- CADASIL syndrome
-
CADASIL syndrome, (a very serious and dangerous disease occurring in the ages between 40-50) Classification and external resources 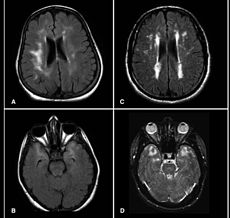
Brain MRI from patients with CADASIL showing multiple lesions.OMIM 125310 DiseasesDB 2161 MeSH D046589 CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) is the most common form of hereditary stroke disorder, and is thought to be caused by mutations of the Notch 3 gene on chromosome 19.[1] The disease belongs to a family of disorders called the Leukodystrophies. The most common clinical manifestations are migraine headaches and transient ischemic attacks or strokes, which usually occur between 40 and 50 years of age, although MRI is able to detect signs of the disease years prior to clinical manifestation of disease.[2][3]
Contents
Pathophysiology
The underlying pathology of CADASIL is progressive degeneration of the smooth muscle cells in blood vessels. Mutations in the Notch 3 gene (on the short arm of chromosome 19) cause an abnormal accumulation of Notch 3 at the cytoplasmic membrane of vascular smooth-muscle cells both in cerebral and extracerebral vessels,[4] seen as granular osmiophilic deposits on electron microscopy.[5]
Interestingly, the Notch 3 gene is in the same locus as the gene for familial hemiplegic migraine.
Clinical features
CADASIL may start with attacks of migraine with aura or subcortical transient ischemic attacks or strokes, or mood disorders between 35 to 55 years of age. The disease progresses to subcortical dementia associated with pseudobulbar palsy and urinary incontinence.
Diagnosis
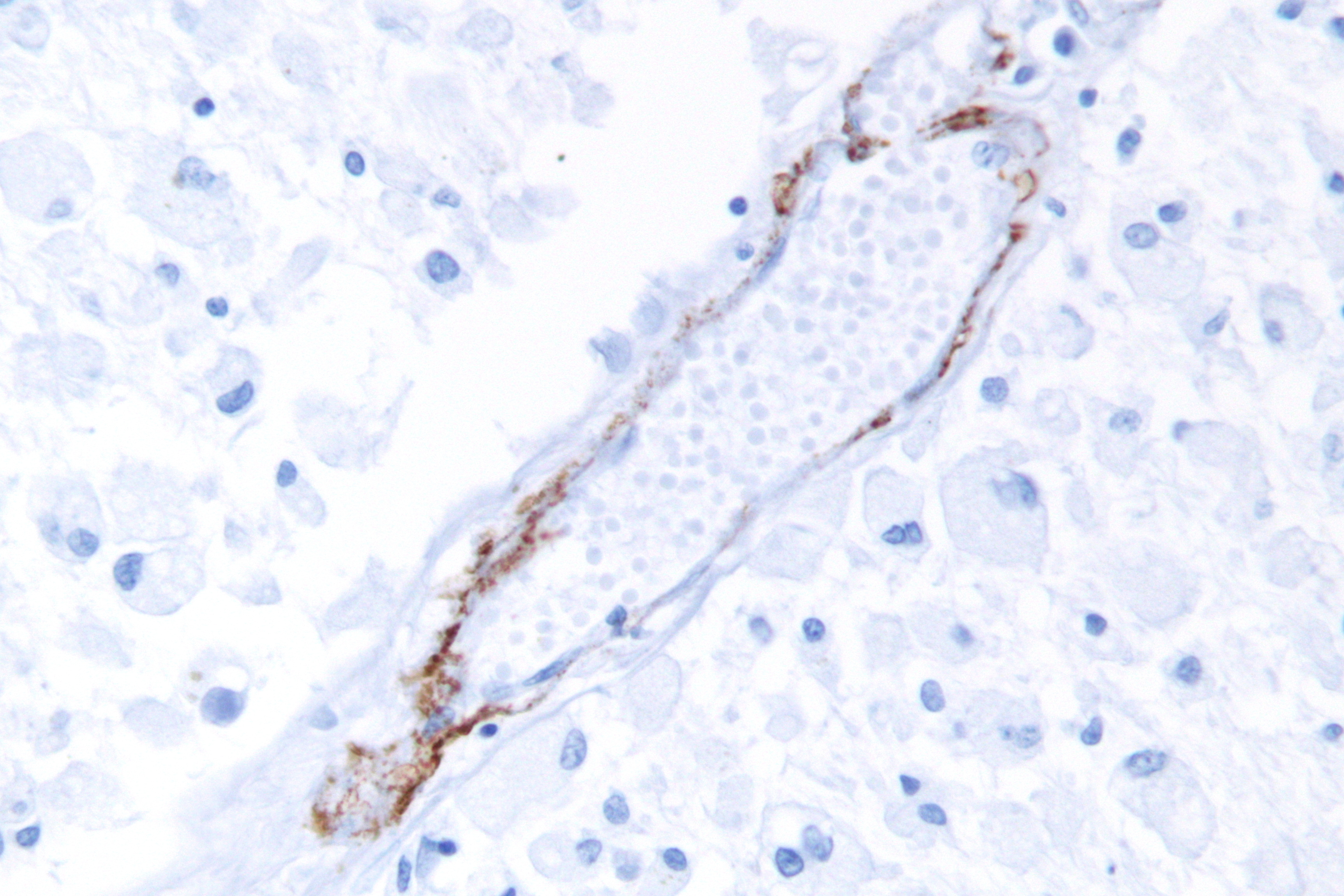
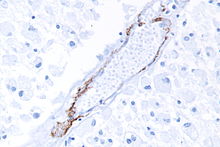 A micrograph showing punctate immunostaining (brown) with a Notch 3 antibody, as is characteristic in CADASIL.
A micrograph showing punctate immunostaining (brown) with a Notch 3 antibody, as is characteristic in CADASIL.
MRIs show hypointensities on T1-weighted images and hyperintensities on T2-weighted images, usually multiple confluent white matter lesions of various sizes, are characteristic. These lesions are concentrated around the basal ganglia, periventricular white matter, and the pons, and are similar to those seen in Binswanger disease.[2][6] These white matter lesions are also seen in asymptomatic individuals with the mutated gene.[7] While MRI is not used to diagnose CADASIL, it can show the progression of white matter changes even decades before onset of symptoms.
