- Hyaluronan
-
Hyaluronan 
Identifiers CAS number 9004-61-9  ,
,
31799-91-4 (potassium salt)
9067-32-7 (sodium salt)ChemSpider 2341172 UNII S270N0TRQY Jmol-3D images Image 1 - [Na+].O=C(N[C@H]4[C@H](O)O[C@H](CO)[C@@H](O)[C@@H]4O[C@@H]3O[C@H](C(=O)O)[C@@H](O[C@@H]2O[C@@H]([C@@H](O)[C@H](O[C@@H]1O[C@H](C(=O)O)[C@@H](O)[C@H](O)[C@H]1O)[C@H]2NC(=O)C)CO)[C@H](O)[C@H]3O)C
- InChI=1S/C28H44N2O23.Na/c1-5(33)29-9-18(11(35)7(3-31)47-25(9)46)49-28-17(41)15(39)20(22(53-28)24(44)45)51-26-10(30-6(2)34)19(12(36)8(4-32)48-26)50-27-16(40)13(37)14(38)21(52-27)23(42)43;/h7-22,25-28,31-32,35-41,46H,3-4H2,1-2H3,(H,29,33)(H,30,34)(H,42,43)(H,44,45);/q;+1/t7-,8-,9-,10-,11-,12-,13+,14+,15-,16-,17-,18-,19-,20+,21+,22+,25-,26+,27-,28-;/m1./s1
Key: YWIVKILSMZOHHF-QJZPQSOGSA-N
InChI=1/C28H44N2O23.Na/c1-5(33)29-9-18(11(35)7(3-31)47-25(9)46)49-28-17(41)15(39)20(22(53-28)24(44)45)51-26-10(30-6(2)34)19(12(36)8(4-32)48-26)50-27-16(40)13(37)14(38)21(52-27)23(42)43;/h7-22,25-28,31-32,35-41,46H,3-4H2,1-2H3,(H,29,33)(H,30,34)(H,42,43)(H,44,45);/q;+1/t7-,8-,9-,10-,11-,12-,13+,14+,15-,16-,17-,18-,19-,20+,21+,22+,25-,26+,27-,28-;/m1./s1
Key: YWIVKILSMZOHHF-QJZPQSOGBN
Properties Molecular formula (C14H21NO11)n Solubility in water soluble (sodium salt) Hazards S-phrases S22, S24/25 (sodium salt) LD50 > 2400 mg/kg (mouse, oral, sodium salt)
>4000 mg/kg (mouse, subcutaneous, sodium salt)
1500 mg/kg (mouse, intraperitoneal, sodium salt) [1]Related compounds Related compounds D-glucuronic acid and D-N-acetylglucosamine (monomers)  (verify) (what is:
(verify) (what is:  /
/ ?)
?)
Except where noted otherwise, data are given for materials in their standard state (at 25 °C, 100 kPa)Infobox references Hyaluronan (also called hyaluronic acid or hyaluronate) is an anionic, nonsulfated glycosaminoglycan distributed widely throughout connective, epithelial, and neural tissues. It is unique among glycosaminoglycans in that it is nonsulfated, forms in the plasma membrane instead of the Golgi, and can be very large, with its molecular weight often reaching the millions.[2] One of the chief components of the extracellular matrix, hyaluronan contributes significantly to cell proliferation and migration, and may also be involved in the progression of some malignant tumors.
The average 70 kg (154 lbs) person has roughly 15 grams of hyaluronan in the body, one-third of which is turned over (degraded and synthesized) every day.[3] Hyaluronic acid is also a component of the group A streptococcal extracellular capsule,[4] and is believed to play a role in virulence.[5][6]
Functions
It was first isolated from the vitreous body of the eye by Karl Meyer who called it hyaluronic acid, in 1934.The term hyaluronan was proposed by Dr. Endre A. Balazs in the 1980’s to encompass the different forms the molecule can take, e.g., the acid form, hyaluronic acid, and the salts, such as sodium hyaluronate, which form at physiological pH[7]. Until the late 1970's, “The polysaccharide of the vitreous humor,” , hyaluronan was described as a "goo" molecule, a ubiquitous carbohydrate polymer that is part of the extracellular matrix.[8] For example, hyaluronan is a major component of the synovial fluid, and was found to increase the viscosity of the fluid. Along with lubricin, it is one of the fluid's main lubricating components. [9]
What makes hyaluronan unique?Hyaluronan is used in medical application for its unique physical/chemical properties. It is very hydrophilic; its viscous solutions have most unusual rheological properties and are exceedingly lubricious.Hyaluronan is an important component of articular cartilage, where it is present as a coat around each cell (chondrocyte).[10] When aggrecan monomers bind to hyaluronan in the presence of link protein, large highly negatively-charged aggregates form. These aggregates imbibe water and are responsible for the resilience of cartilage (its resistance to compression). The molecular weight (size) of hyaluronan in cartilage decreases with age, but the amount increases.[11]
Hyaluronan is also a major component of skin, where it is involved in tissue repair. When skin is exposed to excessive UVB rays, it becomes inflamed (sunburn) and the cells in the dermis stop producing as much hyaluronan, and increase the rate of its degradation. Hyaluronan degradation products also accumulate in the skin after UV exposure.[12]
While it is abundant in extracellular matrices, hyaluronan also contributes to tissue hydrodynamics, movement and proliferation of cells, and participates in a number of cell surface receptor interactions, notably those including its primary receptors, CD44 and RHAMM. Upregulation of CD44 itself is widely accepted as a marker of cell activation in lymphocytes. Hyaluronan's contribution to tumor growth may be due to its interaction with CD44. Receptor CD44 participates in cell adhesion interactions required by tumor cells.
Although hyaluronan binds to receptor CD44, there is evidence hyaluronan degradation products transduce their inflammatory signal through toll-like receptor 2 (TLR2), TLR4 or both TLR2, and TLR4 in macrophages and dendritic cells. TLR and hyaluronan play a role in innate immunity.
