- Gene therapy
-
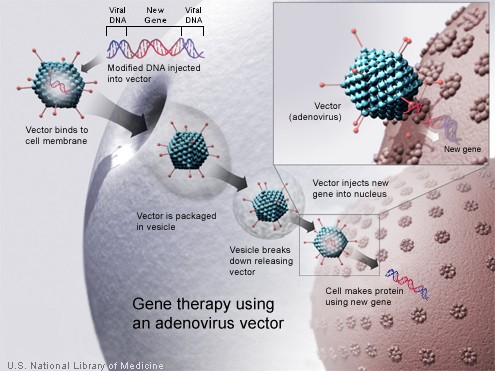
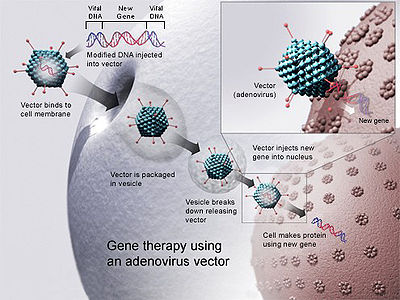 Gene therapy using an Adenovirus vector. A new gene is inserted into an adenovirull. If the treatment is successful, the new gene will make a functional protein.
Gene therapy using an Adenovirus vector. A new gene is inserted into an adenovirull. If the treatment is successful, the new gene will make a functional protein.
Gene therapy is the insertion, alteration, or removal of genes within an individual's cells and biological tissues to treat disease. It is a technique for correcting defective genes that are responsible for disease development.[1] The most common form of gene therapy involves the insertion of functional genes into an unspecified genomic location in order to replace a mutated gene, but other forms involve directly correcting the mutation or modifying normal gene that enables a viral infection. Although the technology is still in its infancy, it has been used with some success.[2]
Approach
Scientists have taken the logical step of trying to introduce genes directly into human cells, focusing on diseases caused by single-gene defects, such as cystic fibrosis, haemophilia, muscular dystrophy and sickle cell anemia. However, this has proven more difficult than modifying bacteria, primarily because of the problems involved in carrying large sections of DNA and delivering them to the correct site on the gene. Today, most gene therapy studies are aimed at cancer and hereditary diseases linked to a genetic defect. Antisense therapy is not strictly a form of gene therapy, but is a related, genetically-mediated therapy.
The most common form of genetic engineering involves the insertion of a functional gene at an unspecified location in the host genome.This is accomplished by isolating and copying the gene of interest, generating a construct containing all the genetic elements for correct expression, and then inserting this construct into a random location in the host organism. Other forms of genetic engineering include gene targeting and knocking out specific genes via engineered nucleases such as zinc finger nucleases, engineered I-CreI homing endonucleases, or nucleases generated from TAL effectors. An example of gene-knockout mediated gene therapy is the knockout of the human CCR5 gene in T-cells in order to control HIV infection.[3] This approach is currently being used in several human clinical trials.[4]
The biology of human gene therapy remains complex and many techniques need further development. Many diseases and their strict genetic link need to be understood more fully before gene therapy can be used appropriately. The public policy debate surrounding the possible use of genetically engineered material in human subjects has been equally complex. Major participants in the debate have come from the fields of biology, government, law, medicine, philosophy, politics, and religion, each bringing different views to the discussion.[citation needed]
Types of gene therapy
Gene therapy may be classified into the two following types:
Germ line gene therapy
In the case of germ line gene therapy, Germ cells, i.e., sperm or eggs, are modified by the introduction of functional genes, which are integrated into their genomes. Therefore, the change due to therapy would be heritable and would be passed on to later generations. This new approach, theoretically, should be highly effective in counteracting genetic disorders and hereditary diseases. However, many jurisdictions prohibit this for application in human beings, at least for the present, for a variety of technical and ethical reasons.[5]
Somatic gene therapy
In the case of somatic gene therapy, the therapeutic genes are transferred into the somatic cells of a patient. Any modifications and effects will be restricted to the individual patient only, and will not be inherited by the patient's offspring or later generations.
Vectors in gene therapy
Viruses
Main article: Viral vectorAll viruses bind to their hosts and introduce their genetic material into the host cell as part of their replication cycle. This genetic material contains basic 'instructions' of how to produce more copies of these viruses, hijacking the body's normal production machinery to serve the needs of the virus. The host cell will carry out these instructions and produce additional copies of the virus, leading to more and more cells becoming infected. Some types of viruses insert their genes into the host's genome, but do not actually enter the cell. Others penetrate the cell membrane disguised as protein molecules and enter the cell.
There are two main types of virus infection: lytic and lysogenic. Shortly after inserting its DNA, viruses of the lytic cycle quickly produce more viruses, burst from the cell and infect more cells. Lysogenic viruses integrate their DNA into the DNA of the host cell and may live in the body for many years before responding to a trigger. The virus reproduces as the cell does and does not inflict bodily harm until it is triggered. The trigger releases the DNA from that of the host and employs it to create new viruses.
Retroviruses
The genetic material in retroviruses is in the form of RNA molecules, while the genetic material of their hosts is in the form of DNA. When a retrovirus infects a host cell, it will introduce its RNA together with some enzymes, namely reverse transcriptase and integrase, into the cell. This RNA molecule from the retrovirus must produce a DNA copy from its RNA molecule before it can be integrated into the genetic material of the host cell. The process of producing a DNA copy from an RNA molecule is termed reverse transcription. It is carried out by one of the enzymes carried in the virus, called reverse transcriptase. After this DNA copy is produced and is free in the nucleus of the host cell, it must be incorporated into the genome of the host cell. That is, it must be inserted into the large DNA molecules in the cell (the chromosomes). This process is done by another enzyme carried in the virus called integrase.
