNA that contradicted this hypothesis.[6] More research is required in order to fully understand the explosive nature of hemangioma growth, which will hopefully yield targeted therapeutics to treat its most complicated presentations.
Complications
The vast majority of hemangiomas are not associated with complications. Hemangiomas may break down on the surface, called ulceration. If the ulceration is deep, significant bleeding may occur in rare occasions. Ulceration on the diaper area can be painful and problematic. If a hemangioma develops in the larynx, breathing can be compromised. A hemangioma can grow and block one of the eyes, causing an occlusion amblyopia. Very rarely, extremely large hemangiomas can cause high-output heart failure due to the amount of blood that must be pumped to excess blood vessels. Lesions adjacent to bone can also cause erosion of the bone.
The most frequent complaints about hemangiomas, however, stem from psychosocial complications: the condition can affect a person's appearance and can provoke attention and malicious reactions from others. Particular problems occur if the lip or nose is involved, as distortion can be difficult to treat surgically. The potential for psychological injury develops from school age onward. It is therefore important to consider treatment prior to school if adequate spontaneous improvement has not occurred.
Children with large segmental hemangiomas of the head and neck can be associated with a disorder called PHACES Syndrome.[7][8]
Treatment
Most hemangiomas disappear without treatment, leaving minimal or no visible marks. Large hemangiomas can leave visible skin changes secondary to severe stretching of the skin or damage to surface texture. When hemangiomas interfere with vision, breathing, or threaten significant cosmetic injury, they are usually treated.[9]
Until recently, the mainstay of treatment was oral corticosteroid therapy, but there are now alternative treatments. A published letter reported that the beta-blocker propranolol reduced severe hemangiomas in infants.[10] The topically applied beta blocker solution / gel Timolol, is also being trialled for small facial hemangiomas that do not justify systemic treatment.[11] Other treatments that have been used include interferon[12] or vincristine. They may be considered if first-line therapy fails.
Surgical removal is sometimes indicated, particularly if there has been delay in commencing treatment and structural changes have become irreversible. Surgery may also be necessary to correct distortion of facial features, again in the case of inadequate or failed early medical intervention. Blockage of the airway will often require a tracheostomy to be performed, which involves the insertion of an external airway through the front of the neck into the trachea below the level of the obstruction.
Smaller raised lesions are sometimes treated with injection of corticosteroid directly into the lesion. A pulsed dye laser can be useful for very early, flat, superficial lesions, if they appear in cosmetically significant areas or for those lesions that leave residual surface blood vessels in the case of incomplete resolution.[13] Sometimes a pulsed dye laser can be used to accelerate healing. Unfortunately, raised lesions or lesions under the skin do not respond to laser treatment. Ulceration will usually heal with topical medication and special dressings under medical supervision.
Prognosis
Hemangiomas go through three stages of development and decay:
- In the proliferation stage, a hemangioma grows very quickly. This stage can last up to twelve months.
- In the rest stage, there is very little change in a hemangioma's appearance. This usually lasts until the infant is one to two years old.
- In the involution phase, a hemangioma finally begins to diminish in size. 50% of lesions will have disappeared by 5 years of age, and the vast majority will have gone by 10
Notes
- ^ Haggstrom AN, Drolet BA, Baselga E, et al. (September 2006). "Prospective study of infantile hemangiomas: clinical characteristics predicting complications and treatment". Pediatrics 118 (3): 882–7. doi:10.1542/peds.2006-0413. PMID 16950977. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=16950977.
- ^ Mulliken JB, Glowacki J (March 1982). "Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics". Plast. Reconstr. Surg. 69 (3): 412–22. doi:10.1097/00006534-198203000-00002. PMID 7063565.
- ^ Kleinman ME, Greives MR, Churgin SS, et al. (December 2007). "Hypoxia-induced mediators of stem/progenitor cell trafficking are increased in children with hemangioma". Arterioscler. Thromb. Vasc. Biol. 27 (12): 2664–70. doi:10.1161/ATVBAHA.107.150284. PMID 17872454. http://atvb.ahajournals.org/cgi/content/full/27/12/2664.
- ^ Barnés CM, Huang S, Kaipainen A, et al. (December 2005). "Evidence by molecular profiling for a placental origin of infantile hemangioma". Proc. Natl. Acad. Sci. U.S.A. 102 (52): 19097–102. doi:10.1073/pnas.0509579102. PMC 1323205. PMID 16365311. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1323205.
- ^ North PE, Waner M, Brodsky MC (April 2002). "Are infantile hemangiomas of placental origin?". Ophthalmology 109 (4): 633–4. doi:10.1016/S0161-6420(02)01071-0. PMID 11949625. http://linkinghub.elsevier.com/retrieve/pii/S0161-6420(02)01071-0.
