- Mucormycosis
-
Mucormycosis Classification and external resources 
ICD-10 B46.0-B46.5 ICD-9 117.7 DiseasesDB 31759 MeSH D009091 Mucormycosis is the term used to describe fungal infections caused by fungi in the order Mucorales,[1]:328 and species in the Mucor, Rhizopus, Absidia and Cunninghamella genera are most often implicated.[2][3] This disease is often characterized by hyphae growing in and around vessels.[4]
"Mucormycosis" and "Zygomycosis" are sometimes used interchangeably.[5] However, zygomycota has been identified as polyphyletic, and is not included in modern fungal classification systems.
Also, while Zygomycosis includes Entomophthorales, mucormycosis excludes this group.
Contents
Signs and symptoms
Mucormycosis frequently involves the sinuses, brain, or lungs as the areas of infection. While oral or cerebral mucormycosis are the most common types of the disease, this infection can also manifest in the gastrointestinal tract, skin, and in other organ systems.[6] In rare cases, the maxilla may be affected by mucormycosis.[7] The rich vascularity of maxillofacial areas usually prevents fungal infections, although more virulent fungi, such as those responsible for mucormycosis, can often overcome this difficulty.[7]
There are several key signs which point towards mucormycosis. One such sign is fungal invasion into the vascular network which results in thrombosis and death of surrounding tissue by loss of blood supply.