Now that the genetic material of the virus has been inserted, it can be said that the host cell has been modified to contain new genes. If this host cell divides later, its descendants will all contain the new genes. Sometimes the genes of the retrovirus do not express their information immediately.
One of the problems of gene therapy using retroviruses is that the integrase enzyme can insert the genetic material of the virus into any arbitrary position in the genome of the host; it randomly inserts the genetic material into a chromosome. If genetic material happens to be inserted in the middle of one of the original genes of the host cell, this gene will be disrupted (insertional mutagenesis). If the gene happens to be one regulating cell division, uncontrolled cell division (i.e., cancer) can occur. This problem has recently begun to be addressed by utilizing zinc finger nucleases[6] or by including certain sequences such as the beta-globin locus control region to direct the site of integration to specific chromosomal sites.
Gene therapy trials using retroviral vectors to treat X-linked severe combined immunodeficiency (X-SCID) represent the most successful application of gene therapy to date. More than twenty patients have been treated in France and Britain, with a high rate of immune system reconstitution observed. Similar trials were restricted or halted in the USA when leukemia was reported in patients treated in the French X-SCID gene therapy trial.[citation needed] To date, four children in the French trial and one in the British trial have developed leukemia as a result of insertional mutagenesis by the retroviral vector. All but one of these children responded well to conventional anti-leukemia treatment. Gene therapy trials to treat SCID due to deficiency of the Adenosine Deaminase (ADA) enzyme (one form of SCID)[7] continue with relative success in the USA, Britain, Ireland, Italy and Japan.
Adenoviruses
Adenoviruses are viruses that carry their genetic material in the form of double-stranded DNA. They cause respiratory, intestinal, and eye infections in humans (especially the common cold). When these viruses infect a host cell, they introduce their DNA molecule into the host. The genetic material of the adenoviruses is not incorporated (transient) into the host cell's genetic material. The DNA molecule is left free in the nucleus of the host cell, and the instructions in this extra DNA molecule are transcribed just like any other gene. The only difference is that these extra genes are not replicated when the cell is about to undergo cell division so the descendants of that cell will not have the extra gene. As a result, treatment with the adenovirus will require readministration in a growing cell population although the absence of integration into the host cell's genome should prevent the type of cancer seen in the SCID trials. This vector system has been promoted for treating cancer and indeed the first gene therapy product to be licensed to treat cancer, Gendicine, is an adenovirus. Gendicine, an adenoviral p53-based gene therapy was approved by the Chinese food and drug regulators in 2003 for treatment of head and neck cancer. Advexin, a similar gene therapy approach from Introgen, was turned down by the US Food and Drug Administration (FDA) in 2008.
Concerns about the safety of adenovirus vectors were raised after the 1999 death of Jesse Gelsinger while participating in a gene therapy trial. Since then, work using adenovirus vectors has focused on genetically crippled versions of the virus.
Envelope protein pseudotyping of viral vectors
The viral vectors described above have natural host cell populations that they infect most efficiently. Retroviruses have limited natural host cell ranges, and although adenovirus and adeno-associated virus are able to infect a relatively broader range of cells efficiently, some cell types are refractory to infection by these viruses as well. Attachment to and entry into a susceptible cell is mediated by the protein envelope on the surface of a virus. Retroviruses and adeno-associated viruses have a single protein coating their membrane, while adenoviruses are coated with both an envelope protein and fibers that extend away from the surface of the virus. The envelope proteins on each of these viruses bind to cell-surface molecules such as heparin sulfate, which localizes them upon the surface of the potential host, as well as with the specific protein receptor that either induces entry-promoting structural changes in the viral protein, or localizes the virus in endosomes wherein acidification of the lumen induces this refolding of the viral coat. In either case, entry into potential host cells requires a favorable interaction between a protein on the surface of the virus and a protein on the surface of the cell. For the purposes of gene therapy, one might either want to limit or expand the range of cells susceptible to transduction by a gene therapy vector. To this end, many vectors have been developed in which the endogenous viral envelope proteins have been replaced by either envelope proteins from other viruses, or by chimeric proteins. Such chimera would consist of those parts of the viral protein necessary for incorporation into the virion as well as sequences meant to interact with specific host cell proteins. Viruses in which the envelope proteins have been replaced as described are referred to as pseudotyped viruses. For example, the most popular retroviral vector for use in gene therapy trials has been the lentivirus Simian immunodeficiency virus coated with the envelope proteins, G-protein, from Vesicular stomatitis virus. This vector is referred to as VSV G-pseudotyped lentivirus, and infects an almost universal set of cells. This tropism is characteristic of the VSV G-protein with which this vector is coated. Many attempts have been made to limit the tropism of viral vectors to one or a few host cell populations. This advance would allow for the systemic administration of a relatively small amount of vector. The potential for off-target cell modification would be limited, and many concerns from the medical community would be alleviated. Most attempts to limit tropism have used chimeric envelope proteins bearing antibody fragments. These vectors show great promise for the development of "magic bullet" gene therapies.
Replication-Competent Vectors
A replication-competent vector called ONYX-015 is used in replicating tumor cells. It was found that in the absence of the E1B-55Kd viral protein, adenovirus caused very rapid apoptosis of infected, p53(+) cells, and this results in dramatically reduced virus progeny and no subsequent spread. Apoptosis was mainly the result of the ability of EIA to inactivate p300. In p53(-) cells, deletion of E1B 55kd has no consequence in terms of apoptosis, and viral replication is similar to that of wild-type virus, resulting in massive killing of cells.