High concentrations of hyaluronan in the brains of young rats, and reduced concentrations in the brains of adult rats suggest hyaluronan plays an important role in brain development.[13]
Structure
Properties of hyaluronan were first determined in the 1930s in the laboratory of Karl Meyer.[14]
Hyaluronan is a polymer of disaccharides, themselves composed of D-glucuronic acid and D-N-acetylglucosamine, linked via alternating β-1,4 and β-1,3 glycosidic bonds. Hyaluronan can be 25,000 disaccharide repeats in length. Polymers of hyaluronan can range in size from 5,000 to 20,000,000 Da in vivo. The average molecular weight in human synovial fluid is 3−4 million Da, and hyaluronan purified from human umbilical cord is 3,140,000 Da.[15]
Hyaluronan is energetically stable, in part because of the stereochemistry of its component disaccharides. Bulky groups on each sugar molecule are in sterically favored positions, whereas the smaller hydrogens assume the less-favorable axial positions.
Biological synthesis
Hyaluronan is synthesized by a class of integral membrane proteins called hyaluronan synthases, of which vertebrates have three types: HAS1, HAS2, and HAS3. These enzymes lengthen hyaluronan by repeatedly adding glucuronic acid and N-acetylglucosamine to the nascent polysaccharide as it is extruded via ABC-transporter through the cell membrane into the extracellular space.[16]
Hyaluronan synthesis (HAS) has been shown to be inhibited by 4-methylumbelliferone (hymecromone, heparvit), a 7-hydroxy-4-methylcoumarin derivative.[17] This selective inhibition (without inhibiting other glycosaminoglycans) may prove useful in preventing metastasis of malignant tumor cells.[18]
Bacillus Subtilis recently has been genetically modified (GMO) to culture a proprietary formula to yield hyaluronans,[19] in a patented process producing human-grade product.
Cell receptors for hyaluronan
So far, cell receptors that have been identified for HA fall into three main groups: CD44, Receptor for HA-mediated motility (RHAMM) and intracellular adhesion molecule-1 (ICAM-1). CD44 and ICAM-1 were already known as cell adhesion molecules with other recognized ligands before their HA binding was discovered.[20]
CD44 is widely distributed throughout the body, and the formal demonstration of HA-CD44 binding was proposed by Aruffo et al.[21] in 1990. To date, it is recognized as the main cell surface receptor for HA. CD44 mediates cell interaction with HA and the binding of the two functions as an important part in various physiologic events,[20][22] such as cell aggregation, migration, proliferation and activation; cell-cell and cell-substrate adhesion; endocytosis of HA, which leads to HA catabolism in macrophages; and assembly of petircellular matrices from HA and proteoglycan. Two significant roles of CD44 in skin were proposed by Kaya et al.[23] The first is regulation of keratinocyte proliferation in response to extracellular stimuli, and the second is the maintenance of local HA homeostasis.[22]
ICAM-1 is known mainly as a metabolic cell surface receptor for HA, and this protein may be responsible mainly for the clearance of HA from lymph and blood plasma, which accounts for perhaps most of its whole-body turnover [20][24] Ligand binding of this receptor, thus, triggers a highly coordinated cascade of events that includes the formation of an endocytotic vesicle, its fusion with primary lysosomes, enzymatic digestion to monosaccharides, active transmembrane transport of these sugars to cell sap, phosphorylation of GlcNAc and enzymatic deacetylation.[20][25][26] Like its name, ICAM-1 may also serve as a cell adhesion molecule, and the binding of HA to ICAM-1 may contribute to the control of ICAM-1-mediated inflammatory activation.[22]
Degradation
Hyaluronan is degraded by a family of enzymes called hyaluronidases. In humans, there are at least seven types of hyaluronidase-like enzymes, several of which are tumor suppressors. The degradation products of hyaluronan, the oligosaccharides and very low-molecular-weight hyaluronan, exhibit pro-angiogenic properties[citation needed]. In addition, recent studies showed hyaluronan fragments, not the native high-molecular mass of hyaluronan, can induce inflammatory responses in macrophages and dendritic cells in tissue injury and in skin transplant rejection[citation needed].
Role of hyaluronan on wound repair process
Skin provides a mechanical barrier to the external environment and acts to prevent the ingress of infectious agents.[27] Once injured, the tissues beneath are exposed to infection; therefore, rapid and effective healing is of crucial significance to reconstruct a barrier function. Skin wound healing is a complex process, and includes many interacting processes initiated by haemostasis and the release of platelet-derived factors.[27] The following stages are inflammation, granulation tissue formation, reepithelization and remodeling. HA is likely to play a multifaceted role in mediation of these cellular and matrix events. The proposed roles of HA in this sequence of skin wound healing events are elucidated in details below.
- Inflammation
Many biological factors, such as growth factors, cytokines, eicosanoids etc., are generated in the inflammation process. These factors are necessary for the subsequent steps of wound healing due to their roles in promoting migration of inflammatory cells, fibroblasts, and endothelial cells into the wound site.[22]
The wound tissue in the early inflammatory phase of wound repair is abundant in HA, probably a reflection of increased synthesis.[22] HA acts as a promoter of early inflammation, which is crucial in the whole skin wound-healing process. In a murine air pouch model of carrageenan/IL-1-induced inflammation, HA was observed to enhance cellular infiltration.[22][28] Kobayashi and colleagues [22][29] showed a dose-dependent increase of the proinflammatory cytokines TNF-α and IL-8 production by human uterine fibroblasts at HA concentrations of 10μg/ml to 1 mg/ml via a CD44-mediated mechanism. Endothelial cells, in response to inflammatory cytokines such as TNF-α, and bacterial lipopolysaccharide, also synthesize HA, which has been shown to facilitate primary adhesion of cytokine-activated lymphocytes expressing the HA-binding variants of CD44 under laminar and static flow conditions.[22][30] It is interesting to note that HA has contradictory dual functions in the inflammatory process. It not only can promote the inflammation, as stated above, but also can moderate the inflammatory response, which may contribute to the stabilization of granulation tissue matrix, as described in the following part.
