- Cerebral hemorrhage
-
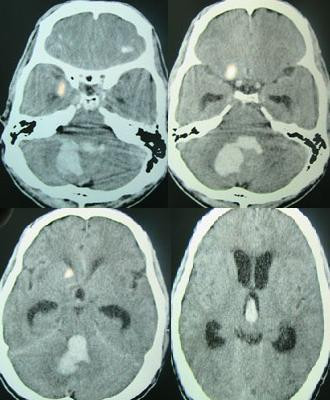
Cerebral hemorrhage Classification and external resources File:Intracerebral heamorrage
Cerebral hemorrhageICD-10 I61, P10.1 ICD-9 431 MeSH D002543 A cerebral hemorrhage or hemorrhage (or intracerebral hemorrhage, ICH) is a subtype of intracranial hemorrhage that occurs within the brain tissue itself. Intracerebral hemorrhage can be caused by brain trauma, or it can occur spontaneously in hemorrhagic stroke. Non-traumatic intracerebral hemorrhage is a spontaneous bleeding into the brain tissue.[1]
A cerebral hemorrhage is an intra-axial hemorrhage; that is, it occurs within the brain tissue rather than outside of it. The other category of intracranial hemorrhage is extra-axial hemorrhage, such as epidural, subdural, and subarachnoid hematomas, which all occur within the skull but outside of the brain tissue. There are two main kinds of intra-axial hemorrhages: intraparenchymal hemorrhage and intraventricular hemorrhages. As with other types of hemorrhages within the skull, intraparenchymal bleeds are a serious medical emergency because they can increase intracranial pressure, which if left untreated can lead to coma and death. The mortality rate for intraparenchymal bleeds is over 40%.[2]
Contents
Signs and symptoms
Patients with intraparenchymal bleeds have symptoms that correspond to the functions controlled by the area of the brain that is damaged by the bleed.[3] Other symptoms include those that indicate a rise in intracranial pressure due to a large mass putting pressure on the brain.[3] Intracerebral hemorrhages are often misdiagnosed as subarachnoid hemorrhages due to the similarity in symptoms and signs. A severe headache followed by vomiting is one of the more common symptoms of intracerebral hemorrhage. Some patients may also go into a coma before the bleed is noticed.
Causes

Intracerebral bleeds are the second most common cause of stroke, accounting for 30–60% of hospital admissions for stroke.[1] High blood pressure raises the risks of spontaneous intracerebral hemorrhage by two to six times.[1] More common in adults than in children, intraparenchymal bleeds due to trauma are usually due to penetrating head trauma, but can also be due to depressed skull fractures. Acceleration-deceleration trauma,[4][5][6] rupture of an aneurysm or arteriovenous malformation (AVM), and bleeding within a tumor are additional causes. Amyloid angiopathy is a not uncommon cause of intracerebral hemorrhage in patients over the age of 55. A very small proportion is due to cerebral venous sinus thrombosis. Infection with the k serotype of Streptococcus mutans may also be a risk factor, due to its prevalence in stroke patients and production of collagen-binding protein.[7]
Risk factors for ICH include:[8]
- Hypertension
- Diabetes
- Menopause
- Current cigarette smoking
- Alcoholic drinks (≥2/day)
Diagnosis

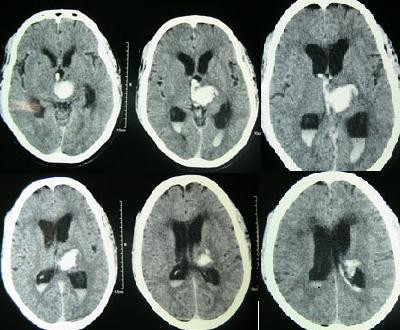
Intraparenchymal hemorrhage can be recognized on CT scans because blood appears brighter than other tissue and is separated from the inner table of the skull by brain tissue. The tissue surrounding a bleed is often less dense than the rest of the brain due to edema, and therefore shows up darker on the CT scan.
Treatment
Treatment depends substantially of the type of ICH. Rapid CT scan and other diagnostic measures are used to determine proper treatment, which may include both medication and surgery.
Medication
- Antihypertensive therapy in acute phases. The AHA/ASA and EUSI guidelines (American Heart Association/American Stroke Association guidelines and the European Stroke Initiative guidelines) have recommended antihypertensive therapy to stabilize the mean arterial pressure at 110 mmHg. One paper showed the efficacy of this antihypertensive therapy without worsening outcome in patients of hypertensive intracerebral hemorrhage within 3 hours onset. [9]
- Giving Factor VIIa within 4 hours limits the bleeding and formation of a hematoma. However, it also increases the risk of thromboembolism.[10]
- Mannitol is effective in acutely reducing raised intracranial pressure.