The definitive test is sequencing the whole Notch 3 gene, which can be done from a sample of blood. However, as this is quite expensive and CADASIL is a systemic arteriopathy, evidence of the mutation can be found in small and medium-sized arteries. Therefore, skin biopsies are often used for the diagnosis.[8][9]
Clinical course
Ischemic strokes are the most frequent presentation of CADASIL, with approximately 85% of symptomatic individuals developing transient ischemic attacks or stroke(s). The mean age of onset of ischemic episodes is approximately 46 years (range 30–70). A classic lacunar syndrome occurs in at least two-thirds of affected patients while hemispheric strokes are much less common. Notably, ischemic strokes typically occur in the absence of traditional cardiovascular risk factors. Recurrent silent strokes, with or without clinical strokes, often lead to cognitive decline and overt subcortical dementia.
Treatment
No specific treatment is available. However, anti-platelet agents such as aspirin, Aggrenox, or clopidogrel might slow down the disease and help prevent strokes. Given the propensity for cardiovascular and cerebrovascular complications, minimizing vascular risk factors and implementing therapy for primary or secondary prevention of stroke and myocardial infarction seems prudent. Stopping oral contraceptive pills is justified particularly in cases with migraine with aura. Aggressive treatment of hypercholesterolemia and hypertension is reasonable although the utility of statins and antihypertensive agents in the absence cardiovascular risk factors is unknown. Homocysteine levels are elevated in CADASIL and treatment with folic acid is reasonable. Anti-platelet therapy appears justifiable whereas anticoagulation may be inadvisable given the propensity for microhemorrhages. Administering tPA following onset of stroke is not advised for CADASIL patients, due to increased risk of microhemorrhages. Warfarin (Coumadin) should be avoided. Some CADASIL patients have used L-Arginine, a naturally occurring amino acid, to ease symptoms such as headache. Aricept, normally used for Alzheimer's Disease, has been shown to improve executive functioning in CADASIL patients.
