- Cauda equina syndrome
Infobox_Disease
Name = PAGENAME
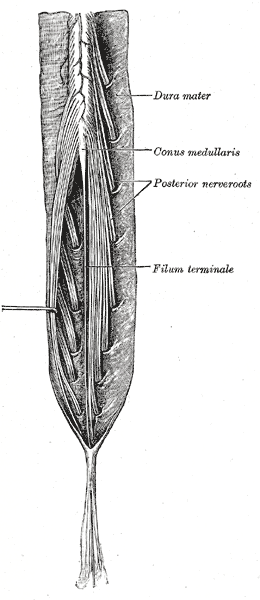
Caption = Cauda equina andfilum terminale seen from behind.
Width = 150
DiseasesDB = 31115
ICD10 = ICD10|G|83|4|g|80
ICD9 = ICD9|344.6
ICDO =
OMIM =
MedlinePlus =
eMedicineSubj = emerg
eMedicineTopic = 85
eMedicine_mult = eMedicine2|orthoped|39
MeshName = Cauda+Equina+Syndrome
MeshNumber = C10.668.829.800.750.700"Cauda equina" syndrome is a serious neurologic condition in which there is acute loss of function of the neurologic elements (
nerve root s) of the spinal canal below the termination (conus) of the spinal cord.Causes
After the conus the canal contains a mass of nerves (the cauda equina" - "' ['horse tail'] '" - branches off the lower end of the spinal cord and contains the nerve roots from L1-5 and S1-5. The nerve roots from L4-S4 join in the sacral plexus which affects the sciatic nerve ) which travels caudally (toward the feet).
Any lesion which compresses or disturbs the function of the cauda equina may disable the nerves although the most common is a central disc prolapse.
Metastatic disease should be suspected in every patient with weight loss and cauda equina syndrome. [cite journal
author=Walid MS, Ajjan M, Johnston KW, Robinson JS.
title=Cauda Equina Syndrome--Think of Cancer
journal=The Permanente Journal.
volume=12
issue=2
pages=48–51
year=2008
issn=1552-5767
pmid=
doi=]igns
Signs include weakness of the muscles innervated by the compressed roots (often
paraplegia ), sphincter weaknesses causing urinary retention and post-void residualincontinence as assessed bycatheterizing after the patient hasvoided .Also, there may be decreased rectal tone;sexual dysfunction ;saddle anesthesia ; bilateralleg pain and weakness; and bilateral absence of ankle reflexes. Pain may, however, be wholly absent; the patient may complain only of lack of bladder control and of saddle-anaesthesia, and may walk into the consulting-room.Diagnosis is usually confirmed by an
MRI scan orCT scan , depending on availability. If cauda equina syndrome exists, surgery is an option depending on the etiology discovered and the patient's candidacy for major spine surgery.Treatment/management
The management of true cauda equina syndrome frequently involves surgical decompression.
Cauda equina syndrome of sudden onset is regarded as a medical emergency. Surgical decompression by means of laminectomy or other approaches may be undertaken within 48 hours of symptoms developing if a compressive lesion, e.g. ruptured disc, epidural abscess, tumor or hematoma is demonstrated. This treatment may significantly improve the chance that long-term neurological damage will be avoided. There are, however, no evidence-based medical standards that address the question of ultra-early versus delayed (48 hours) surgical decompression in cauda equina syndrome due to ruptured lumbar disc.
Prognosis
The prognosis for complete recovery is dependent upon many factors. The most important of these factors is the severity and duration of compression upon the damaged nerve(s). As a general rule the longer the interval of time before intervention to remove the compression causing nerve damage the greater the damage caused to the nerve(s).
Damage can be so severe and/or prolonged that nerve regrowth is impossible. In such cases the nerve damage will be permanent. In cases where the nerve(s) has been damaged but is still capable of regrowth, recovery time is widely variable. Quick surgical intervention can lead to complete recovery almost immediately afterward. Delayed or severe nerve damage can mean up to several years recovery time because nerve growth is exceptionally slow.
References
External links
*
*
* [http://www.apparelyzed.com Spinal Cord Injury Peer Support]
Wikimedia Foundation. 2010.