- Papilledema
-
Papilloedema Classification and external resources File:Papilloedema.jpg
Fundal photograph showing severe papilloedema in the right eyeICD-10 H47.1 ICD-9 377.0 DiseasesDB 9580 eMedicine oph/187 MeSH D010211 Papilledema (or papilloedema) is optic disc swelling that is caused by increased intracranial pressure. The swelling is usually bilateral and can occur over a period of hours to weeks. Unilateral presentation is extremely rare.
In intracranial hypertension, papilledema most commonly occurs bilaterally. When papilledema is found on fundoscopy, further evaluation is warranted as vision loss can result if the underlying condition is not treated. Further evaluation with a CT or MRI of the brain and/or spine is usually performed. Unilateral papilledema can suggest orbital pathology, such as an optic nerve glioma.
Contents
Signs and symptoms
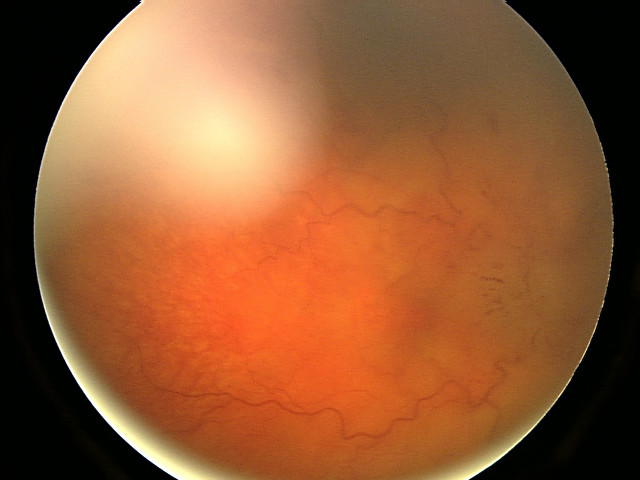
 Fundal photograph showing less severe papilledema
Fundal photograph showing less severe papilledema
Papilledema may be asymptomatic or present with headache in the early stages. However it may progress to enlargement of the blind spot, blurring of vision, visual obscurations (inability to see in a particular part of the visual field for a period of time) and ultimately total loss of vision may occur.
The signs of papilledema that are seen using an ophthalmoscope include
- venous engorgement (usually the first signs)
- loss of venous pulsation
- hemorrhages over and / or adjacent to the optic disc
- blurring of optic margins
- elevation of optic disc
- Paton's lines = radial retinal lines cascading from the optic disc
- If papilloedema persists for months, the disc hyperaemia subsides giving way to a grey or pale discthat loses its central cup. with time, the disc may develop small glistening crystalline deposits (disc pseudodrusen)
On visual field examination, the physician may elicit an enlarged blind spot; the visual acuity may remain relatively intact until papilledema is severe or prolonged.
Diagnosis
Checking the eyes for signs of papilledema should be carried out whenever there is a clinical suspicion of raised intracranial pressure, and is recommended in newly onset headaches. This may be done by ophthalmoscopy or slit lamp examination.
Causes
- Raised intracranial pressure: brain tumor, pseudotumor cerebri or cerebral venous sinus thrombosis, Intracerebral hemorrhage
- Respiratory failure[1]
- Hypotonia
- Accutane (Isotretinoin), which is a powerful derivative of Vitamin A, rarely causes Papilledema.
- Hypervitaminosis A, in some people who take megadoses of nutritional supplements and vitamins.
- Hyperammonemia, elevated level of ammonia in blood (including cerebral edema/intracranial pressure)
- Guillain-Barré syndrome due to elevated protein levels
- Foster Kennedy syndrome (FKS)
- Chiari Malformation
- Tumors of the frontal lobe
- Acute Mountain Sickness and High Altitude Cerebral Oedema
- Lyme disease (Lyme meningitis specifically, when the bacterial infection is in the central nervous system, causing increased intracranial pressure).
- Malignant Hypertension
- Medulloblastoma
- Orbital A.Ocular venous drainage block:central retinal venous block, cavernous sinus trombosis B.Local lesion:optic neuritis, ischemia of the nerve head, toxin (methanol), infiltration of the disc by glioma,sarcoidosis and lymphoma
Pathophysiology
As the optic nerve sheath is continuous with the subarachnoid space of the brain (and is regarded as an extension of the central nervous system), increased pressure is transmitted through to the optic nerve. The brain itself is relatively spared from pathological consequences of high pressure. However, the anterior end of the optic nerve stops abruptly at the eye. Hence the pressure is asymmetrical and this causes a pinching and protrusion of the optic nerve at its head. The fibers of the retinal ganglion cells of the optic disc become engorged and bulge anteriorly. Persistent and extensive optic nerve head swelling, or optic disc edema, can lead to loss of these fibers and permanent visual impairment.
Treatment
The treatment depends largely on the underlying cause. However, the root cause of papilledema is the increased intracranial pressure (ICP). This is a dangerous sign, indicative of a brain tumor, CNS inflammation or idiopathic intracranial hypertension (IIH) that may become manifest in the near future.
Thus, a biopsy is routinely performed prior to the treatment in the initial stages of papilledema to detect whether a brain tumor is present. If detected, laser treatment, radiation and surgeries can be used to treat the tumor.
To decrease ICP, medications can be administered by increasing the absorption of Cerebrospinal fluid (CSF), or decreasing its production. Such medicines include diuretics like acetazolamide and lasix. These diuretics, along with surgical interventions, can also treat IIH. In IIH, weight loss (even a loss of 10-15%) can lead to normalization of ICP.
Meanwhile, steroids can reduce inflammation (if this is a contributing factor to increased ICP), and may help to prevent vision loss. However, steroids have also been known to cause increased ICP, especially with a change in dosage. However, if a severe inflammatory condition exist, such as multiple sclerosis, steroids with anti-inflammatory effects such as Methylprednisolone and prednisone can help.
Other treatments include repeated lumbar punctures to remove excess spinal fluid in the cranium. The removal of potentially causative medicines including tetracyclines and vitamin A analogues may help decrease ICP, however this is only necessary if the medication is truly felt to contribute to ICP increase.
References
- ^ Cameron AJ (1933). "Marked papilloedema in pulmonary emphysema". Br J Ophthalmol 17 (3): 167–9. doi:10.1136/bjo.17.3.167. PMC 511527. PMID 18169104. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=511527. Full text at PMC: 511527
External links
Categories:- Disorders of optic nerve and visual pathways
Wikimedia Foundation. 2010.