- Granulation and organization of the granulation tissue matrix
Granulation tissue is the perfused, fibrous connective tissue that replaces a fibrin clot in healing wounds. It typically grows from the base of a wound and is able to fill wounds of almost any size it heals. HA is abundant in granulation tissue matrix. A variety of cell functions that are essential for tissue repair may attribute to this HA-rich network. These functions include facilitation of cell migration into the provisional wound matrix, cell proliferation and organization of the granulation tissue matrix.[22] Absolutely, initiation of inflammation is extremely crucial for the formation of granulation tissue, therefore the pro-inflammatory role of HA as discussed above also contribute to this stage of wound healing.[22]
- HA and cell migration
Cell migration is essential for the formation of granulation tissue.[22] The early stage of granulation tissue is dominated by a HA-rich extracellular matrix, which is regarded as a conducive environment for migration of cells into this temporary wound matrix. Contributions of HA to cell migration may attribute to its physicochemical properties as stated above, as well as its direct interactions with cells. For the former scenario, HA provides an open hydrated matrix that facilitates cell migration,[22] whereas, in the latter scenario, directed migration and control of the cell locomotory mechanisms are mediated via the specific cell interaction between HA and cell surface HA receptors. As discussed before, the three principal cell surface receptors for HA are CD44, RHAMM, and ICAM-1. RHAMM is more related to cell migration. It forms links with several protein kinases associated with cell locomotion, for example, extracellular signal-regulated protein kinase (ERK), p125fak, and pp60c-src.[31][32][33] During fetal development, the migration path through which neural crest cells migrate is rich in HA.[22] HA is closely associated with the cell migration process in granulation tissue matrix, and studies show that cell movement can be inhibited, at least partially, by HA degradation or blocking HA receptor occupancy.[34]
By providing the dynamic force to the cell, HA synthesis has also been shown to associate with cell migration.[35] Basically, HA is synthesized at the plasma membrane and released directly into the extracellular environment.[22] This may contribute to the hydrated microenvironment at sites of synthesis, and is essential for cell migration by facilitating cell detachment.
- Role of HA in moderation of the inflammatory response
Although inflammation is an integral part of granulation tissue formation, for normal tissue repair to proceed, inflammation needs to be moderated. The initial granulation tissue formed is highly inflammatory with a high rate of tissue turnover mediated by matrix degrading enzymes and reactive oxygen metabolites that are products of inflammatory cells.[22] Stabilization of granulation tissue matrix can be achieved by moderating inflammation. HA functions as an important moderator in this moderation process, which contradicts its role in inflammatory stimulation, as described above. HA can protect against free-radical damage to cells.[36] This may attribute to its free-radical scavenging property, a physicochemical characteristic shared by large polyionic polymers. In a rat model of free-radical scavenging property investigated by Foschi D. and colleagues, HA has been shown to reduce damage to the granulation tissue.[37]
In addition to the free-radical scavenging role, HA may also function in the negative feedback loop of inflammatory activation through its specific biological interactions with the biological constituents of inflammation.[22] TNF-α, an important cytokine generated in inflammation, stimulates the expression of TSG-6 (TNF-stimulated gene 6) in fibroblasts and inflammatory cells. TSG-6, a HA-binding protein, also forms a stable complex with the serum proteinase inhibitor IαI (Inter-α-inhibitor) with a synergistic effect on the latter’s plasmin-inhibitory activity. Plasmin is involved in activation of the proteolytic cascade of matrix metalloproteinases and other proteinases leading to inflammatory tissue damage. Therefore, the action of TSG-6/ IαI complex, which may be additionally organized by binding to HA in the extracellular matrix, may serve as a potent negative feedback loop to moderate inflammation and stabilize the granulation tissue as healing progresses.[22][38] In the murine air pouch model of carragenan/IL-1 (Interleukin-1β)-induced inflammation, where HA has been shown to have a proinflammatory property, reduction of inflammation can be achieved by administrating TSG-6, and the result is comparable with systemic dexamethasone treatment.
- Reepithelization
HA plays an important role in the normal epidermis. HA also has crucial functions in the reepithelization process due to several of its properties. It serves as an integral part of the extracellular matrix of basal keratinocytes, which are major constituents of the epidermis; its free-radical scavenging function and its role in keratinocyte proliferation and migration.[22]
In normal skin, HA is found in relative high concentrations in the basal layer of the epidermis where proliferating keratinocytes are found.[39] CD44 is collocated with HA in the basal layer of epidermis where additionally it has been shown to be preferentially expressed on plasma membrane facing the HA-rich matrix pouches.[22][40] Maintaining the extracellular space and providing an open, as well as hydrated, structure for the passage of nutrients are the main functions of HA in epidermis. Tammi R. and other colleagues [39] found HA content increases at the presence of retinoic acid (vitamin A). The proposed effects of retinoic acid against skin photo-damage and aging may be correlated, at least in part, with an increase of skin HA content, giving rise to increase of tissue hydration. It has been suggested the free-radical scavenging property of HA contributes to protection against solar radiation, supporting the role of CD44 acting as a HA receptor in the epidermis.[22]
Epidermal HA also functions as a manipulator in the process of keratinocyte proliferation, which is essential in normal epidermal function, as well as during reepithelization in tissue repair. In the wound healing process, HA is expressed in the wound margin, in the connective tissue matrix, and collocating with CD44 expression in migrating keratinocytes.[22][41] Kaya et al. found suppression of CD44 expression by an epidermis-specific antisense transgene resulted in animals with defective HA accumulation in the superficial dermis, accompanied by distinct morphologic alterations of basal keratinocytes and defective keratinocyte proliferation in response to mitogen and growth factors. Decrease in skin elasticity, impaired local inflammatory response, and impaired tissue repair were also observed.[22] Their observations are strongly supportive of the important roles HA and CD44 have in skin physiology and tissue repair.[22]
- Fetal wound healing and scarring
Lack of fibrous scarring is the primary feature of fetal wound healing. Even for longer periods, HA content in fetal wounds is still higher than that in adult wounds, which suggests that HA may, at least in part, reduce collagen deposition and therefore lead to reduced scarring.[42] This suggestion is in agreement with the research of West et al., who showed in adult and late gestation fetal wound healing, removal of HA results in fibrotic scarring.[22] Though the exact role of HA in skin scarring is still under investigation, based on all the facts that have been observed, it must be a great contributor to the less fibrous scarring.