A replication-defective vector deletes some essential genes. These deleted genes are still necessary in the body so they are replaced with either a helper virus or a DNA molecule.
Cis and trans-acting elements
Replication-defective vectors always contain a “transfer construct”. The transfer construct carries the gene to be transduced or “transgene”. The transfer construct also carries the sequences which are necessary for the general functioning of the viral genome: packaging sequence, repeats for replication and, when needed, priming of reverse transcription. These are denominated cis-acting elements, because they need to be on the same piece of DNA as the viral genome and the gene of interest. Trans-acting elements are viral elements, which can be encoded on a different DNA molecule. For example, the viral structural proteins can be expressed from a different genetic element than the viral genome.
Herpes Simplex Virus
The Herpes simplex virus is a human neurotropic virus. This is mostly examined for gene transfer in the nervous system. The wild type HSV-1 virus is able to infect neurons. Infected neurons are not rejected by the immune system. Though the latent virus is not transcriptionally apparent, it does possess neuron specific promoters that can continue to function normally[further explanation needed]. Antibodies to HSV-1 are common in humans, however complications due to herpes infection are somewhat rare.[9]
Non-viral methods
Non-viral methods present certain advantages over viral methods, with simple large scale production and low host immunogenicity being just two. Previously, low levels of transfection and expression of the gene held non-viral methods at a disadvantage; however, recent advances in vector technology have yielded molecules and techniques with transfection efficiencies similar to those of viruses.[2]
Injection of Naked DNA
This is the simplest method of non-viral transfection. Clinical trials carried out of intramuscular injection of a naked DNA plasmid have occurred with some success; however, the expression has been very low in comparison to other methods of transfection. In addition to trials with plasmids, there have been trials with naked PCR product, which have had similar or greater success. Cellular uptake of naked DNA is generally inefficient. Research efforts focusing on improving the efficiency of naked DNA uptake have yielded several novel methods, such as electroporation, sonoporation, and the use of a "gene gun", which shoots DNA coated gold particles into the cell using high pressure gas.[10]
Physical Methods to Enhance Delivery
Electroporation
Electroporation is a method that uses short pulses of high voltage to carry DNA across the cell membrane. This shock is thought to cause temporary formation of pores in the cell membrane, allowing DNA molecules to pass through. Electroporation is generally efficient and works across a broad range of cell types. However, a high rate of cell death following electroporation has limited its use, including clinical applications.
More recently a newer method of electroporation, termed electron-avalanche transfection, has been used in gene therapy experiments. By using a high-voltage plasma discharge, DNA was efficiently delivered following very short (microsecond) pulses. Compared to electroporation, the technique resulted in greatly increased efficiency and less cellular damage.
Gene Gun
The use of particle bombardment, or the gene gun, is another physical method of DNA transfection. In this technique, DNA is coated with gold particles and loaded into a device which generates a force to achieve penetration of DNA/gold into the cells.
Sonoporation
Sonoporation uses ultrasonic frequencies to deliver DNA into cells. The process of acoustic cavitation is thought to disrupt the cell membrane and allow DNA to move into cells.
Magnetofection
In a method termed magnetofection, DNA is complexed to magnetic particles, and a magnet is placed underneath the tissue culture dish to bring DNA complexes into contact with a cell monolayer.
Chemical Methods to Enhance Delivery
Oligonucleotides
The use of synthetic oligonucleotides in gene therapy is to inactivate the genes involved in the disease process. There are several methods by which this is achieved. One strategy uses antisense specific to the target gene to disrupt the transcription of the faulty gene. Another uses small molecules of RNA called siRNA to signal the cell to cleave specific unique sequences in the mRNA transcript of the faulty gene, disrupting translation of the faulty mRNA, and therefore expression of the gene. A further strategy uses double stranded oligodeoxynucleotides as a decoy for the transcription factors that are required to activate the transcription of the target gene. The transcription factors bind to the decoys instead of the promoter of the faulty gene, which reduces the transcription of the target gene, lowering expression. Additionally, single stranded DNA oligonucleotides have been used to direct a single base change within a mutant gene. The oligonucleotide is designed to anneal with complementarity to the target gene with the exception of a central base, the target base, which serves as the template base for repair. This technique is referred to as oligonucleotide mediated gene repair, targeted gene repair, or targeted nucleotide alteration.
Lipoplexes and polyplexes
To improve the delivery of the new DNA into the cell, the DNA must be protected from damage and (positively charged). Initially, anionic and neutral lipids were used for the construction of lipoplexes for synthetic vectors. However, in spite of the facts that there is little toxicity associated with them, that they are compatible with body fluids and that there was a possibility of adapting them to be tissue specific; they are complicated and time consuming to produce so attention was turned to the cationic versions.
Cationic lipids, due to their positive charge, were first used to condense negatively charged DNA molecules so as to facilitate the encapsulation of DNA into liposomes. Later it was found that the use of cationic lipids significantly enhanced the stability of lipoplexes. Also as a result of their charge, cationic liposomes interact with the cell membrane, endocytosis was widely believed as the major route by which cells uptake lipoplexes. Endosomes are formed as the results of endocytosis, however, if genes can not be released into cytoplasm by breaking the membrane of endosome, they will be sent to lysosomes where all DNA will be destroyed before they could achieve their functions. It was also found that although cationic lipids themselves could condense and encapsulate DNA into liposomes, the transfection efficiency is very low due to the lack of ability in terms of “endosomal escaping”. However, when helper lipids (usually electroneutral lipids, such as DOPE) were added to form lipoplexes, much higher transfection efficiency was observed. Later on, it was figured out that certain lipids have the ability to destabilize endosomal membranes so as to facilitate the escape of DNA from endosome, therefore those lipids are called fusogenic lipids. Although cationic liposomes have been widely used as an alternative for gene delivery vectors, a dose dependent toxicity of cationic lipids were also observed which could limit their therapeutic usages.
