- One and a half syndrome
-
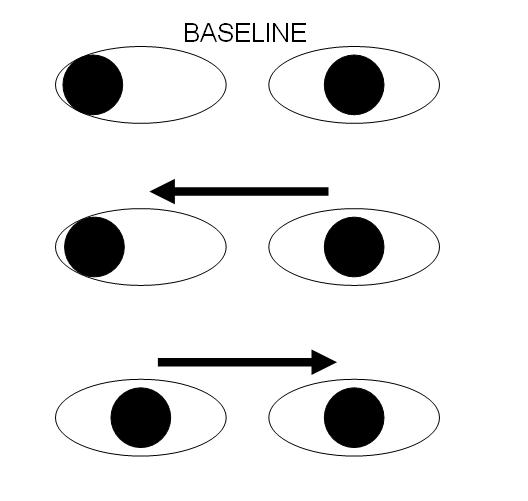
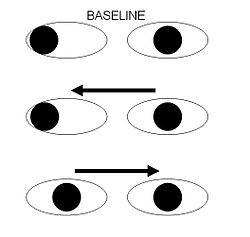 Schematic representation of most common extra-ocular movement abnormality in one and a half syndrome.
Schematic representation of most common extra-ocular movement abnormality in one and a half syndrome.
The one and a half syndrome is a rare ophthalmoparetic syndrome characterized by "a conjugate horizontal gaze palsy in one direction and an internuclear ophthalmoplegia in the other".[1] The most common manifestation of this unusual syndrome is limitation of horizontal eye movement to adduction (moving away from the midline) of one eye (e.g. right eye in the diagram on the right) with no horizontal movement of the other eye (e.g. left eye in the diagram on the right).[2] Nystagmus is also present when the eye on the opposite side of the lesion is abducted. Convergence is classically spared as Cranial Nerve III (oculomotor nerve) and its nucleus is spared bilaterally.
Contents
Anatomy
The syndrome usually results from single unilateral lesion of the paramedian pontine reticular formation and the ipsilateral medial longitudinal fasciculus. An alternative anatomical cause is a lesion of the abducens nucleus (VI) on one side, with interruption of the ipsilateral medial longitudinal fasciculus after it has crossed the midline from its site of origin in the contralateral oculomotorius (III) nucleus (resulting in a failure of adduction of the ipsilateral eye).
Causes
Causes of the one and a half syndrome include pontine hemorrhage, ischemia, tumors, infective mass lesions such as tuberculomas, and demyelinating conditions like multiple sclerosis.
Treatment
There have been cases of improvement in extra-ocular movement with botulinum toxin injection.[3]
See also
References
- ^ Wall M, Wray S (1983). "The one-and-a-half syndrome--a unilateral disorder of the pontine tegmentum: a study of 20 cases and review of the literature.". Neurology 33 (8): 971–80. PMID 6683820.
- ^ Siegel A, Sapru HN (2006). Essential Neuroscience (1st ed.). Baltimore, Maryland: Lippincott, Williams, & Wilkins. pp. 190–191. ISBN 9780781791212
- ^ Kipioti A, Taylor R (2003). "Botulinum toxin treatment of "one and a half syndrome"". Br J Ophthalmol 87 (7): 918–9. doi:10.1136/bjo.87.7.918-a. PMC 1771745. PMID 12812899. http://bjo.bmjjournals.com/cgi/reprint/87/7/918-a.
External links
- 1060438082 at GPnotebook - This link incorrectly states that the contralateral eye can still adduct. It can only abduct with nystagmus.
- Video at University of Utah
Lesions of spinal cord and brain Spinal cord/
vascular myelopathysensory: Sensory ataxia · Tabes dorsalis
motor: Motor neurone disease
mixed: Brown-Séquard syndrome · cord syndrome (Posterior, Anterior, Central/Syringomyelia) · Subacute combined degeneration of spinal cord (B12) · Cauda equina syndrome
Anterior spinal artery syndromeBrainstem Medulla (CN 8, 9, 10, 12)Pons (CN 5, 6, 7, 8)Lateral pontine syndrome (AICA) (lateral) · Medial pontine syndrome/Millard-Gubler syndrome (basilar)/Foville's syndrome (dorsal, basilar) · Locked-in syndrome (ventral) · Internuclear ophthalmoplegia · One and a half syndromeMidbrain (CN 3, 4)Weber's syndrome (ventral peduncle, PCA) · Benedikt syndrome (ventral tegmentum, PCA) · Parinaud's syndrome (dorsal, tumor) · Nothnagel's syndrome · Claude's syndromeOtherCerebellum Basal ganglia Cortex ACA syndrome · MCA syndrome · PCA syndrome
frontal lobe: Expressive aphasia · Abulia
parietal lobe: Receptive aphasia · Hemispatial neglect · Gerstmann syndrome · Astereognosis
occipital lobe: Balint's syndrome · Cortical blindness · Pure alexia
temporal lobe: Cortical deafness · ProsopagnosiaOther Categories:- Disorders of ocular muscles, binocular movement, accommodation and refraction
Wikimedia Foundation. 2010.