Role of hyaluronan in cancer metastasis
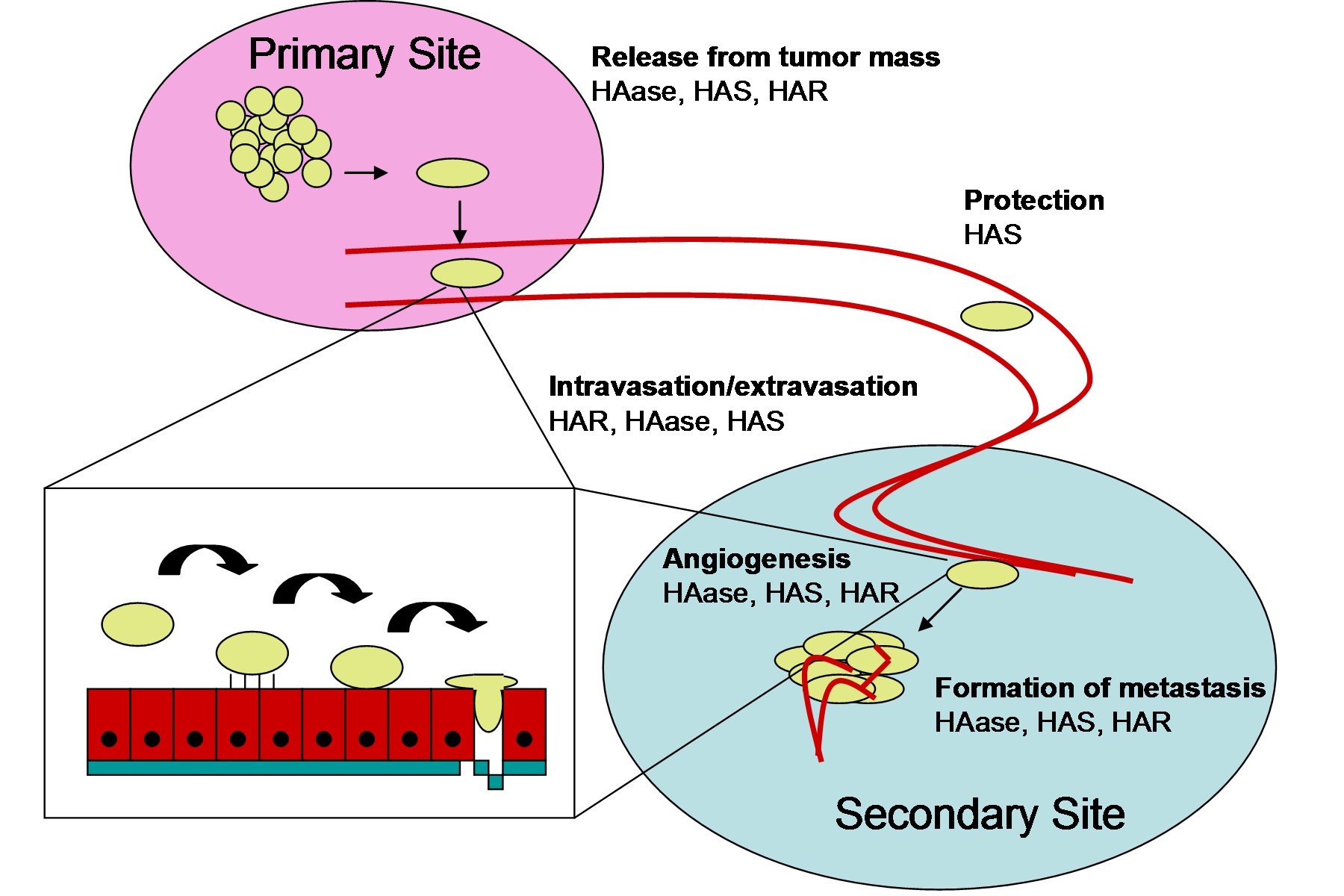
 Figure 1. The process of cancer metastasis in which HA-associated molecules play a role in the steps. Abbreviations: hyaluronic acid (HA), hyaluronic acid synthase (HAS), hyaluronic acid receptor (HAR), hyaluronidase (HAase/HYAL)
Figure 1. The process of cancer metastasis in which HA-associated molecules play a role in the steps. Abbreviations: hyaluronic acid (HA), hyaluronic acid synthase (HAS), hyaluronic acid receptor (HAR), hyaluronidase (HAase/HYAL)
As shown in Figure 1, the various types of molecules that interact with hyaluronan can contribute to many of the stages of cancer metastasis.