The most common use of lipoplexes has been in gene transfer into cancer cells, where the supplied genes have activated tumor suppressor control genes in the cell and decrease the activity of oncogenes. Recent studies have shown lipoplexes to be useful in transfecting respiratory epithelial cells, so they may be used for treatment of genetic respiratory diseases such as cystic fibrosis.
Complexes of polymers with DNA are called polyplexes. Most polyplexes consist of cationic polymers and their production is regulated by ionic interactions. One large difference between the methods of action of polyplexes and lipoplexes is that polyplexes cannot release their DNA load into the cytoplasm, so to this end, co-transfection with endosome-lytic agents (to lyse the endosome that is made during endocytosis, the process by which the polyplex enters the cell) such as inactivated adenovirus must occur. However, this isn't always the case, polymers such as polyethylenimine have their own method of endosome disruption as does chitosan and trimethylchitosan.
Dendrimers
A dendrimer is a highly branched macromolecule with a spherical shape. The surface of the particle may be functionalized in many ways and many of the properties of the resulting construct are determined by its surface.
In particular it is possible to construct a cationic dendrimer, i.e. one with a positive surface charge. When in the presence of genetic material such as DNA or RNA, charge complimentarity leads to a temporary association of the nucleic acid with the cationic dendrimer. On reaching its destination the dendrimer-nucleic acid complex is then taken into the cell via endocytosis.
In recent years the benchmark for transfection agents has been cationic lipids. Limitations of these competing reagents have been reported to include: the lack of ability to transfect a number of cell types, the lack of robust active targeting capabilities, incompatibility with animal models, and toxicity. Dendrimers offer robust covalent construction and extreme control over molecule structure, and therefore size. Together these give compelling advantages compared to existing approaches.
Producing dendrimers has historically been a slow and expensive process consisting of numerous slow reactions, an obstacle that severely curtailed their commercial development. The Michigan based company Dendritic Nanotechnologies discovered a method to produce dendrimers using kinetically driven chemistry, a process that not only reduced cost by a magnitude of three, but also cut reaction time from over a month to several days. These new "Priostar" dendrimers can be specifically constructed to carry a DNA or RNA payload that transfects cells at a high efficiency with little or no toxicity.[citation needed]
Inorganic Nanoparticles
Inorganic nanoparticles, such as gold, silica, iron oxide (ex. magnetofection) and calcium phosphates have been shown to be capable of gene delivery.[11] Some of the benefits of inorganic vectors is in their storage stability, low manufacturing cost and often time, low immunogenicity, and resistance to microbial attack. Nanosized materials less than 100nm have been shown to efficiently trap the DNA or RNA and allows its escape from the endosome without degradation. Inorganics have also been shown to exhibit improved in vitro transfection for attached cell lines due to their increased density and preferential location on the base of the culture dish. Quantum dots have also been used successfully and permits the coupling of gene therapy with a stable fluorescence marker.
Hybrid methods
Due to every method of gene transfer having shortcomings, there have been some hybrid methods developed that combine two or more techniques. Virosomes are one example; they combine liposomes with an inactivated HIV or influenza virus. This has been shown to have more efficient gene transfer in respiratory epithelial cells than either viral or liposomal methods alone. Other methods involve mixing other viral vectors with cationic lipids or hybridising viruses.
Major developments in gene therapy
1970s and earlier
In 1972 Friedmann and Roblin authored a paper in Science titled "Gene therapy for human genetic disease?"[12] They cite Rogers S for proposing "that exogenous 'good'" DNA be used to replace the defective DNA in those who suffer from genetic defects.[13] They also cite the first attempt to perform gene therapy as [New York Times, 20 September 1970].
1990s
The first approved gene therapy case in the United States took place on September 14, 1990, at the National Institute of Health. It was performed on a four year old girl named Ashanti DeSilva. It was a treatment for a genetic defect that left her with an immune system deficiency. The effects were only temporary, but successful (Boylan 313).
New gene therapy approach repairs errors in messenger RNA derived from defective genes. This technique has the potential to treat the blood disorder thalassaemia, cystic fibrosis, and some cancers.[14] Researchers at Case Western Reserve University and Copernicus Therapeutics are able to create tiny liposomes 25 nanometers across that can carry therapeutic DNA through pores in the nuclear membrane.[15]
Sickle cell disease is successfully treated in mice.[16]
in 1992 Doctor Claudio Bordignon working at the Vita-Salute San Raffaele University, Milan, Italy performed the first procedure of gene therapy using hematopoietic stem cells as vectors to deliver genes intended to correct hereditary diseases.[17] In 2002 this work led to the publication of the first successful gene therapy treatment for adenosine deaminase-deficiency (SCID). The success of a multi-center trial for treating children with SCID (severe combined immune deficiency or "bubble boy" disease) held from 2000 and 2002 was questioned when two of the ten children treated at the trial's Paris center developed a leukemia-like condition. Clinical trials were halted temporarily in 2002, but resumed after regulatory review of the protocol in the United States, the United Kingdom, France, Italy, and Germany.[18]
In 1993 Andrew Gobea was born with severe combined immunodeficiency (SCID). Genetic screening before birth showed that he had SCID. Blood was removed from Andrew's placenta and umbilical cord immediately after birth, containing stem cells. The allele that codes for ADA was obtained and was inserted into a retrovirus. Retroviruses and stem cells were mixed, after which they entered and inserted the gene into the stem cells' chromosomes. Stem cells containing the working ADA gene were injected into Andrew's blood system via a vein. Injections of the ADA enzyme were also given weekly. For four years T-cells (white blood cells), produced by stem cells, made ADA enzymes using the ADA gene. After four years more treatment was needed.
