- Childbirth
-
"Parturition" redirects here. For the Voyager episode, see Parturition (Star Trek: Voyager).
Childbirth (also called labor, birth, partus or parturition) is the culmination of a human pregnancy or gestation period with the birth of one or more newborn infants from a woman's uterus. The process of normal human childbirth is categorized in three stages of labour: the shortening and dilation of the cervix, descent and birth of the infant, and birth of the placenta.[1] In many cases, with increasing frequency, childbirth is achieved through caesarean section, the removal of the neonate through a surgical incision in the abdomen, rather than through vaginal birth.[2] In the U.S. and Canada it represents nearly 1 in 3 (31.8%) and 1 in 4 (22.5%) of all childbirths, respectively.[3][4]
Contents
Signs and symptoms
 Natural childbirth at home.
Natural childbirth at home.
Labor is accompanied by intense and prolonged pain. Pain levels reported by laboring women vary widely. Pain levels appear to be influenced by fear and anxiety levels. Some other factors may include experience with prior childbirth, age, ethnicity, preparation, physical environment and immobility.
Psychological
Childbirth can be an intense event and strong emotions, both positive and negative, can be brought to the surface.
Between 70% and 80% of mothers in the United States report some feelings of sadness or "baby blues" after childbirth.[citation needed] Postpartum depression may develop in some women; about 10% of mothers in the United States are diagnosed with this condition. Abnormal and persistent fear of childbirth is known as tokophobia.
Preventive group therapy has proven effective as a prophylactic treatment for postpartum depression.[5]
Childbirth is stressful for the infant. In addition to the normal stress of leaving the protected uterine environment, additional stresses associated with breech birth, such as asphyxiation, may affect the infant's brain.[citation needed]
Normal human birth
Mechanism of vaginal birth
Because humans are bipedal with an erect stance and have, in relation to the size of the pelvis, the biggest head of any mammalian species, human fetuses and human female pelvises are adapted to make birth possible.
The erect posture causes the weight of the abdominal contents to thrust on the pelvic floor, a complex structure which must not only support this weight but allow three channels to pass through it: the urethra, the vagina and the rectum. The relatively large head and shoulders require a specific sequence of maneuvers to occur for the bony head and shoulders to pass through the bony ring of the pelvis. A failure of these maneuvers results in a longer and more painful labor and can even arrest labor entirely. All changes in the soft tissues of the cervix and the birth canal depend on the successful completion of these six phases:
- Engagement of the fetal head in the transverse position. The baby's head is facing across the pelvis at one or other of the mother's hips.
- Descent and flexion of the fetal head.
- Internal rotation. The fetal head rotates 90 degrees to the occipito-anterior position so that the baby's face is towards the mother's rectum.
- Delivery by extension. The fetal head passes out of the birth canal. Its head is tilted forwards so that the crown of its head leads the way through the vagina.
- Restitution. The fetal head turns through 45 degrees to restore its normal relationship with the shoulders, which are still at an angle.
- External rotation. The shoulders repeat the corkscrew movements of the head, which can be seen in the final movements of the fetal head.
The fetal head may temporarily change shape substantially (becoming more elongated) as it moves through the birth canal. This change in the shape of the fetal head is called molding and is much more prominent in women having their first vaginal delivery.[6]
Latent phase
The latent phase of labor, also called prodromal labor, may last many days and the contractions are an intensification of the Braxton Hicks contractions that may start around 26 weeks gestation. Cervical effacement occurs during the closing weeks of pregnancy and is usually complete or near complete, by the end of the latent phase. Cervical effacement or cervical dilation is the thinning and stretching of the cervix. The degree of cervical effacement may be felt during a vaginal examination. A 'long' cervix implies that not much has been taken into the lower segment, and vice versa for a 'short' cervix. Latent phase ends with the onset of active first stage; when the cervix is about 3 cm dilated.