Hyaluronan synthases (HAS) play roles in all of the stages of cancer metastasis. By producing anti-adhesive HA, HAS can allow tumor cells to release from the primary tumor mass, and if HA associates with receptors such as CD44, the activation of Rho GTPases can promote epithelial-mesenchymal transition (EMT) of the cancer cells. During the processes of intravasation or extravasation, the interaction of HAS produced HA with receptors such as CD44 or RHAMM promote the cell changes that allow for the cancer cells to infiltrate the vascular or lymphatic systems. While traveling in these systems, HA produced by HAS protects the cancer cell from physical damage. Finally, in the formation of a metastatic lesion, HAS produces HA to allow the cancer cell to interact with native cells at the secondary site and to produce a tumor for itself.[43]
Hyaluronidases (HAase or HYAL) also play many roles in cancer metastasis. By helping to degrade the ECM surrounding the tumor, hyaluronidases help the cancer cell escape from the primary tumor mass and play a major role in intravasation by allowing degradation of the basement membrane of the lymph or blood vessel. Hyaluronidases again play these roles in establishment of a metastatic lesion by helping with extravasation and clearing the ECM of the secondary site.[44] Finally, hyaluronidases play a key role in the process of angiogenesis. HA fragments promote angiogenesis and hyaluronidases produce these fragments.[45] Interestingly, hypoxia also increases production of HA and activity of hyaluronidases.[46]
The hyaluronan receptors, CD44 and RHAMM, are most thoroughly studied in terms of their roles in cancer metastasis. Increased clinical CD44 expression has been positively correlated to metastasis in a number of tumor types.[47] In terms of mechanics, CD44 affects adhesion of cancer cells to each other and to endothelial cells, rearranges the cytoskeleton through the Rho GTPases, and increases the activity of ECM degrading enzymes.[48] Increased RHAMM expression has also been clinically correlated with cancer metastasis. In terms of mechanics, RHAMM promotes cancer cell motility through a number of pathways including focal adhesion kinase (FAK), Map kinase (MAPK), pp60(c-src), and the downstream targets of Rho kinase (ROK).[49] RHAMM can also cooperate with CD44 to promote angiogenesis toward the metastatic lesion.[50]
Medical applications
Hyaluronan is found in many tissues of the body, such as skin, cartilage, and the vitreous humour. Therefore, it is well suited to biomedical applications targeting these tissues. The first hyaluronan biomedical product, Healon, was developed in the 1970s and 1980s by Pharmacia, and is approved for use in eye surgery (i.e., corneal transplantation, cataract surgery, glaucoma surgery, and surgery to repair retinal detachment). Other biomedical companies also produce brands of hyaluronan for opthalmic surgery.[51][52][53]
Native hyaluronan has a relatively short half-life (shown in rabbits)[54] so various manufacturing techniques have been deployed to extend the length of the chain and stabilise the molecule for its use in medical applications. The introduction of protein based cross-links,[55] the introduction of free-radical scavenging molecules such as sorbitol[56] and minimal stabilisation of the HA chains through chemical agents e.g. NASHA stabilisation are all techniques that have been used.[57]
In the late 1970s, intraocular lens implantation was often followed by severe corneal edema, due to endothelial cell damage during the surgery. It was evident that a viscous, clear, physiologic lubricant to prevent such scraping of the endothelial cells was needed.[58][59] Endre Balazs patented a process for purifying hyaluronic acid, a physiologic lubricant (which he called Healon) from rooster combs in the early 1970s. At first, Balazs saw Healon as a noninflammatory vitreous substitute. Claus Dohlman had used Balazs’ Healon in one case in which the anterior chamber flattened after a complicated corneal transplant. Although one might imagine the viscous hyaluronic acid would have caused a rise in IOP, Dohlman reported no such rise in his case[citation needed]. Since that time, Balazs had licensed the synthesis process to Pharmacia, a Swedish drug company. Although Pharmacia saw no market for a vitreous substitute, when their scientists figured out a way to increase the viscosity of hyaluronic acid, they felt it might work as an injectable agent in the treatment of both human and equine arthritis. The equine arthritis market proved to be small and the treatment of human osteoarthritis produced only marginal improvement[citation needed], so Pharmacia decided to abandon Healon. At this time, David Miller realized that Healon was the lubricant needed by the eye surgeon[citation needed].
Balazs arranged to have Pharmacia send 20 sterile vials to Dr. David Miller for rabbit experiments. By 1976, Miller and colleagues published a study showing Healon worked well in protecting the rabbit corneal endothelium during IOL implantation[citation needed]. With a new possible use for Healon, Miller met with Pharmacia and performed a lens extraction and IOL implantation using Healon in a rabbit eye. The demonstration ignited a new enthusiasm for eye surgery with Healon. A small human pilot study at Boston’s Beth Israel Hospital by Miller confirmed Healon’s beneficial effects[citation needed].
In a large, well-controlled clinical trial, Dr. Robert Stegmann, of Pretoria, South Africa was able to quantify the advantages of Healon in IOL implantation by showing significantly higher postoperative corneal endothelial counts in the Healon eyes as opposed to the controls[citation needed].
The U.S. Food and Drug Administration quickly approved Healon as a surgical device in 1980, and Healon was successfully launched. By the year 2009, an estimated quarter of a billion patients had benefited from the useful properties of Healon in eye surgery[citation needed].
In 1992, Miller and Stegmann received the Innovators Award by the American Society of Cataract and Refractive Surgery for developing the use of Healon in repairing injured eyes[citation needed].
Hyaluronan is also used to treat osteoarthritis of the knee.[60] Such treatments, called viscosupplementation, are administered as a course of injections into the knee joint, and are believed to supplement the viscosity of the joint fluid, thereby lubricating the joint, cushioning the joint, and producing an analgesic effect. It has also been suggested that hyaluronan has positive biochemical effects on cartilage cells. However, some placebo-controlled studies have cast doubt on the efficacy of hyaluronan injections, and hyaluronan is recommended primarily as a last alternative before surgery[61] Oral use of hyaluronan has been lately suggested, although its effectiveness needs to be demonstrated. At present, there are some preliminary clinical studies that suggest oral administration of hyaluronan has a positive effect on osteoarthritis, but it remains to be seen if there is any real benefit from the treatment.