The 1999 death of Jesse Gelsinger in a gene-therapy experiment resulted in a significant setback to gene therapy research in the United States.[19][20] As a result, the U.S. FDA suspended several clinical trials pending the re-evaluation of ethical and procedural practices in the field.[21]
2000s
2003
In 2003 a University of California, Los Angeles research team inserted genes into the brain using liposomes coated in a polymer called polyethylene glycol. The transfer of genes into the brain is a significant achievement because viral vectors are too big to get across the blood-brain barrier. This method has potential for treating Parkinson's disease.[22]
RNA interference or gene silencing may be a new way to treat Huntington's disease. Short pieces of double-stranded RNA (short, interfering RNAs or siRNAs) are used by cells to degrade RNA of a particular sequence. If a siRNA is designed to match the RNA copied from a faulty gene, then the abnormal protein product of that gene will not be produced.[23]
2006
Scientists at the National Institutes of Health (Bethesda, Maryland) have successfully treated metastatic melanoma in two patients using killer T cells genetically retargeted to attack the cancer cells. This study constitutes one of the first demonstrations that gene therapy can be effective in treating cancer.[24]
In March 2006 an international group of scientists announced the successful use of gene therapy to treat two adult patients for a disease affecting myeloid cells. The study, published in Nature Medicine, is believed to be the first to show that gene therapy can cure diseases of the myeloid system.[25]
In May 2006 a team of scientists led by Dr. Luigi Naldini and Dr. Brian Brown from the San Raffaele Telethon Institute for Gene Therapy (HSR-TIGET) in Milan, Italy reported a breakthrough for gene therapy in which they developed a way to prevent the immune system from rejecting a newly delivered gene.[26] Similar to organ transplantation, gene therapy has been plagued by the problem of immune rejection. So far, delivery of the 'normal' gene has been difficult because the immune system recognizes the new gene as foreign and rejects the cells carrying it. To overcome this problem, the HSR-TIGET group utilized a newly uncovered network of genes regulated by molecules known as microRNAs. Dr. Naldini's group reasoned that they could use this natural function of microRNA to selectively turn off the identity of their therapeutic gene in cells of the immune system and prevent the gene from being found and destroyed. The researchers injected mice with the gene containing an immune-cell microRNA target sequence, and the mice did not reject the gene, as previously occurred when vectors without the microRNA target sequence were used. This work will have important implications for the treatment of hemophilia and other genetic diseases by gene therapy.
In November 2006 Preston Nix from the University of Pennsylvania School of Medicine reported on VRX496, a gene-based immunotherapy for the treatment of human immunodeficiency virus (HIV) that uses a lentiviral vector for delivery of an antisense gene against the HIV envelope. In the Phase I trial enrolling five subjects with chronic HIV infection who had failed to respond to at least two antiretroviral regimens, a single intravenous infusion of autologous CD4 T cells genetically modified with VRX496 was safe and well tolerated. All patients had stable or decreased viral load; four of the five patients had stable or increased CD4 T cell counts. In addition, all five patients had stable or increased immune response to HIV antigens and other pathogens. This was the first evaluation of a lentiviral vector administered in U.S. Food and Drug Administration-approved human clinical trials for any disease.[27] Data from an ongoing Phase I/II clinical trial were presented at CROI 2009.[28]
2007
On 1 May 2007 Moorfields Eye Hospital and University College London's Institute of Ophthalmology announced the world's first gene therapy trial for inherited retinal disease. The first operation was carried out on a 23 year-old British male, Robert Johnson, in early 2007.[29] Leber's congenital amaurosis is an inherited blinding disease caused by mutations in the RPE65 gene. The results of the Moorfields/UCL trial were published in New England Journal of Medicine in April 2008. They researched the safety of the subretinal delivery of recombinant adeno associated virus (AAV) carrying RPE65 gene, and found it yielded positive results, with patients having modest increase in vision, and, perhaps more importantly, no apparent side-effects.[30]
2009
In September 2009, the journal Nature reported that researchers at the University of Washington and University of Florida were able to give trichromatic vision to squirrel monkeys using gene therapy, a hopeful precursor to a treatment for color blindness in humans.[31] In November 2009, the journal Science reported that researchers succeeded at halting a fatal brain disease, adrenoleukodystrophy, using a vector derived from HIV to deliver the gene for the missing enzyme.[32]
2010
A paper by Komáromy et al. published in April 2010, deals with gene therapy for a form of achromatopsia in dogs. Achromatopsia, or complete color blindness, is presented as an ideal model to develop gene therapy directed to cone photoreceptors. Cone function and day vision have been restored for at least 33 months in two young dogs with achromatopsia. However, the therapy was less efficient for older dogs.[33]
2011
In 2007 and 2008, a man being treated by Gero Hütter was cured of HIV by repeated Hematopoietic stem cell transplantation (see also Allogeneic stem cell transplantation, Allogeneic bone marrow transplantation, Allotransplantation) with double-delta-32 mutation which disables the CCR5 receptor; this cure was not completely accepted by the medical community until 2011.[34] This cure required complete ablation of existing bone marrow which is very debilitating.
Problems and ethics
For the safety of gene therapy, the Weismann barrier is fundamental in the current thinking. Soma-to-germline feedback should therefore be impossible. However, there are indications[35] that the Weismann barrier can be breached. One way it might possibly be breached is if the treatment were somehow misapplied and spread to the testes and therefore would infect the germline against the intentions of the therapy.
