- Parinaud's syndrome
-
Not to be confused with Parinaud's oculoglandular syndrome.
Parinaud's syndrome Classification and external resources 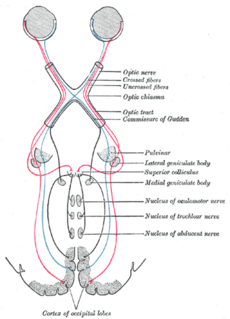
ICD-10 G46.3 ICD-9 378.81 DiseasesDB 32982 MeSH D015835 Parinaud's Syndrome, also known as dorsal midbrain syndrome is a group of abnormalities of eye movement and pupil dysfunction. It is caused by lesions of the upper brain stem and is named for Henri Parinaud[1][2] (1844–1905), considered to be the father of French ophthalmology. It is also one of the clinical manifestations of Bartonella infection.
Contents
Signs and symptoms
Parinaud's Syndrome is a cluster of abnormalities of eye movement and pupil dysfunction, characterized by:
- Paralysis of upgaze: Downward gaze is usually preserved. This vertical palsy is supranuclear, so doll's head maneuver should elevate the eyes, but eventually all upward gaze mechanisms fail.[3]
- Pseudo-Argyll Robertson pupils: Accommodative paresis ensues, and pupils become mid-dilated and show light-near dissociation.
- Convergence-Retraction nystagmus: Attempts at upward gaze often produce this phenomenon. On fast up-gaze, the eyes pull in and the globes retract. The easiest way to bring out this reaction is to ask the patient to follow down-going stripes on an optokinetic drum.
- Eyelid retraction (Collier's sign)
- Conjugate down gaze in the primary position: "setting-sun sign". Neurosurgeons will often see this sign most commonly in patients with failed ventriculoperitoneal shunts.
It is also commonly associated with bilateral papilledema. It has less commonly been associated with spasm of accommodation on attempted upward gaze, pseudoabducens palsy (also known as thalamic esotropia) or slower movements of the abducting eye than the adducting eye during horizontal saccades, see-saw nystagmus and associated ocular motility deficits including skew deviation, oculomotor nerve palsy, trochlear nerve palsy and internuclear ophthalmoplegia.
Causes

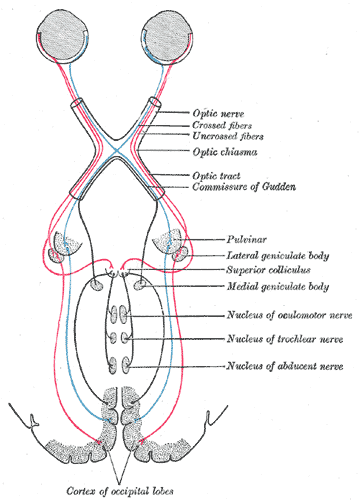
Parinaud's Syndrome results from injury, either direct or compressive, to the dorsal midbrain. Specifically, compression or ischemic damage of the mesencephalic tectum, including the superior colliculus adjacent oculomotor (origin of cranial nerve III) and Edinger-Westphal nuclei, causing dysfunction to the motor function of the eye.
Classically, it has been associated with three major groups:
- Young patients with brain tumors in the pineal gland or midbrain: pinealoma (intracranial germinomas) are the most common lesion producing this syndrome.
- Women in their 20s-30s with multiple sclerosis
- Older patients following stroke of the upper brainstem
However, any other compression, ischemia or damage to this region can produce these phenomena: obstructive hydrocephalus, midbrain hemorrhage, cerebral arteriovenous malformation, trauma and brainstem toxoplasmosis infection. Neoplasms and giant aneurysms of the posterior fossa have also been associated with the midbrain syndrome.
Vertical supranuclear ophthalmoplegia has also been associated with metabolic disorders, such as Niemann-Pick disease, Wilson's disease, kernicterus, and barbiturate overdose.
Prognosis and Treatment
The eye findings of Parinaud's Syndrome generally improve slowly over months, especially with resolution of the causative factor; continued resolution after the first 3-6 months of onset is uncommon. However, rapid resolution after normalization of intracranial pressure following placement of a ventriculoperitoneal shunt has been reported.
Treatment is primarily directed towards etiology of the dorsal midbrain syndrome. A thorough workup, including neuroimaging is essential to rule out anatomic lesions or other causes of this syndrome. Visually significant upgaze palsy can be relieved with bilateral inferior rectus recessions. Retraction nystagmus and convergence movement are usually improved with this procedure as well.
References
- ^ synd/1906 at Who Named It?
- ^ H. Parinaud. Paralysie des mouvements associés des yeux. Archives de neurologie, Paris, 1883, 5: 145-172.
- ^ [1] Neuro-Opthalmic Examination
External links
- Aguilar-Rebolledo F, Zárate-Moysén A, Quintana-Roldán G (1998). "Parinaud's syndrome in children" (in Spanish; Castilian). Rev. Invest. Clin. 50 (3): 217–20. PMID 9763886.
- Waga S, Okada M, Yamamoto Y (1979). "Reversibility of Parinaud syndrome in thalamic hemorrhage". Neurology 29 (3): 407–9. PMID 571990.
- -1268056053 at GPnotebook
Categories:- Medical signs
- Diseases of the eye and adnexa

Wikimedia Foundation. 2010.