[8] If the disease involves the brain then symptoms may include a one-sided headache behind the eyes, facial pain, fevers, nasal stuffiness that progresses to black discharge, and acute sinusitis along with swelling of the eye.[9] Affected skin may appear relatively normal during the earliest stages of infection. This skin quickly progresses to an erythemic (reddening, occasionally with edema) stage, before eventually turning black due to necrosis.[8] In other forms of mucormycosis, such as pulmonary, cutaneous, or disseminated mucormycosis, symptoms may also include dyspnea (difficulty breathing), and persistent cough; in cases of necrosis, symptoms include nausea and vomiting, coughing blood, and abdominal pain.[6][9]
Diagnosis
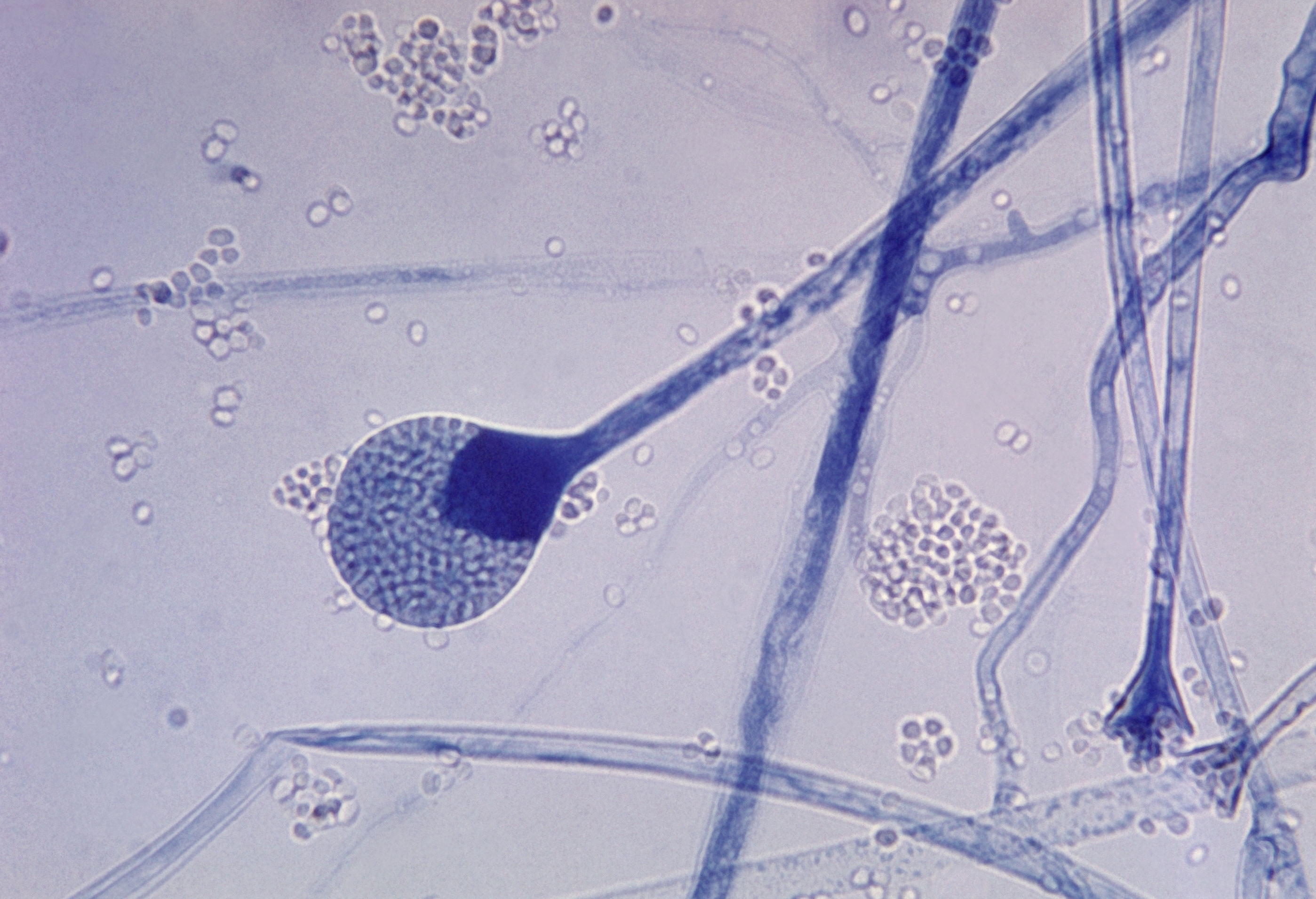
 This photomicrograph reveals a mature sporangium of a Mucor sp. fungus, which can be responsible for mucormycosis
This photomicrograph reveals a mature sporangium of a Mucor sp. fungus, which can be responsible for mucormycosis
As swabs of tissue or discharge are generally unreliable, the diagnosis of Mucormycosis tends to be established by a biopsy specimen of the involved tissue.
Treatment
If mucormycosis is suspected, prompt amphotericin B therapy should be administered due to the rapid spread and mortality rate of the disease. Amphotericin B (which works by damaging the cell walls of the fungi) is usually administered for a further 4–6 weeks after initial therapy begins to ensure eradication of the infection. Posaconazole has been shown to be effective against mucormycosis, perhaps more so than amphotericin B, but has not yet replaced it as the standard of care.