First stage: dilation
There are several factors that midwives and clinicians use to assess the laboring mother's progress, and these are defined by the Bishop Score. The Bishop score is also used as a means to predict whether the mother is likely to spontaneously progress into second stage (delivery).
The first stage of labor starts classically when the effaced (thinned) cervix is 3 cm dilated. There is a variation in this point as some women may have active contractions prior to reaching this point, or they may reach this point without regular contractions. The onset of actual labor is defined when the cervix begins to progressively dilate. Rupture of the membranes, or a blood stained 'show' may or may not occur at or around this stage.
Uterine muscles form opposing spirals from the top of the upper segment of the uterus to its junction with the lower segment. During effacement, the cervix becomes incorporated into the lower segment of the uterus. During a contraction, these muscles contract causing shortening of the upper segment and drawing upwards of the lower segment, in a gradual expulsive motion. This draws the cervix up over the baby's head. Full dilation is reached when the cervix has widened enough to allow passage of the baby's head, around 10 cm dilation for a term baby.
The duration of labour varies widely, but active phase averages some 8 hours for women giving birth to their first child ("primiparae") and 4 hours for women who have already given birth ("multiparae"). Active phase arrest is defined as in a primigravid woman as the failure of the cervix to dilate at a rate of 1.2 cm/hr over a period of at least two hours. This definition is based on Friedman's Curve, which plots the typical rate of cervical dilation and fetal descent during active labor.[7] Some practitioners may diagnose "Failure to Progress", and consequently, perform a Cesarean.[8]
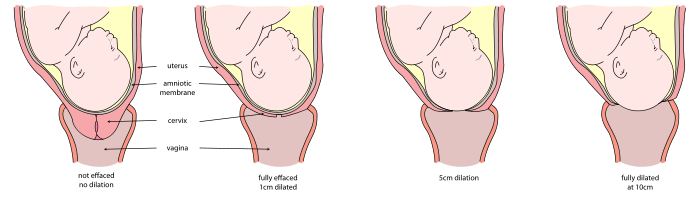 Sequence of cervix dilation during labor
Sequence of cervix dilation during laborSecond stage: fetal expulsion
This stage begins when the cervix is fully dilated, and ends when the baby is finally born. As pressure on the cervix increases, the Ferguson reflex increases uterine contractions so that the second stage can go ahead. At the beginning of the normal second stage, the head is fully engaged in the pelvis; the widest diameter of the head has successfully passed through the pelvic brim. Ideally it has successfully also passed below the interspinous diameter. This is the narrowest part of the pelvis. If these have been accomplished, what remains is for the fetal head to pass below the pubic arch and out through the introitus. This is assisted by the additional maternal efforts of "bearing down" or pushing. The fetal head is seen to 'crown' as the labia part. At this point, the woman may feel a burning or stinging sensation.
Birth of the fetal head signals the successful completion of the fourth mechanism of labor (delivery by extension), and is followed by the fifth and sixth mechanisms (restitution and external rotation).
 A newborn baby with umbilical cord ready to be clamped
A newborn baby with umbilical cord ready to be clampedThe second stage of labor will vary to some extent, depending on how successfully the preceding tasks have been accomplished.
Third stage: umbilical cord closure and placental expulsion
Further information: Umbilical cord and Placental expulsion Breastfeeding during and after the third stage, the placenta is visible in the bowl to the right.
Breastfeeding during and after the third stage, the placenta is visible in the bowl to the right.The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor.
The umbilical cord is routinely clamped and cut in this stage, but it would normally close naturally even if not clamped. A 2008 Cochrane Review looked into the timing of clamping the umbilical cord. It found that the time of clamping made no difference to the mother, but did have effects for the baby. If the cord is clamped after 2–3 minutes, the infant receives increased amounts of haemoglobin in their first months of life, but may have an increased risk of needing phototherapy to treat jaundice. Sometimes a newborn’s liver is slow to break down all of the red cells they had in the womb, particularly if they are left with more fetal blood from delayed cord clamping and phototherapy helps to speed the breakdown.[9]
Placental expulsion begins as a physiological separation from the wall of the uterus. The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor. The placenta is usually expelled within 15–30 minutes of the baby being born. Placental expulsion can be managed actively, for example by giving oxytocin via intramuscular injection followed by cord traction to assist in delivering the placenta. Alternatively, it can be managed expectantly, allowing the placenta to be expelled without medical assistance. A Cochrane database study[10] suggests that blood loss and the risk of postpartum bleeding will be reduced in women offered active management of the third stage of labour.