Dry, scaly skin (xerosis) such as that caused by atopic dermatitis (eczema) may be treated with a prescription skin lotion containing sodium hyaluronate as its active ingredient.[62]
Due to its high biocompatibility and its common presence in the extracellular matrix of tissues, hyaluronan is gaining popularity as a biomaterial scaffold in tissue engineering research.[63] In particular, a number of research groups have found hyaluronan's properties for tissue engineering and regenerative medicine are significantly improved with crosslinking, producing a hydrogel. This added feature allows a researcher to form a desired shape, as well as to deliver therapeutic molecules, into a host.[64] Hyaluronan can be crosslinked by attaching thiols (trade names: Extracel, HyStem),[64] methacrylates,[65] and tyramines (trade name: Corgel).[66] Hyaluronan can also be crosslinked directly with formaldehyde (trade name: Hylan-A) or with divinylsulfone (trade name: Hylan-B).[67]
In some cancers, hyaluronan levels correlate well with malignancy and poor prognosis. Hyaluronan is, thus, often used as a tumor marker for prostate and breast cancer. It may also be used to monitor the progression of the disease[citation needed].
Hyaluronan may also be used postoperatively to induce tissue healing, notably after cataract surgery.[68] Current models of wound healing propose the larger polymers of hyaluronic acid appear in the early stages of healing to physically make room for white blood cells, which mediate the immune response.
Hyaluronan has also been used in the synthesis of biological scaffolds for wound-healing applications. These scaffolds typically have proteins such as fibronectin attached to the hyaluronan to facilitate cell migration into the wound. This is particularly important for individuals with diabetes suffering from chronic wounds.[69]
In 2007, the EMA extended its approval of Hylan GF-20 as a treatment for ankle and shoulder osteoarthritis pain.[70]
Hyaluronan is also used in anti-adhesive products such as Hyalobarrier, widely used in pelvic and abdominal surgery to prevent postoperative adhesions.
In May, 2011, Dr Endre Balazs was awarded the Helen Keller Award for Vision Research for his work in championing the development of hyaluronan and Healon. The award was presented by the Helen Keller Foundation for Research and education.[citation needed]
Cosmetic applications
Hyaluronan is a common ingredient in skin-care products.
In 2003, the FDA approved hyaluronan injections for filling soft tissue defects such as facial wrinkles. Restylane is a common trade name for the product. Hyaluronan injections temporarily smooth wrinkles by adding volume under the skin, with effects typically lasting for six months.
Juvéderm is a bacterial hyaluronic acid injectable filler, similar to Restylane, but differing slightly in terms of effect and longevity. It is used for lip augmentation, reduction of folds and wrinkles, and removal of scars. The effects of Juvéderm treatments are also temporary, and costs are similar to those of Restylane.[71]
The presence of hyaluronic acid in epithelial tissue has been shown to promote keratinocyte proliferation and increase the presence of retinoic acid, effecting skin hydration. Hyaluronic acid's interaction with CD44 drives collagen synthesis and normal skin function. Present in the extracellular matrix of basal keratinocytes, hyaluronic acid is critical to the structural integrity of the dermal collagen matrix. These benefits make hyaluronic acid a very effective topical humectant; however, results may only be sustained as part of an ongoing treatment program.[72]
Equine applications
Hyaluronan is used in treatment of articular disorders in horses, in particular those in competition or heavy work. It is indicated for carpal and fetlock joint dysfunctions, but not when joint sepsis or fracture are suspected. It is especially used for synovitis associated with equine osteoarthritis. It can be injected directly into an affected joint, or intravenously for less localized disorders. It may cause mild heating of the joint if directly injected, but this does not affect the clinical outcome. Intra-articularly administered medicine is fully metabolized in less than a week.[73]
Note that, according to Canadian regulation, hyaluronan in HY-50 preparation should not be administered to animals to be slaughtered for horse meat.[74] In Europe, however, the same preparation is not considered to have any such effect, and edibility of the horse meat is not affected.[75]
Etymology
Hyaluronic acid is derived from hyalos (Greek for vitreous) and uronic acid because it was first isolated from the vitreous humour and possesses a high uronic acid content.
The term hyaluronate refers to the conjugate base of hyaluronic acid. Because the molecule typically exists in vivo in its polyanionic form, it is most commonly referred to as hyaluronan.
See also
References
- ^ Hyaluronate Sodium in the ChemIDplus database, consulté le 12 février 2009
- ^ Frasher, J.R.E et al'; Laurent, T. C.; Laurent, U. B. G. (1997). "Hyaluronan: its nature, distribution, functions and turnover" (PDF). Journal of Internal Medicine 242: 27–33. doi:10.1046/j.1365-2796.1997.00170.x. PMID 9260563. http://www3.interscience.wiley.com.iiiprxy.library.miami.edu/cgi-bin/fulltext/119157843/PDFSTART. Retrieved 2009-06-05.
- ^ Stern R (August 2004). "Hyaluronan catabolism: a new metabolic pathway". Eur J Cell Biol 83 (7): 317–25. doi:10.1078/0171-9335-00392. PMID 15503855.
- ^ Sugahara, K.; N.B. Schwartz and A. Dorfman (1979). "Biosynthesis of hyaluronic acid by Streptococcus". Journal of Biological Chemistry 254 (14): 6252–6261. PMID 376529. http://www.jbc.org/content/254/14/6252.full.pdf.
- ^ Wessels, M.R.; A.E. Moses, J.B. Goldberg and T.J. DiCesare (1991). "Hyaluronic acid capsule is a virulence factor for mucoid group A streptococci". PNAS 88 (19): 8317–8321. doi:10.1073/pnas.88.19.8317. PMC 52499. PMID 1656437. http://www.pnas.org/content/88/19/8317.full.pdf.
- ^ Schrager, H.M.; J.G. Rheinwald and M.R. Wessels (1996). "Hyaluronic acid capsule and the role of streptococcal entry into keratinocytes in invasive skin infection". Journal of Clinical Investigation 98 (9): 1954–1958. doi:10.1172/JCI118998. PMC 507637. PMID 8903312. http://www.jci.org/articles/view/118998/pdf.
- ^ Meyer K and Palmer JW (1934) “The polysaccharide of the vitreous humor,”. J Biol Chem, 107: 629-634.