After administration of either amphotericin B or Posaconazole, surgical removal of the "fungus ball" is indicated. The disease must be monitored carefully for any signs of reemergence.[6][10]
Surgical therapy can be very drastic, and in some cases of Rhinocerebral disease removal of infected brain tissue may be required. In some cases surgery may be disfiguring because it may involve removal of the palate, nasal cavity, or eye structures.[9] Surgery may be extended to more than one operation.[6] It has been hypothesised that hyperbaric oxygen may be beneficial as an adjunctive therapy because higher oxygen pressure increases the ability of neutrophils to kill the organism.[8]
Prognosis
In most cases, the prognosis of mucormycosis is poor and has varied mortality rates depending on its form and severity. In the rhinocerebral form, the mortality rate is between 30% and 70%, whereas disseminated mucormycosis presents with the highest mortality rate in an otherwise healthy patient, with a mortality rate of up to 90%.[8] Patients with AIDS have a mortality rate of almost 100%.[10] Possible complications of mucormycosis include the partial loss of neurological function, blindness and clotting of brain or lung vessels.[9]
Epidemiology
Mucormycosis is a very rare infection, and as such it is hard to note histories of patients and incidence of the infection.[6] However, one American oncology center revealed that mucormycosis was found in 0.7% of autopsies and roughly 20 patients per every 100,000 admissions to that center.[10] In the United States, mucormycosis was most commonly found in rhinocerebral form, almost always with hyperglycemia and metabolic acidosis.[11] In most cases the patient is immunocompromised, although rare cases have occurred in which the subject was not; these are usually due to a traumatic inoculation of fungal spores. Internationally, mucormycosis was found in 1% of patients with acute leukemia in an Italian review.[6]
A cluster of infections occurred in the wake of the 2011 Joplin tornado. As of July 19, a total of 18 suspected cases of cutaneous mucormycosis had been identified, of which 13 were confirmed. A confirmed case was defined as 1) necrotizing soft-tissue infection requiring antifungal treatment or surgical debridement in a person injured in the tornado, 2) with illness onset on or after May 22, and 3) positive fungal culture or histopathology and genetic sequencing consistent with a Mucormycete. No additional cases have been reported since June 17. Ten patients required admission to an intensive-care unit, and five died.[12]
Cutaneous mucormycosis has been reported after previous natural disasters; however, this is the first known cluster occurring after a tornado. None of the infections were found in persons cleaning up debris. Health-care providers should consider environmental fungi as potential causes of necrotizing soft-tissue infections in patients injured during tornados and initiate early treatment for suspected infections.[13]
Predisposing factors for mucormycosis include AIDS, diabetes, malignancies such as lymphomas, renal failure, organ transplant, long term corticosteroid and immunosuppressive therapy, cirrhosis energy malnutrition,[6][7] and Deferoxamine therapy. Despite this, however, there have been cases of mucormycosis reported with no apparent predisposing factors present.[11]
References
- ^ James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 0-7216-2921-0.
- ^ Rinaldi M.G. (1989). "Zygomycosis". Infect Dis Clin North Am 3: 19–41.
- ^ Lee F.Y.; Mossad S.B.; Adal K.A. (1999). "Pulmonary mucormycosis: the last 30 years". Arch Intern Med 159: 1301–9. doi:10.1001/archinte.159.12.1301. PMID 10386506.
- ^ ADA.
- ^ Staff Springfield News-Leader (10 June 2011) "Aggressive fungus strikes Joplin tornado victims" Seattle PI, Hearst Communications Inc.
- ^ a b c d e f g Nancy F Crum-Cianflone, MD MPH. "Mucormycosis". eMedicine. http://www.emedicine.com/med/topic1513.htm. Retrieved 2008-05-19.
- ^ a b c Auluck A (2007). "Maxillary necrosis by mucormycosis. a case report and literature review" (PDF). Med Oral Patol Oral Cir Bucal 12 (5): E360–4. PMID 17767099. http://www.medicinaoral.com/medoralfree01/v12i5/medoralv12i5p360.pdf. Retrieved 2008-05-19.
- ^ a b c d Spellberg B, Edwards J, Ibrahim A (2005). "Novel perspectives on mucormycosis: pathophysiology, presentation, and management". Clin. Microbiol. Rev. 18 (3): 556–69. doi:10.1128/CMR.18.3.556-569.2005. PMC 1195964. PMID 16020690. http://cmr.asm.org/cgi/content/full/18/3/556. Full text at PMC: 1195964
- ^ a b c d "MedlinePlus Medical Encyclopedia: Mucormycosis". http://www.nlm.nih.gov/medlineplus/ency/article/000649.htm. Retrieved 2008-05-19.
- ^ a b c Rebecca J. Frey, PhD. "Mucormycosis". Health A to Z. http://www.healthatoz.com/healthatoz/Atoz/clients/haz/general/custom/default.jsp. Retrieved 2008-05-19.
