- Ingrown nail
-
Ingrown nail Classification and external resources 
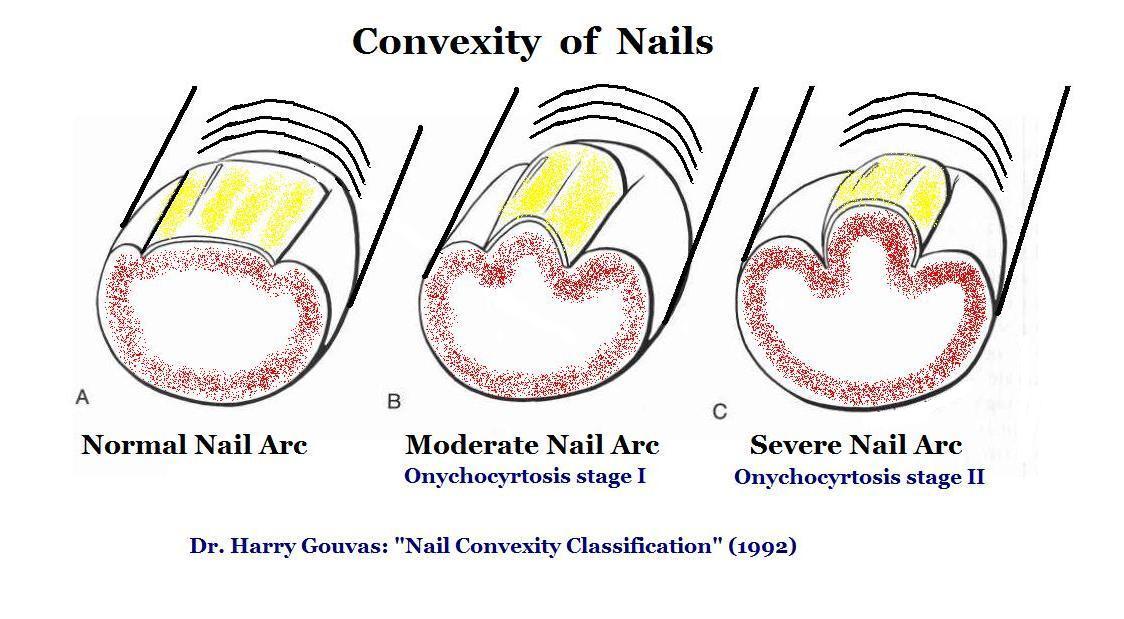
An ingrown toenailICD-10 L60.0 ICD-9 703.0 DiseasesDB 29440 eMedicine emerg/593 ped/942 Onychocryptosis (from Greek ὄνυξ onyx "nail" + κρυπτός kryptos "hidden"), also known as an ingrown toenail, or unguis incarnatus[1] is a common form of nail disease. It is an often painful condition in which the nail grows so that it cuts into one or both sides of the paronychium or nail bed. The common opinion is that the nail enters inside the paronychium but an ingrown toenail may be overgrown toe skin.[2] The disease starts from a microbial inflammation of the paronychium, secondary a to granuloma, and the result is a nail buried inside the granuloma.[3] While ingrown nails can occur in both the nails of the hand and feet, they occur most commonly with the toenails. A true ingrowing toenail, or onychocryptosis, is caused by the actual penetration of the flesh by a sliver of nail.[4] This should not be confused with other painful nail conditions such as involuted nails, or the presence of small corns, callus or debris down the nail sulci (grooves either side of the nail plate)or under the nail plate itself.[5] Also it should not be confused with a similar nail disorder, onychocyrtosis (from Greek ὄνυξ onyx "nail" + κυρτός kyrtos "convex") or convex nail.[3]
Signs and symptoms
 Nail Arc Convexity
Nail Arc Convexity
Symptoms of an ingrown nail include pain along the margins of the nail (caused by hypergranulation that occurs around the aforementioned region), worsening of pain when wearing tight footwear, and sensitivity to pressure of any kind, even the weight of bedsheets. Bumping of an affected toe can produce sharp, even excruciating, pain as the tissue is punctured further by the nail. By the very nature of the condition, ingrown nails become easily infected unless special care is taken to treat the condition early on and keep the area clean. Signs of infection include redness and swelling of the area around the nail, drainage of pus, and watery discharge tinged with blood. The main symptom is swelling at the base of the nail on the side the nail is ingrowing (may be both sides).