- ^ Pittman KM, Losken HW, Kleinman ME, et al. (November 2006). "No evidence for maternal-fetal microchimerism in infantile hemangioma: a molecular genetic investigation". J. Invest. Dermatol. 126 (11): 2533–8. doi:10.1038/sj.jid.5700516. PMID 16902414. http://www.nature.com/jid/journal/v126/n11/abs/5700516a.html.
- ^ Oza VS, Wang E, Berenstein A, et al. (April 2008). "PHACES association: a neuroradiologic review of 17 patients". AJNR Am J Neuroradiol 29 (4): 807–13. doi:10.3174/ajnr.A0937. PMID 18223093. http://www.ajnr.org/cgi/pmidlookup?view=long&pmid=18223093.
- ^ Heyer GL, Dowling MM, Licht DJ, et al. (February 2008). "The cerebral vasculopathy of PHACES syndrome". Stroke 39 (2): 308–16. doi:10.1161/STROKEAHA.107.485185. PMID 18174492. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=18174492.
- ^ Hunzeker C, Geronemus R. "Treatment of Superficial Infantile Hemangiomas of the Eyelid Using the 595-nm Pulsed Dye Laser" Dermatol. Surg. 36(5):590-597 2010 [1]
- ^ Léauté-Labrèze C et al. (June 2008). "Propranolol for Severe Hemangiomas of Infancy". New England Journal of Medicine 358 (24): 2649–2651. doi:10.1056/NEJMc0708819. PMID 18550886. http://content.nejm.org/cgi/content/full/358/24/2649.
- ^ (Guo S, Ni N. Topical treatment for Capillary hemangioma of the eyelid using topical beta-blocker solution. Archives of Ophthalmology. 2010;128(2):255-256. Arch Dermatol. 2010 May;146(5):564-5.Topical timolol gel for infantile hemangiomas: a pilot study. Pope E, Chakkittakandiyil A.)
- ^ Wilson MW, Hoehn ME, Haik BG, Rieman M, Reiss U (May 2007). "Low-dose cyclophosphamide and interferon alfa 2a for the treatment of capillary hemangioma of the orbit". Ophthalmology 114 (5): 1007–11. doi:10.1016/j.ophtha.2006.11.031. PMID 17337066. http://linkinghub.elsevier.com/retrieve/pii/S0161-6420(06)01612-5.
- ^ Rizzo C, Brightman L, Chapas A, Hale E, Cantatore-Francis J, Bernstein L, Geronemus R. "Outcomes of Childhood Hemangiomas Treated with the Pulsed Dye Laser with Dynamic Cooling: A Retrospective Chart Analysis" Dermatol. Surg. 35(12):1947-1954. 2009 [2]
External links
- Hemangioma - Children's Hospital Los Angeles
- Hemangioma - at Web MD
- Hemangioma - Children's Hospital Boston
- Humpath #1990 (Pathology images) at humpath.com
- MedlinePlus Encyclopedia Hemangioma
- Hepatic Hemangioma at medicinenet.com
- Haemangiomas of infancy at rch.org.au
- Liver Hemangioma at USUHS - MedPix
Vascular tissue neoplasm (ICD-O 9120–9179) (C49+C46/D18, 171+176/215) Blood Hemangioma/hemangiosarcoma · Blue rubber bleb nevus syndrome · Hemangioendothelioma (Infantile hemangioendothelioma · Endovascular papillary hemangioendothelioma · Epithelioid hemangioendothelioma · Spindle cell hemangioendothelioma · Composite hemangioendothelioma · Proliferating angioendotheliomatosis · Retiform hemangioendothelioma) · Hemangiopericytoma · Angiokeratoma · Capillary hemangioma (Hemangioblastoma) · Cavernous hemangioma · Venous lakeKaposi's sarcoma: African cutaneous Kaposi sarcoma · African lymphadenopathic Kaposi sarcoma · AIDS-associated Kaposi sarcoma · Classic Kaposi sarcoma · Immunosuppression-associated Kaposi sarcoma · Kaposiform hemangioendotheliomaAngioma serpiginosum · Cherry angioma · Glomeruloid hemangioma · Microvenular hemangioma · Spider angioma · Targetoid hemosiderotic hemangioma · Tufted angioma · Universal angiomatosis
Pyogenic granulomaLymphatic Lymphangioma/lymphangiosarcoma · PEComa (Lymphangioleiomyomatosis) · Cystic hygroma · Lymphangioma circumscriptumEither Categories:- Benign neoplasms
- Dermal and subcutaneous growths
-




Wikimedia Foundation. 2010.