Some of the problems of gene therapy include:
- Short-lived nature of gene therapy – Before gene therapy can become a permanent cure for any condition, the therapeutic DNA introduced into target cells must remain functional and the cells containing the therapeutic DNA must be long-lived and stable. Problems with integrating therapeutic DNA into the genome and the rapidly dividing nature of many cells prevent gene therapy from achieving any long-term benefits. Patients will have to undergo multiple rounds of gene therapy.
- Immune response – Anytime a foreign object is introduced into human tissues, the immune system has evolved to attack the invader. The risk of stimulating the immune system in a way that reduces gene therapy effectiveness is always a possibility. Furthermore, the immune system's enhanced response to invaders that it has seen before makes it difficult for gene therapy to be repeated in patients.
- Problems with viral vectors – Viruses, the carrier of choice in most gene therapy studies, present a variety of potential problems to the patient —toxicity, immune and inflammatory responses, and gene control and targeting issues. In addition, there is always the fear that the viral vector, once inside the patient, may recover its ability to cause disease.
- Multigene disorders – Conditions or disorders that arise from mutations in a single gene are the best candidates for gene therapy. Unfortunately, some of the most commonly occurring disorders, such as heart disease, high blood pressure, Alzheimer's disease, arthritis, and diabetes, are caused by the combined effects of variations in many genes. Multigene or multifactorial disorders such as these would be especially difficult to treat effectively using gene therapy.
- Chance of inducing a tumor (insertional mutagenesis) - If the DNA is integrated in the wrong place in the genome, for example in a tumor suppressor gene, it could induce a tumor. This has occurred in clinical trials for X-linked severe combined immunodeficiency (X-SCID) patients, in which hematopoietic stem cells were transduced with a corrective transgene using a retrovirus, and this led to the development of T cell leukemia in 3 of 20 patients.[36]
Deaths have occurred due to gene therapy, including that of Jesse Gelsinger.[37]
Preventive gene therapy
Preventive gene therapy is the repair of a gene with a mutation associated with a progressive disease, prior to the expression of a medical condition, in order to prevent that expression. There are a number of considerations:[38]
- It is hard to get U.S. FDA approval to treat a pre-symptomatic condition because it is hard to predict the complications that may arise, so it is hard to give a risk/benefit analysis. This is an obstacle to long-term therapies.
- It is easier to gain approval for short-term therapies to treat expressed conditions rather than prevent them.
- It is not known whether the repair of a mutation will help to treat a condition which has already progressed beyond the initial consequences of that mutation.
In popular culture
- In the TV series Dark Angel gene therapy is mentioned as one of the practices performed on transgenics and their surrogate mothers at Manticore, and in the episode Prodigy, Dr. Tanaka uses a groundbreaking new form of gene therapy to turn Jude, a premature, vegetative baby of a crack/cocaine addict, into a boy genius.
- Gene therapy is a crucial plot element in the video game Metal Gear Solid, where it has been used to enhance the battle capabilities of enemy soldiers.
- Gene therapy plays a major role in the sci-fi series Stargate Atlantis, as a certain type of alien technology can only be used if one has a certain gene which can be given to the members of the team through gene therapy.
- Gene therapy also plays a major role in the plot of the James Bond movie Die Another Day.
- Gene therapy plays a recurring role in the present-time sci-fi television program ReGenesis, where it is used to cure various diseases, enhance athletic performance and produce vast profits for bio-tech corporations. (e.g. an undetectable performance-enhancing gene therapy was used by one of the characters on himself, but to avoid copyright infringement, this gene therapy was modified from the tested-to-be-harmless original, which produced a fatal cardiovascular defect)
- Gene therapy is the basis for the plot line of the film I Am Legend.[39]
- Gene therapy is an important plot key in the game Bioshock where the game contents refer to plasmids and [gene] splicers.
- The book Next by Michael Crichton unravels a story in which fictitious biotechnology companies experiment with gene therapy.
- In the television show Alias, a breakthrough in molecular gene therapy is discovered, whereby a patient's body is reshaped to identically resemble someone else. Protagonist Sydney Bristow's best friend was secretly killed and her "double" resumed her place.
Gun of God David R. Cudlip (Author)
See also
- Antisense therapy
- DNA
- Full Genome Sequencing
- Gene therapy for color blindness
- Genetic engineering
- Life extension
- List of life extension related topics
- Pharmacological gene therapy
- Predictive Medicine
- Technology assessment
- Therapeutic gene modulation
References
- ^ Notes on Gene Therapy | PharmaXChange.info
- ^ a b Kamimura K, Suda T, Zhang G, et al. (2011). "Advances in Gene Delivery Systems". Pharm Med 25 (5): 293–306. doi:10.2165/11594020-000000000-00000. http://adisonline.com/pharmaceuticalmedicine/Abstract/2011/25050/Advances_in_Gene_Delivery_Systems.2.aspx.
- ^ Perez EE, Wang J, Miller JC, et al. (July 2008). "Establishment of HIV-1 resistance in CD4+ T cells by genome editing using zinc-finger nucleases". Nat. Biotechnol. 26 (7): 808–16. doi:10.1038/nbt1410. PMID 18587387.
- ^ Urnov FD, Rebar EJ, Holmes MC, Zhang HS, Gregory PD (September 2010). "Genome editing with engineered zinc finger nucleases". Nat. Rev. Genet. 11 (9): 636–46. doi:10.1038/nrg2842. PMID 20717154.
- ^ Strachnan, T. and A. P. Read, Human Molecular Genetics, 3rd Edition, Garland Publishing, 2004, p. 616.