Causes
The main cause of onychocryptosis is unsuitable footwear, including shoes with inadequate toe-box room and tight stockings that apply top and or side pressures. Less frequent causes include the damp atmosphere of enclosed shoes, softening the nail-plate and swelling the epidermal keratin, which eventually increases the convex arch permanently; genetics; and trauma and disease. Improper cutting may cause the nail to cut into the side-fold skin from growth and impact, whether or not the nail is "ingrown" (true onychocryptosis). The nail bends inwards or upwards depending on the angle of its cut. If the cutting tool, such as scissors, is in an attitude where the lower blade is closer to the toe than the upper blade, that will cause the toenail to grow from its base upwards, and vice versa. The process is visible along the nail as it grows, appearing as a warp advancing to the end of the nail. The upper corners turn more easily than the center of the nail tip. As people cut their nails by holding the tool always in the same angle, they induce these conditions by accident; as the nail turns closer to the skin, it becomes harder to fit the lower blade in the right attitude under the nail. When cutting a nail, it is not just the correct angle that is important, but also how short it is cut. A shorter cut will bend the nail more, unless the cut is even on both top and bottom of the nail.
Causes may include:
- Bad nail-care, including cutting the nail too short, rounded off at the tip or peeled off at the edges instead of being cut straight across[6]
- Ill-fitting shoes, as those that are too narrow or too short can cause bunching of the toes in the developmental stages of the foot (frequently in those under 21), causing the nail to curl and dig into the skin
- Trauma to the nail plate or toe, which can occur by stubbing the toenail, dropping things on the toe or going through the end of the shoes (as during sports or other vigorous activity), can cause the flesh to become injured and the nail to grow irregularly and press into the flesh
- Predisposition, such as abnormally shaped nail beds, nail deformities caused by diseases, or a genetic susceptibility
- Ingrown toenails may be the result of a bacterial infection, treatable with antibiotics. See Treatments.
A more physiologically sound description is that an ingrown toenail is actually too much skin around the nail ("overgrown toeskin")—the nail is not the problem. Vandenbos and Bowers theorized that pressure necrosis of the soft tissues surrounding the nail due to weight-bearing is the primary cause of ingrowing toenails. They wrote "the term 'ingrown toenail' is unfortunate in that it incriminates the nail as the causative factor and is responsible for the fact that most operative and conservative treatments are directed toward the nail. It is our thesis that persons who develop this condition have an unusually wide area of tissue medial and lateral to the nail and that with weight bearing this tissue tends to bulge up around the nail. When such persons trim the nail in a curved or rounded fashion instead of straight across, further bulging of soft tissue is allowed, and as the nail grows out, pressure necrosis of soft tissue occurs. If our thesis that the fault lies not with the nail but with an excess of soft tissue is correct, treatment by removal of a segment of nail is not rational. It increases the relative amount of soft tissue and predisposes to recurrence and at the same time inept attempts to remove some nail matrix lead to faulty regrowth of the nail. The logical conclusion is that soft tissue should be excised, so that with weight bearing there will be no tissue to bulge up across the nail.".[7] One study compared patients with ingrown toenails to healthy controls and found no difference in the shape of toenails between patients and controls and suggested that treatment should not be based on the correction of a non-existent nail deformity.[8] Ingrown toenails are caused by weight-bearing (activities such as walking, etc.) in patients that have too much soft tissue (skin) on the sides of the nail. Weight bearing causes this excessive amount of skin to bulge up along the sides of the nail. The pressure on the skin around the nail results in the tissue being damaged, resulting in swelling, redness and infection. In the past (and still today) the most common treatments are mainly directed at the nail (paradigm paralysis). Treatments often include removal of part or all of the nail. But since the nail is normal and the problem of too much skin around the nail is not treated, this often results in the problem returning or in deformity/mutilation of the nail.