- ^ Toole, B.P. (August 2000). "Hyaluronan is not just a goo! (.pdf)". Journal of Clinical Investigation 106 (3): 335–336. doi:10.1172/JCI10706. PMC 314333. PMID 10930435. http://www.jci.org/articles/view/10706/pdf.
- ^ Hyaluronan as a Versatile Biomaterial for Surface Treatment of Medical Devices Djoerd Hoekstra President and CEO, Biocoat, Incorporated
- ^ Meyer K and Palmer JW (1934) “The polysaccharide of the vitreous humor,”. J Biol Chem, 107: 629-634.
- ^ Holmes et al. (1988) Hyaluronic acid in human articular cartilage. Age-related changes in content and size. Biochem J 250:435-441.
- ^ Averbeck M et al. (2007) Differential regulation of hyaluronan metabolism in the epidermal and dermal compartments of human skin by UVB irradiation. J Invest Dermatol 127:687-697.
- ^ Glycosaminoglycans of Brain during Development. R. U. Margolis, R. K. Margolis, L. B. Chang, and C. Preti. BIOCHEMISTRY VOL. 14, NO. I , 1975. Pg. 85. Retrieved 1/17/08.
- ^ Meyer K, Hobby GL, Chaffee E, Dawson MH (January 1940). "The hydrolysis of hyaluronic acid by bacterial enzymes". J Exp Med 71 (2): 137–46. doi:10.1084/jem.71.2.137. PMC 2135078. PMID 19870951. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2135078.
- ^ Saari H et al. (1993) Differential effects of reactive oxygen species on native synovial fluid and purified human umbilical cord hyaluronate. Inflammation 17:403-415.
- ^ Schulz,T.; Schumacher,U.; Prehm,P. Hyaluronan export by the ABC transporter MRP5 and its modulation by intracellular cGMP. J.Biol.Chem.282,20999-21004
- ^ Kakizaki, I.; Kojima, K.; Takagaki, K.; Endo, M.; Kannagi, R.; Ito, M.; Maruo, Y.; Sato, H. et al. (2004). "A novel mechanism for the inhibition of hyaluronan biosynthesis by 4-methylumbelliferone". J. Biol. Chem. 279 (32): 33281–33289. doi:10.1074/jbc.M405918200. PMID 15190064.
- ^ Yoshihara, S; Kon, A; Kudo, D; Nakazawa, H; Kakizaki, I; Sasaki, M; Endo, M; Takagaki, K (2005). "A hyaluronan synthase suppressor, 4-methylumbelliferone, inhibits liver metastasis of melanoma cells.". FEBS letters 579 (12): 2722–6. doi:10.1016/j.febslet.2005.03.079. PMID 15862315.
- ^ Novozymes Biopharma | Produced without the use of animal-derived materials or solvents
- ^ a b c d Wayne D. Comper, Extracellular Matrix Volume 2 Molecular Components and Interactions, 1996, Harwood Academic Publishers
- ^ Aruffo A., et al. Cell, 1990, 61: 1303-1313
- ^ a b c d e f g h i j k l m n o p q r s t u v w x W. Y. John Chen and Giovanni Abatangelo, Wound Repair and Regeneration, 1999, 7: 79-89
- ^ Kaya G. et al. Genes & Development, 1997, 15: 996-1007
- ^ Laurent U. B. G. and Reed R. K. Advanced Drug Delivery Reviews, 1991, 7: 237-256
- ^ Fraser J. R. E. et al. Biochemical Journal, 1988, 356: 153-158
- ^ Campbell P. et al. Hepatology, 1990, 11: 199-204
- ^ a b Kennndy J. F., et al., HA, Volume 2 Biomedical, Medical and Clinical Aspects, 2002, Woodhead Publishing Limited.
- ^ Wisniewski H. G., et al., The Journal of Immunology, 1996, 156: 1609-1615
- ^ Kobayashi H. and Terao T. American Journal of Physiology, 1997, 276: C1151-1159
- ^ Mohamadzadeh M., et al., The Journal of Clinical Investigation, 1998, 101: 97-108
- ^ Hall C. L., et al., The Journal of cell biology, 1992, 117: 1343-1350
- ^ Wang C. et al., Clinical Cancer Research, 1998, 4: 567-576
- ^ Hall C. L., et al., Oncogene, 1996. 13: 2213-2214
- ^ Morriss-Kay G. M., et al., Journal of Embryology and Experimental Morphology, 1986, 98: 59-70
- ^ Ellis I. R., et al., Experimental Cell Research, 1996, 228: 326-342
- ^ Tammi R., et al., Journal of Investigative Dermatology, 1988, 90: 412-414
- ^ Foschi D., et al., International Journal on Tissue Reaction, 1990, 12: 333-339
- ^ Wisniewski H. G. and Vilcek J. Cytokine & Growth Factor Reviews, 1997, 8: 143-156
- ^ a b Tammi R, et al., Journal of Investigative Dermatology, 1989, 92: 326-332
- ^ Tuhkanen A-L, et al., Journal of Histochemistry and Cytochemistry, 1998, 46: 241-248
- ^ Kaya G. et al., Genes & Development, 1997, 15: 996-1007
- ^ Longaker M. T., et al., Annals of Surgery, 1991, 213: 292-296
- ^ Baradwaj AG, et al. Spontaneous metastasis of prostate cancer is promoted by excess hyaluornan synthesis and processing. Am J Path. 2009;174:1027-1036
- ^ Bharadwaj AG, et al. Inducible hyaluornan production reveals differential effects of prostate tumor cell growth and tumor angiogenesis. J Cell Biol. 2007;282:20561-20572
- ^ Gao F, et al. Hyaluronan oligosaccharides are potential stimulators to angiogenesis via RHAMM mediated signal pathway in wound healing. Clinical and Investigative Medicine. 2008;31:E106-116
- ^ Gao, et al. Hypoxia-induced alterations in hyaluronan and hyaluronidase. Adv Exp Med Biol. 2005;566:249-256
