- Internuclear ophthalmoplegia
-
Internuclear ophthalmoplegia Classification and external resources 
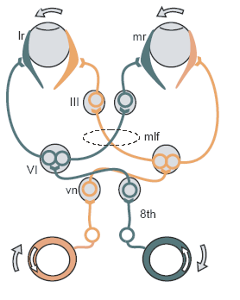
Schematic demonstrating right internuclear ophthalmoplegia, caused by injury of the right medial longitudinal fasciculus.ICD-10 H51.2 ICD-9 378.86 DiseasesDB 6853 Internuclear ophthalmoplegia (INO) is a disorder of conjugate lateral gaze in which the affected eye shows impairment of adduction. When an attempt is made to gaze contralaterally (relative to the affected eye), the affected eye adducts minimally, if at all. The contralateral eye abducts, however with nystagmus. Additionally, the divergence of the eyes leads to horizontal diplopia. That is, if the right eye is affected the patient will "see double" when looking to the left, seeing two images side-by-side. Convergence is generally preserved.
Contents
Causes
The disorder is caused by injury or dysfunction in the medial longitudinal fasciculus (MLF), a heavily-myelinated tract that allows conjugate eye movement by connecting the paramedian pontine reticular formation (PPRF) -abducens nucleus complex of contralateral side to the oculomotor nucleus of the ipsilateral side.
In young patients with bilateral INO, multiple sclerosis is often the cause. In older patients with one-sided lesions a stroke is a distinct possibility. Other causes are possible.[1]
Variants
A rostral lesion within the midbrain may affect the convergence center thus causing bilateral divergence of the eyes which is known as the WEBINO syndrome ( Wall Eyed Bilateral INO)[2] as each eye looks at the opposite "wall".
If the lesion affects the PPRF (or the abducens nucleus) and the MLF on the same side (the MLF having crossed from the opposite side)then the "one and a half syndrome" occurs which, simply put, involves paralysis of all conjugate horizontal eye movements other than abduction of the eye on the opposite side to the lesion.
References
- ^ Keane JR (May 2005). "Internuclear ophthalmoplegia: unusual causes in 114 of 410 patients". Arch. Neurol. 62 (5): 714–7. doi:10.1001/archneur.62.5.714. PMID 15883257. http://archneur.ama-assn.org/cgi/pmidlookup?view=long&pmid=15883257.
- ^ Lana MA, Moreira PR, Neves LB (December 1990). "Wall-eyed bilateral internuclear ophthalmoplegia (Webino syndrome) and myelopathy in pyoderma gangrenosum". Arq Neuropsiquiatr 48 (4): 497–501. PMID 2094199.
External links
- 1611005961 at GPnotebook
- Animation at mrcophth.com
Lesions of spinal cord and brain Spinal cord/
vascular myelopathysensory: Sensory ataxia · Tabes dorsalis
motor: Motor neurone disease
mixed: Brown-Séquard syndrome · cord syndrome (Posterior, Anterior, Central/Syringomyelia) · Subacute combined degeneration of spinal cord (B12) · Cauda equina syndrome
Anterior spinal artery syndromeBrainstem Lateral pontine syndrome (AICA) (lateral) · Medial pontine syndrome/Millard-Gubler syndrome (basilar)/Foville's syndrome (dorsal, basilar) · Locked-in syndrome (ventral) · Internuclear ophthalmoplegia · One and a half syndromeWeber's syndrome (ventral peduncle, PCA) · Benedikt syndrome (ventral tegmentum, PCA) · Parinaud's syndrome (dorsal, tumor) · Nothnagel's syndrome · Claude's syndromeOtherCerebellum Basal ganglia Cortex ACA syndrome · MCA syndrome · PCA syndrome
frontal lobe: Expressive aphasia · Abulia
parietal lobe: Receptive aphasia · Hemispatial neglect · Gerstmann syndrome · Astereognosis
occipital lobe: Balint's syndrome · Cortical blindness · Pure alexia
temporal lobe: Cortical deafness · ProsopagnosiaOther Categories:- Disorders of ocular muscles, binocular movement, accommodation and refraction
Wikimedia Foundation. 2010.