- ^ Durai S, Mani M, Kandavelou K, Wu J, Porteus MH, Chandrasegaran S (2005). "Zinc finger nucleases: custom-designed molecular scissors for genome engineering of plant and mammalian cells". Nucleic Acids Res. 33 (18): 5978–90. doi:10.1093/nar/gki912. PMC 1270952. PMID 16251401. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1270952.
- ^ http://www.scid.net/about.htm
- ^ a b "The Process of Gene Therapy." Alternate Heals. 8 may 2006. Alternate Medicine, Web. 23 November 2009.
- ^ Harwood, Adrian J. Protocols for Gene Analysis. 1st. 31. Totowa, New Jersey: Humana Press, 1994. Print.
- ^ Scribd.com
- ^ Wagner,DE and Bhaduri, SB. (2011)Progress and Outlook of Inorganic Nanoparticles for Delivery of Nucleic Acid Sequences Related to Orthopedic Pathologies: A Review., Tissue Engineering Part B: Reviews.
- ^ Friedmann, T.; Roblin, R. (1972). "Gene Therapy for Human Genetic Disease?". Science 175 (4025): 949. Bibcode 1972Sci...175..949F. doi:10.1126/science.175.4025.949. PMID 5061866.
- ^ Rogers S, New Sci. 1970, p. 194)
- ^ "Subtle gene therapy tackles blood disorder - 11 October 2002". New Scientist. http://www.newscientist.com/article/dn2915-subtle-gene-therapy-tackles-blood-disorder.html. Retrieved 2010-08-17.
- ^ "DNA nanoballs boost gene therapy - 12 May 2002". New Scientist. http://www.newscientist.com/article/dn2257-dna-nanoballs-boost-gene-therapy.html. Retrieved 2010-08-17.
- ^ Fisher, Jennifer. "Murine Gene Therapy Corrects Symptoms of Sickle Cell Disease - The Scientist - Magazine of the Life Sciences". The Scientist. http://www.the-scientist.com/article/display/12938/. Retrieved 2010-08-17.
- ^ Abbott, A. (1992). "Gene therapy. Italians first to use stem cells". Nature 356 (6369): 465–199. Bibcode 1992Natur.356..465A. doi:10.1038/356465a0. PMID 1560817.
- ^ Cavazzana-Calvo M, Thrasher A, Mavilio F (Feb 2004). "The future of gene therapy". Nature 427 (6977): 779–81. doi:10.1038/427779a. PMID 14985734.
- ^ "First patient treated in stem cell study". Washington Post. 10-11-2010. http://www.washingtonpost.com/wp-dyn/content/article/2010/10/11/AR2010101102946.html. Retrieved 10-11-2010.
- ^ "Death Prompts FDA to Suspend Arthritis Gene Therapy Trial". Medpage Today. 7-27-2007. http://www.medpagetoday.com/Genetics/GeneralGenetics/6275. Retrieved 10-11-2010.
- ^ "Gene Therapy Ordered Halted At University". New York Times. 1-22-2000. http://select.nytimes.com/gst/abstract.html?res=F60E1EF73B590C718EDDA80894D8404482. Retrieved 10-11-2010.
- ^ "Undercover genes slip into the brain". New Scientist. 20 March 2003. http://www.newscientist.com/article/dn3520-undercover-genes-slip-into-the-brain.html. Retrieved 2010-08-17.
- ^ "Gene therapy may switch off Huntington's". New Scientist. 13 March 2003. http://www.newscientist.com/article/dn3493-gene-therapy-may-switch-off-huntingtons.html. Retrieved 2010-08-17.
- ^ Morgan RA, Dudley ME, Wunderlich JR, et al. (Oct 2006). "Cancer Regression in Patients After Transfer of Genetically Engineered Lymphocytes". Science 314 (5796): 126–9. doi:10.1126/science.1129003. PMC 2267026. PMID 16946036. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2267026.
- ^ Ott MG, Schmidt M, Schwarzwaelder K, et al. (Apr 2006). "Correction of X-linked chronic granulomatous disease by gene therapy, augmented by insertional activation of MDS1-EVI1, PRDM16 or SETBP1". Nat Med. 12 (4): 401–9. doi:10.1038/nm1393. PMID 16582916.
- ^ Brown BD, Venneri MA, Zingale A, Sergi Sergi L, Naldini L (May 2006). "Endogenous microRNA regulation suppresses transgene expression in hematopoietic lineages and enables stable gene transfer". Nat Med. 12 (5): 585–91. doi:10.1038/nm1398. PMID 16633348.
- ^ Levine BL, Humeau LM, Boyer J, et al. (Nov 2006). "Gene transfer in humans using a conditionally replicating lentiviral vector". Proc Natl Acad Sci U S A. 103 (46): 17372–7. doi:10.1073/pnas.0608138103. PMC 1635018. PMID 17090675. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1635018.
- ^ "Penn Medicine presents HIV gene therapy trial data at CROI 2009". EurekAlert!. http://www.eurekalert.org/pub_releases/2009-02/uops-pmp021009.php. Retrieved 2009-11-19.
- ^ "Gene therapy first for poor sight". BBC News. May 1, 2007. http://news.bbc.co.uk/1/hi/health/6609205.stm. Retrieved May 3, 2010.
- ^ Maguire AM, Simonelli F, Pierce EA, et al. (May 2008). "Safety and Efficacy of Gene Transfer for Leber's Congenital Amaurosis". N Engl J Med. 358 (21): 2240–8. doi:10.1056/NEJMoa0802315. PMC 2829748. PMID 18441370. http://content.nejm.org/cgi/content/full/NEJMoa0802315.