- ^ Ouhtit A, et al. In vivo evidence for the role of CD44s in promoting breast cancer metastasis to the liver. Am J Path. 2007;171:2033-2039
- ^ Naor, et al. Involvement of CD44, a molecule with a thousand faces, in cancer dissemination. Sem Cancer Biol. 2008;18:260-267
- ^ Hall CL, et al. Hyaluronan: RHAMM mediated cell locomotion and signaling in tumorigenesis. J Neuro-oncology. 1995;103:203-207
- ^ Savani, et al. Differential involvement of the hyaluornan (HA) receptors CD44 and receptor for HA-mediated motility in endothelial cell function and angiogenesis. J Biol Chem. 2001;276:36770-36778
- ^ Error 404: Page Not Found | Alcon
- ^ Bausch & Lomb: Amvisc and Amvisc Plus - Brief Statement
- ^ Medical Grade Hyaluronan | Lifecore Biomedical
- ^ >Brown TJ; Laurent UBJ Fraser JRE (1991). "Turnover of hyaluronan in synovial joints: elimination of labelled hyaluronan from the knee joint of the rabbit". Experimental Physiology 76 (1): 125–134. PMID 2015069.</
- ^ Frampton JE (2010). "Hylan GF-20 Single injection formulation". Drugs Aging 27 (1): 77–85. doi:10.2165/11203900-000000000-00000. PMID 20030435.</
- ^ Anteis | Change starts here
- ^ Medicijnvrije behandeling van artrose en artritis
- ^ 1. Miller D, O’Connor P,William J: Use of Na-Hyaluronate during intraocular lens implantation in rabbits. Ophthal Surg. 8:58-61, 1977
- ^ 7. Miller D, Stegmann R: Healon: A Comprehensive Guide to it’s Use in Ophthalmic Surgery. J Wiley, NY, 1983
- ^ Puhl W; Scharf P (July 1997). "Intra-articular hyaluronan treatment for osteoarthritis". Ann Rheum Dis 56 (7): 637–40. doi:10.1136/ard.56.7.441. PMC 1752402. PMID 9486013. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1752402.
- ^ Comparison of two hyaluronan drugs and placebo in patients with knee osteoarthritis. A controlled, randomized, double-blind, parallel-design multicentre study - Karlsson et al. 41 (11): 1240 - Rheumatology
- ^ http://www.drugs.com/cdi/hylira-gel.html.
- ^ Bio-skin FAQ
- ^ a b Shu XZ, Liu Y, Palumbo FS, Luo Y, Prestwich GD: In situ crosslinkable hyaluronan hydrogels for tissue engineering. Biomaterials, 25:1339-1348, 2004.
- ^ Gerecht S, Burdick JA, Ferreira LS, Townsend SA, Langer R, and Vunjak-Novakovic G: Hyaluronic acid hydrogel for controlled self-renewal and differentiation of human embryonic stem cells. Proc Natl Acad Sci USA, 104:11298-11303, 2007.
- ^ Dar A, Calabro A: Synthesis and characterization of tyramine-based hyaluronan hydrogels. J Mater Sci: Mater Med, 20:33-44, 2009.
- ^ Wnek GE, Bowlin GL (editors): Encyclopedia of Biomaterials and Biomedical Engineering. Informa Healthcare, 2008.
- ^ De Andrés Santos MI, Velasco-Martín A, Hernández-Velasco E, Martín-Gil J, Martín-Gil FJ (1994). "Thermal behaviour of aqueous solutions of sodium hyaluronate from different commercial sources". Thermochim Acta 242: 153–160. doi:10.1016/0040-6031(94)85017-8.
- ^ Shu XZ, Ghosh K, Liu Y, Palumbo FS, Luo Y, Clark RAF, Prestwich GD: Attachment and spreading of fibroblast on an RGD peptide-modified injectable hyaluronan hydrogel. J Biomed Materials Res, 68:365-75, 2004.
- ^ "Hylan G-F 20 (Synvisc) approved by EMEA for pain due to ankle and shoulder OA". National Health Service. http://www.library.nhs.uk/musculoskeletal/ViewResource.aspx?resID=182567. Retrieved 2007-07-09.
- ^ Juvederm[dead link]
- ^ Hyaluronic Acid Essential Actives, KAVI.
- ^ Genitrix HY-50 Vet datasheet
- ^ HY-50 for veterinary use
- ^ Genitrix HY-50 Vet brochure
External links
Unsulfated, extracellular HyaluronanSulfated, extracellular Sulfated, intracellular Preparations for treatment of wounds and ulcers (D03) Cicatrizants epichlorohydrin: Cadexomer iodine • Dextranomer • Crilanomer
B5: Dexpanthenol • Calcium pantothenate
nitrate: Glyceryl trinitrate • Isosorbide dinitrate
other: Becaplermin • Hyaluronic acid • EnoxoloneProteolytic enzymes Trypsin • ClostridiopeptidaseDecongestants and other nasal preparations (R01) Topical Sympathomimetics, plainCyclopentamine • Ephedrine • Phenylephrine • Oxymetazoline • Tetryzoline • Xylometazoline • Naphazoline • Tramazoline • Metizoline • Tuaminoheptane • Fenoxazoline • Tymazoline • EpinephrineSpaglumic acid
histamine antagonists (Levocabastine, Antazoline, Thonzylamine)
mast cell stabilizer (some are also antihistamines) (Cromoglicic acid, Nedocromil, Azelastine, Olopatadine, Lodoxamide)Other nasal preparationsCafaminol • Calcium hexamine thiocyanate • Retinol • Ipratropium bromide • Ritiometan • Mupirocin • Hexamidine • Framycetin • Hyaluronic acid • Eucalyptus oilSystemic use:
SympathomimeticsCategories:- Glycosaminoglycans
Wikimedia Foundation. 2010.