Prevention
The most common place for ingrown nails is in the big toe, but ingrowth can occur on any nail. Ingrown nails can be avoided by cutting nails straight across; nails should not be cut along a curve, nor should they be cut too short. The important thing to avoid is cutting the nail shorter than the flesh around it. Footwear which is too small or too narrow, or with too shallow a 'toe box', will exacerbate any underlying problem with a toenail. It may not be so critical that the nails be cut perfectly 'straight across' as this may imply that they be squared at the corners. Sharp square corners may be uncomfortable and cause snagging on socks. Proper cutting leaves the leading edge of the nail free of the flesh, precluding it from growing into the toe. Filing of the corner is reasonable. Some nails require cutting of the corners far back to remove edges that dig into the flesh, this may be done as a partial wedge resection at a podiatrist's office. Ingrown toe nails can be caused by injury, commonly blunt trauma where the flesh is pressed against the nail causing a small cut that swells. Also, injury to the nail can cause it to grow abnormally, making it wider or thicker than normal or even bulged or crooked. Stubbing the toenail, dropping things on the toe and 'going through the end of your shoes' in sports are common injuries to the digits. Injuries to the toes can be prevented by wearing properly fitting shoes, especially when working or playing. One myth is that a V should be cut in the end of the ingrown nail. The reasoning of is that if one cuts a V in the nail, the edge of the nail will grow together as the nail grows out. This does not happen - the shape of the nail is determined by the growing area at the base of the toe and not by the end of the nail. A notch does not alleviate an ingrown toenail, and may do harm if cut too deeply.[6]
Management
 Toothpick segment used to prevent ingrowing
Toothpick segment used to prevent ingrowingThe treatment of an ingrown toenail partly depends on how severe it is.[9] In mild to moderate cases conservative treatment with warm water soaks, antibacterial ointment and using dental floss or a gutter splint to provide a tract along which the nail may grow, may suffice.[9] If conservative treatment of a minor ingrown toenail does not succeed or if the ingrown toenail is severe, surgical management is recommended.[9]
Surgery
Main article: Surgical treatment of ingrown toe nails A toe post wedge resection with an image of the nail removed
A toe post wedge resection with an image of the nail removedThe initial surgical approach is typically a partial avulsion of the lateral nail plate known as a wedge resection or a complete removal of the toenail.[9] If the ingrown toenail reoccurs despite this treatment, destruction of the germinal matrix with phenol is recommended.[9] Topical antibiotics may be used post procedure but oral antibiotics are not recommended as they may delay healing.[9]
References
- ^ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders. p. 789. ISBN 0-7216-2921-0.
- ^ Chapeskie H (2008). "Ingrown toenail or overgrown toe skin?". Canadian Family Physician 54 (11): 1561–2. PMC 2592332. PMID 19005128. http://www.cfp.ca/cgi/content/full/54/11/1561.
- ^ a b Harry Gouvas: Wedge Resection (Lateral Onychoplasty) as the method of choice for Ingrown Toenail". Orthopaedic Medical Congress in Athens, 14 Oct, 2004, paper, 148
- ^ Ingrown Toenail: http://www.nhs.uk/conditions/ingrown-toenail/Pages/Introduction.aspx
- ^ Ingrown Toenail: http://www.walkwithoutpain.com.au/what-is-onychophosis-subungal-corns-corns-under-the-toenails-podiatry-faqs-21/
- ^ a b "FootPhysicians.com Information on Ingrown Toenails". http://www.footphysicians.com/footankleinfo/ingrown-toenail.htm. Retrieved 31 March 2010.