- Acetaminophen may be needed to avoid hyperthermia, and to relieve headache.[10]
- Frozen plasma, vitamin K, protamine, or platelet transfusions are given in case of a coagulopathy.[10]
- Fosphenytoin or other anticonvulsant is given in case of seizures or lobar hemorrhage.[10]
- H2 antagonists or proton pump inhibitors are commonly given for stress ulcer prophylaxis, a condition somehow linked with ICH.[10]
- Corticosteroids, in concert with antihypertensives, reduces swelling.[11]
Surgery
Surgery is required if the hematoma is greater than 3 cm, if there is a structural vascular lesion or lobar hemorrhage in a young patient.[10]
- A catheter may be passed into the brain vasculature to close off or dilate blood vessels, avoiding invasive surgical procedures.[12]
- Aspiration by stereotactic surgery or endoscopic drainage may be used in basal ganglia hemorrhages, although successful reports are limited.[10]
Other treatment
- Tracheal intubation is indicated in patients with decreased level of consciousness or other risk of airway obstruction.[10]
- IV fluids are given to maintain fluid balance, using normotonic rather than hypotonic fluids.[10]
Prognosis
The risk of death from an intraparenchymal bleed in traumatic brain injury is especially high when the injury occurs in the brain stem.[2] Intraparenchymal bleeds within the medulla oblongata are almost always fatal, because they cause damage to cranial nerve X, the vagus nerve, which plays an important role in blood circulation and breathing.[4] This kind of hemorrhage can also occur in the cortex or subcortical areas, usually in the frontal or temporal lobes when due to head injury, and sometimes in the cerebellum.[4][13]
For spontaneous ICH seen on CT scan, the death rate (mortality) is 34–50% by 30 days after the insult,[1] and half of the deaths occur in the first 2 days.[14]
The inflammatory response triggered by stroke has been viewed as harmful, focusing on the influx and migration of blood-borne leukocytes, neutrophils, and macrophages. New area of interest are the Mast Cells.[15]
Epidemiology
It accounts for 20% of all cases of cerebrovascular disease in the US, behind cerebral thrombosis (40%) and cerebral embolism (30%).[16]
It is two or more times more prevalent in black American patients than it is in white.[17]
References
- ^ a b c d e f (? this looks wrong) Yadav YR, Mukerji G, Shenoy R, Basoor A, Jain G, Nelson A (2007). "Endoscopic management of hypertensive intraventricular haemorrhage with obstructive hydrocephalus". BMC Neurol 7: 1. doi:10.1186/1471-2377-7-1. PMC 1780056. PMID 17204141. http://www.biomedcentral.com/1471-2377/7/1.
- ^ a b Sanders MJ and McKenna K. 2001. Mosby’s Paramedic Textbook, 2nd revised Ed. Chapter 22, "Head and Facial Trauma." Mosby.
- ^ a b Vinas FC and Pilitsis J. 2006. "Penetrating Head Trauma." Emedicine.com.
- ^ a b c McCaffrey P. 2001. "The Neuroscience on the Web Series: CMSD 336 Neuropathologies of Language and Cognition." California State University, Chico. Retrieved on June 19, 2007.
- ^ Orlando Regional Healthcare, Education and Development. 2004. "Overview of Adult Traumatic Brain Injuries." Retrieved on 2008-01-16.
- ^ Shepherd S. 2004. "Head Trauma." Emedicine.com. Retrieved on June 19, 2007.
- ^ Kazuhiko Nakano et al.. "The collagen-binding protein of Streptococcus mutans is involved in haemorrhagic stroke". Nature Communications. http://www.nature.com/ncomms/journal/v2/n9/full/ncomms1491.html.
- ^ Major Risk Factors for Intracerebral Hamorrhage in the Young Are Modifiable Edward Feldmann, MD; Joseph P. Broderick, MD; Walter N. Kernan, MD; Catherine M. Viscoli, PhD; Lawrence M. Brass, MD; Thomas Brott, MD; Lewis B. Morgenstern, MD; Janet Lee Wilterdink, MD Ralph I. Horwitz, MD. Published in Stroke. 2005;36:1881.
- ^ Fujii M et al. J Clin Neurosci 17:1136-9,2010 PMID:20541417
- ^ a b c d e f g h i eMedicine Specialties > Neurology > Neurological Emergencies > Intracranial Haemorrhage: Treatment & Medication. By David S Liebeskind, MD. Updated: Aug 7, 2006
- ^ MedlinePlus - Intracerebral haemorrhage Update Date: 7/14/2006. Updated by: J.A. Lee, M.D.
- ^ Cedars-Sinai Health System - Cerebral Hemorrhages Retrieved on 02/25/2009
- ^ Graham DI and Gennareli TA. Chapter 5, "Pathology of Brain Damage After Head Injury" Cooper P and Golfinos G. 2000. Head Injury, 4th Ed. Morgan Hill, New York.
- ^ Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults
- ^ [1] Lindsberg e.a.: Mast cells as early responders in the regulation of acute blood–brain barrier changes after cerebral ischemia and hemorrhage
- ^ Page 117 in: Henry S. Schutta; Lechtenberg, Richard (1998). Neurology practice guidelines. New York: M. Dekker. ISBN 0-8247-0104-6.
- ^ Copenhaver BR, Hsia AW, Merino JG, et al. (October 2008). "Racial differences in microbleed prevalence in primary intracerebral hemorrhage". Neurology 71 (15): 1176–82. doi:10.1212/01.wnl.0000327524.16575.ca. PMC 2676986. PMID 18838665. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2676986.
External links
- Parent friendly information on IVH in premature babies from The Hospital for Sick Children
- LPCH on Intraventricular
- Information on brain haemorrhage from Headway - the brain injury association UK based charity providing information and support
CNS disease, Vascular disease: Cerebrovascular diseases (G45–G46 and I60–I69, 430–438) Brain ischemia/
cerebral infarction
(ischemic stroke/TIA)Intracranial hemorrhage
(hemorrhagic stroke)Extra-axialCerebral/Intra-axialBrainstemAneurysm Other/general Neurotrauma (S06, Sx4, T09.3–4, 850–854, 950–957) Traumatic brain injury Intracranial hemorrhage/hematoma: intra-axial (Intraparenchymal hemorrhage, Intraventricular hemorrhage) · extra-axial (Subdural hematoma, Epidural hematoma, Subarachnoid hemorrhage)Spinal cord injury PNS Nerve injury (Peripheral nerve injury), Wallerian degenerationCategories:- Neurotrauma
- Stroke
- Cerebrovascular diseases
Wikimedia Foundation. 2010.