- ^ Nature.com
- ^ Kaiser, Jocelyn (2009-11-05). "Gene Therapy Halts Brain Disease in Two Boys - ScienceNOW". Sciencenow.sciencemag.org. http://sciencenow.sciencemag.org/cgi/content/full/2009/1105/1. Retrieved 2010-08-17.
- ^ Komáromy, A.; Alexander, J.; Rowlan, J.; Garcia, M.; Chiodo, V.; Kaya, A.; Tanaka, J.; Acland, G. et al. (2010). "Gene therapy rescues cone function in congenital achromatopsia". Human molecular genetics 19 (13): 2581–2593. doi:10.1093/hmg/ddq136. PMC 2883338. PMID 20378608. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2883338.
- ^ "The Man Who Had HIV and Now Does Not", by Tina Rosenberg, New York Magazine, May 29, 2011
- ^ Korthof G. "The implications of Steele's soma-to-germline feedback for human gene therapy". http://home.planet.nl/~gkorthof/kortho39a.htm.
- ^ Woods NB, Bottero V, Schmidt M, von Kalle C, Verma IM (Apr 2006). "Gene therapy: therapeutic gene causing lymphoma". Nature 440 (7088): 1123. doi:10.1038/4401123a. PMID 16641981.
Thrasher AJ, Gaspar HB, Baum C, et al. (Sep 2006). "Gene therapy: X-SCID transgene leukaemogenicity". Nature 443 (7109): E5–6; discussion E6–7. doi:10.1038/nature05219. PMID 16988659. - ^ ORNL.gov
- ^ "Gene Therapy Woes", by Mae-Wan Ho, March 29, 2005, Institute of Science in Society
- ^ "A Real-life 'I Am Legend?' Researcher Champions Development Of 'Reovirus' As Potential Treatment For Cancer". Sciencedaily.com. 2008-05-09. http://www.sciencedaily.com/releases/2008/05/080508185334.htm. Retrieved 2010-08-17.
- Tinkov, S., Bekeredjian, R., Winter, G., Coester, C., Polyplex-conjugated microbubbles for enhanced ultrasound targeted gene therapy,2008 AAPS Annual Meeting and Exposition, 16–20 November, Georgia World Congress Center, Atlanta, GA, USA, <http://www.aapsj.org/abstracts/AM_2008/AAPS2008-000838.PDF>
- Gardlík R, Pálffy R, Hodosy J, Lukács J, Turna J, Celec P (Apr 2005). "Vectors and delivery systems in gene therapy". Med Sci Monit. 11 (4): RA110–21. PMID 15795707. http://www.medscimonit.com/fulltxt.php?ICID=15907.
- Staff (November 18, 2005). "Gene Therapy" (FAQ). Human Genome Project Information. Oak Ridge National Laboratory. http://www.ornl.gov/sci/techresources/Human_Genome/medicine/genetherapy.shtml. Retrieved 2006-05-28.
- Salmons B, Günzburg WH (Apr 1993). "Targeting of retroviral vectors for gene therapy". Hum Gene Ther. 4 (2): 129–41. doi:10.1089/hum.1993.4.2-129. PMID 8494923.
- Baum C, Düllmann J, Li Z, et al. (Mar 2003). "Side effects of retroviral gene transfer into hematopoietic stem cells". Blood 101 (6): 2099–114. doi:10.1182/blood-2002-07-2314. PMID 12511419.
- Horn PA, Morris JC, Neff T, Kiem HP (Sep 2004). "Stem cell gene transfer—efficacy and safety in large animal studies". Mol. Ther. 10 (3): 417–31. doi:10.1016/j.ymthe.2004.05.017. PMID 15336643.
- Wang, Hongjie; Dmitry M. Shayakhmetov, Tobias Leege, Michael Harkey, Qiliang Li, Thalia Papayannopoulou, George Stamatoyannopolous, and André Lieber (September 2005). "A Capsid-Modified Helper-Dependent Adenovirus Vector Containing the β-Globin Locus Control Region Displays a Nonrandom Integration Pattern and Allows Stable, Erythroid-Specific Gene Expression". Journal of Virology 79 (17): 10999–1013. doi:10.1128/JVI.79.17.10999-11013.2005. PMC 1193620. PMID 16103151. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1193620.
- Gene therapy. Italians first to use stem cells. Abbott A. Nature. 9 April 1992;356(6369):465
External links
- Gene Therapy: Molecular Bandage? University of Utah's Genetic Science Learning Center
- The American Society of Gene & Cell Therapy
- The European Society of Gene Therapy
- 2003 news relating to gene therapy
- Research Group at Cambridge, UK working on overcoming current hurdles to successful gene therapy
- Council for Responsible Genetics
- Molecular Medicine and Gene Therapy at Lund University
- Dossier on gene therapy and clinical trials
- Cancer-genetherapy.com Site focusing on cancer gene therapy
- Gene Therapy Review.
- Gene Therapy News Network Excellent resource for latest news on Gene Therapy and Genetic Medicine.
Genetic engineering Genetically
modified
organismsMammalsMaizePotatoAmfloraRiceSoybeanRoundup Ready soybean · Vistive GoldTomatoFish tomato · Flavr SavrCottonBt cotton · Roundup Ready cottonOtherFishGlofish · SalmonBacteria and virusesProcesses TypesUses In agricultureIn humans and diagnosticsGene therapy · Genetic enhancementIn researchRelated articles Transgene · Detection of genetically modified organisms · Genetic pollution · Genetic engineering in fiction · Reverse transfectionSimilar fields Categories:
Wikimedia Foundation. 2010.