- ^ http://www.ingrowntoenails.ca/images/vanderbos/article.htm
- ^ Pearson HJ, Bury RN, Wapples J, Watkin DF (November 1987). "Ingrowing toenails: is there a nail abnormality? A prospective study". J Bone Joint Surg Br 69 (5): 840–2. PMID 3680356. http://www.jbjs.org.uk/cgi/reprint/69-B/5/840.
- ^ a b c d e f Heidelbaugh, JJ; Lee, H (2009 Feb 15). "Management of the ingrown toenail.". American family physician 79 (4): 303–8. PMID 19235497.
- Chapeskie H (2008). "Ingrown toenail or overgrown toe skin?". Canadian Family Physician 54 (11): 1561–1562. PMC 2592332. PMID 19005128. http://www.cfp.ca/cgi/content/full/54/11/1561?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&author1=Chapeskie&andorexactfulltext=and&searchid=1&FIRSTINDEX=0&sortspec=relevance&resourcetype=HWCIT.
- Vandenbos KQ, Bowers WP (1959). "Ingrown toenail: a result of weight bearing on soft tissue". US Armed Forces Medical Journal 10 (10): 1168–1173. http://www.ingrowntoenails.ca/images/vanderbos/article.htm.
- Pearson HJ, Bury RN, Wapples J, Watkin DF (1987). "Ingrowing toenails: is there a nail abnormality? A prospective study". J Bone Joint Surg Br 69 (5): 840–842. PMID 3680356. http://www.jbjs.org.uk/cgi/reprint/69-B/5/840.
- Aksakal AB, Ozsoy E, Gürer M (2003). "Silicone gel sheeting for the management and prevention of onychocryptosis". Dermatol Surg 29 (3): 261–4. doi:10.1046/j.1524-4725.2003.29061.x. PMID 12614420. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=1076-0512&date=2003&volume=29&issue=3&spage=261.
- Boll OF (1945). "Surgical correction of ingrowing toenails". J Natl Assoc Chiroprod. 35: 8–9.
- Kominsky SJ, Daniels MD (2000). "A modified approach to the phenol and alcohol chemical partial matrixectomy". J Am Podiatr Med Assoc 90 (4): 208–10. PMID 10800276. http://www.japmaonline.org/cgi/pmidlookup?view=long&pmid=10800276.
- Rounding C, Bloomfield S (2005). Rounding, Catherine. ed. "Surgical treatments for ingrowing toenails". Cochrane Database Syst Rev (2): CD001541. doi:10.1002/14651858.CD001541.pub2. PMID 15846620.
- Boberg JS, Frederiksen MS, Harton FM (2002). "Scientific analysis of phenol nail surgery". J Am Podiatr Med Assoc 92 (10): 575–9. PMID 12438504. http://www.japmaonline.org/cgi/pmidlookup?view=long&pmid=12438504.