In popular culture
John Ruskin has been suggested to have suffered from CADASIL[10] The visual disturbances this caused was reported by Ruskin in his diaries, and it has also been suggested that it might have been a factor in causing him to describe James Whistler's Nocturne in Black and Gold – The Falling Rocket as "ask[ing] two hundred guineas for throwing a pot of paint in the public's face". This resulted in the famous libel trial that resulted in a jury awarding Whistler one farthing damages.[10]
The character Julia, in the 2004 Spanish film The Sea Inside, has the condition.
Patient Support
A website has recently been developed to provide information to patients and those caring for individuals diagnosed with CADASIL. (www.cadasil.co.uk)
See also
References
- ^ Joutel A, Corpechot C, Ducros A, et al. (October 1996). "Notch3 mutations in CADASIL, a hereditary adult-onset condition causing stroke and dementia". Nature 383 (6602): 707–10. doi:10.1038/383707a0. PMID 8878478.
- ^ a b Chabriat H, Vahedi K, Iba-Zizen MT, et al. (October 1995). "Clinical spectrum of CADASIL: a study of 7 families. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy". Lancet 346 (8980): 934–9. PMID 7564728.
- ^ James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. p. 545. ISBN 0-7216-2921-0.
- ^ Joutel A, Andreux F, Gaulis S, et al. (March 2000). "The ectodomain of the Notch3 receptor accumulates within the cerebrovasculature of CADASIL patients". J. Clin. Invest. 105 (5): 597–605. doi:10.1172/JCI8047. PMC 289174. PMID 10712431. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=289174.
- ^ Ruchoux MM, Guerouaou D, Vandenhaute B, Pruvo JP, Vermersch P, Leys D (1995). "Systemic vascular smooth muscle cell impairment in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy". Acta Neuropathol. 89 (6): 500–12. doi:10.1007/BF00571504. PMID 7676806.
- ^ Ropper AH, Brown RH, ed (2005). "Cerebrovascular Diseases". Adams and Victor's Principles of Neurology. New York: McGraw-Hill. ISBN 007141620.
- ^ Tournier-Lasserve E, Joutel A, Melki J, et al. (March 1993). "Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy maps to chromosome 19q12". Nat. Genet. 3 (3): 256–9. doi:10.1038/ng0393-256. PMID 8485581.
- ^ Joutel A, Favrole P, Labauge P, et al. (December 2001). "Skin biopsy immunostaining with a Notch3 monoclonal antibody for CADASIL diagnosis". Lancet 358 (9298): 2049–51. doi:10.1016/S0140-6736(01)07142-2. PMID 11755616.
- ^ Ueda M, Nakaguma R, Ando Y (March 2009). "[Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)]" (in Japanese). Rinsho Byori 57 (3): 242–51. PMID 19363995.
- ^ a b Kempster PA, Alty JE (September 2008). "John Ruskin's relapsing encephalopathy". Brain 131 (Pt 9): 2520–5. doi:10.1093/brain/awn019. PMID 18287121. http://brain.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=18287121.
External links
- The CADASIL Foundation
- United Leukodystrophy Foundation: CADASIL
- GeneReviews/NCBI/NIH/UW entry on CADASIL
CNS disease, Vascular disease: Cerebrovascular diseases (G45–G46 and I60–I69, 430–438) Brain ischemia/
cerebral infarction
(ischemic stroke/TIA)Intracranial hemorrhage
(hemorrhagic stroke)Extra-axialBrainstemAneurysm Other/general Categories:- Deficiencies of intracellular signaling peptides and proteins
- Neurological disorders
- Skin conditions resulting from errors in metabolism

Wikimedia Foundation. 2010.