- ^ a b Roden MM, Zaoutis TE, Buchanan WL, et al (September 2005). "Epidemiology and outcome of Mucormycosis: a review of 929 reported cases". Clin. Infect. Dis. 41 (5): 634–53. doi:10.1086/432579. PMID 16080086.
- ^ Rare Infection Strikes Victims of a Tornado in Missouri
- ^ MMWR Weekly July 29, 2011 / 60(29);992
Infectious diseases · Mycoses and Mesomycetozoea (B35–B49, 110–118) Superficial and
cutaneous
(dermatomycosis):
Tinea=skin;
Piedra (exothrix/
endothrix)=hairBy locationTinea barbae/Tinea capitis (Kerion) · Tinea corporis (Ringworm, Dermatophytid) · Tinea cruris · Tinea manuum · Tinea pedis (Athlete's foot) · Tinea unguium/Onychomycosis (White superficial onychomycosis · Distal subungual onychomycosis · Proximal subungual onychomycosis)
Tinea corporis gladiatorum · Tinea faciei · Tinea imbricata · Tinea incognito · FavusBy organismEpidermophyton floccosum · Microsporum canis · Microsporum audouinii · Trichophyton interdigitale/mentagrophytes · Trichophyton tonsurans · Trichophyton schoenleini · Trichophyton rubrumOtherHortaea werneckii (Tinea nigra) · Piedraia hortae (Black piedra)Subcutaneous,
systemic,
and opportunisticDimorphic
(yeast+mold)Coccidioides immitis/Coccidioides posadasii (Coccidioidomycosis, Disseminated coccidioidomycosis, Primary cutaneous coccidioidomycosis. Primary pulmonary coccidioidomycosis) · Histoplasma capsulatum (Histoplasmosis, Primary cutaneous histoplasmosis, Primary pulmonary histoplasmosis, Progressive disseminated histoplasmosis) · Histoplasma duboisii (African histoplasmosis) · Lacazia loboi (Lobomycosis) · Paracoccidioides brasiliensis (Paracoccidioidomycosis)OtherBlastomyces dermatitidis (Blastomycosis, North American blastomycosis, South American blastomycosis) · Sporothrix schenckii (Sporotrichosis) · Penicillium marneffei (Penicilliosis)Yeast-likeCandida albicans (Candidiasis, Oral, Esophageal, Vulvovaginal, Chronic mucocutaneous, Antibiotic candidiasis, Candidal intertrigo, Candidal onychomycosis, Candidal paronychia, Candidid, Diaper candidiasis, Congenital cutaneous candidiasis, Perianal candidiasis, Systemic candidiasis, Erosio interdigitalis blastomycetica) · C. glabrata · C. tropicalis · C. lusitaniae · Pneumocystis jirovecii (Pneumocystosis, Pneumocystis pneumonia)Mold-likeAspergillus (Aspergillosis, Aspergilloma, Allergic bronchopulmonary aspergillosis, Primary cutaneous aspergillosis) · Exophiala jeanselmei (Eumycetoma) · Fonsecaea pedrosoi/Fonsecaea compacta/Phialophora verrucosa (Chromoblastomycosis) · Geotrichum candidum (Geotrichosis) · Pseudallescheria boydii (Allescheriasis)Mucorales
(Mucormycosis)Entomophthorales
(Entomophthoramycosis)Basidiobolus ranarum (Basidiobolomycosis) · Conidiobolus coronatus/Conidiobolus incongruus (Conidiobolomycosis)Enterocytozoon bieneusi/Encephalitozoon intestinalisMesomycetozoea Ungrouped Alternariosis · Fungal folliculitis · Fusarium (Fusariosis) · Granuloma gluteale infantum · Hyalohyphomycosis · Otomycosis · PhaeohyphomycosisCategories:- Mycosis-related cutaneous conditions

Wikimedia Foundation. 2010.