Disorders of skin appendages (L60–L75, 703–706) Nail other: Ingrown nail · Anonychiaungrouped: Paronychia (Acute paronychia, Chronic paronychia ) · Chevron nail · Congenital onychodysplasia of the index fingers · Green nails · Half and half nails · Hangnail · Hapalonychia · Hook nail · Lichen planus of the nails · Longitudinal erythronychia · Malalignment of the nail plate · Median nail dystrophy · Mees' lines · Melanonychia · Muehrcke's lines · Nail–patella syndrome · Onychoatrophy · Onychocryptosis · Onycholysis · Onychomadesis · Onychomatricoma · Onychomycosis · Onychophosis · Onychoptosis defluvium · Onychorrhexis · Onychoschizia · Platonychia · Pincer nails · Plummer's nail · Psoriatic nails · Pterygium inversum unguis · Pterygium unguis · Purpura of the nail bed · Racquet nail · Red lunulae · Shell nail syndrome · Splinter hemorrhage · Spotted lunulae · Staining of the nail plate · Stippled nails · Subungual hematoma · Terry's nails · Twenty-nail dystrophyHair noncicatricial alopecia: Alopecia/Alopecia areata (Alopecia totalis, Alopecia universalis, Ophiasis)
Androgenic alopecia (male-pattern baldness) · Hypotrichosis · Telogen effluvium · Traction alopecia · Lichen planopilaris · Trichorrhexis nodosa · Alopecia neoplastica · Anagen effluvium · Alopecia mucinosacicatricial alopecia: Pseudopelade of Brocq · Central centrifugal cicatricial alopecia · Pressure alopecia · Traumatic alopecia · Tumor alopecia · Hot comb alopecia · Perifolliculitis capitis abscedens et suffodiens · Graham-Little syndrome · Folliculitis decalvansHirsutism · Acquired generalized hypertrichosis · Generalized congenital hypertrichosis · Localized acquired hypertrichosis · Localized congenital hypertrichosis · Patterned acquired hypertrichosis · Prepubertal hypertrichosis · X-linked hypertrichosisAcneAcne vulgaris · Acne conglobata · Acne miliaris necrotica · Tropical acne · Infantile acne/Neonatal acne · Excoriated acne · Acne fulminans · Acne medicamentosa (e.g., steroid acne) · Halogen acne (Iododerma, Bromoderma, Chloracne) · Oil acne · Tar acne · Acne cosmetica · Occupational acne · Acne aestivalis · Acne keloidalis nuchae · Acne mechanica · Acne with facial edema · Pomade acne · Acne necrotica · Blackhead · Lupus miliaris disseminatus facieiPerioral dermatitis (Granulomatous perioral dermatitis) · Phymatous rosacea (Rhinophyma, Blepharophyma, Gnathophyma, Metophyma, Otophyma) · Papulopustular rosacea · Lupoid rosacea · Erythrotelangiectatic rosacea · Glandular rosacea · Gram-negative rosacea · Steroid rosacea · Ocular rosacea · Persistent edema of rosacea · Rosacea conglobata · variants (Periorificial dermatitis, Pyoderma faciale)UngroupedGranulomatous facial dermatitis · Idiopathic facial aseptic granuloma · Periorbital dermatitis · SAPHO syndromeFollicular cystsFolliculitis (Folliculitis nares perforans, Tufted folliculitis) · Pseudofolliculitis barbae
Hidradenitis (Hidradenitis suppurativa, Recurrent palmoplantar hidradenitis, Neutrophilic eccrine hidradenitis)UngroupedAcrokeratosis paraneoplastica of Bazex · Acroosteolysis · Bubble hair deformity · Disseminate and recurrent infundibulofolliculitis · Erosive pustular dermatitis of the scalp · Erythromelanosis follicularis faciei et colli · Hair casts · Hair follicle nevus · Intermittent hair–follicle dystrophy · Keratosis pilaris atropicans · Kinking hair · Koenen's tumor · Lichen planopilaris · Lichen spinulosus · Loose anagen syndrome · Menkes kinky hair syndrome · Monilethrix · Parakeratosis pustulosa · Pili (Pili annulati · Pili bifurcati · Pili multigemini · Pili pseudoannulati · Pili torti) · Pityriasis amiantacea · Plica neuropathica · Poliosis · Rubinstein–Taybi syndrome · Setleis syndrome · Traumatic anserine folliculosis · Trichomegaly · Trichomycosis axillaris · Trichorrhexis (Trichorrhexis invaginata · Trichorrhexis nodosa) · Trichostasis spinulosa · Uncombable hair syndrome · Wooly hair · Wooly hair nevusSweat glands Miliaria (Colloid milium • Miliaria crystalline • Miliaria profunda • Miliaria pustulosa • Miliaria rubra • Occlusion miliaria • Postmiliarial hypohidrosis), Granulosis rubra nasi, Ross’ syndrome, Anhidrosis, Hyperhidrosis (Generalized, Gustatory, Palmoplantar)Categories:- Conditions of the skin appendages


Wikimedia Foundation. 2010.