When the amniotic sac has not ruptured during labour or pushing, the infant can be born with the membranes intact. This is referred to as "being born in the caul." The caul is harmless and its membranes are easily broken and wiped away. With the advent of modern interventive obstetrics, artificial rupture of the membranes has become common, so babies are rarely born in the caul.
Fourth stage
The "fourth stage of labor" is a term used in two different senses:
- It can refer to the immediate puerperium,[11] or the hours immediately after delivery of the placenta.[12]
- It can be used in a more metaphorical sense to describe the weeks following delivery.[13]
Afterwards
Further information: PostnatalMany cultures feature initiation rites for newborns, such as naming ceremonies, baptism, and others.
Mothers are often allowed a period where they are relieved of their normal duties to recover from childbirth. The length of this period varies. In many countries, taking time off from work to care for a newborn is called "maternity leave" or "parental leave" and can vary from a few days to several months.
Station
Refers to the relationship of the fetal presenting part to the level of the ischial spines. When the presenting part is at the ichial spines the station is 0 (synonymous with engagement). If the presenting fetal part is above the spines, the distance is measured and described as minus stations, which range from -1 to -4 cm. If the presenting part is below the ischial spines, the distance is stated as plus stations ( +1 to +4 cm). At +3 and +4 the presenting part is at the perineum and can be seen.[14]
Management
Eating or drinking during labor has no harmful effects on outcomes[15], although doctors do not want women in labor to eat food in case they end up needing a cesarean section.
Pain control
- Non pharmaceutical
Some women prefer to avoid analgesic medication during childbirth. They can still try to alleviate labor pain using psychological preparation, education, massage, acupuncture, TENS unit use, hypnosis, or water therapy in a tub or shower. Some women like to have someone to support them during labor and birth, such as the father of the baby, a family member, a close friend, a partner, or a doula. Some women deliver in a squatting or crawling position in order to more effectively push during the second stage and so that gravity can aid the descent of the baby through the birth canal.
The human body also has a chemical response to pain, by releasing endorphins. Endorphins are present before, during, and immediately after childbirth.[16] Some homebirth advocates believe that this hormone can induce feelings of pleasure and euphoria during childbirth,[17] reducing the risk of maternal depression some weeks later.[16]
Water birth is an option chosen by some women for pain relief during labor and childbirth, and some studies have shown waterbirth in an uncomplicated pregnancy to reduce the need for analgesia, without evidence of increased risk to mother or newborn.[18] Hot water tubs are available in many hospitals and birthing centres.
Meditation and mind medicine techniques are also used for pain control during labour and delivery. These techniques are used in conjunction with progressive muscle relaxation and many other forms of relaxation for the mind and body to aid in pain control for women during childbirth. One such technique is the use of hypnosis in childbirth. There are a number of organizations that teach women and their partners to use a variety of techniques to assist with labor comfort, without the use of pharmaceuticals.
A new mode of analgesia is sterile water injection placed just underneath the skin in the most painful spots during labor. A control trial in Iran of 0.5mL injections was conducted with normal saline which revealed a statistical superiority with water over saline.[19]
- Pharmaceutical
Different measures for pain control have varying degrees of success and side effects to the woman and her baby. In some countries of Europe, doctors commonly prescribe inhaled nitrous oxide gas for pain control, especially as 50% nitrous oxide, 50% oxygen, known as Entonox; in the UK, midwives may use this gas without a doctor's prescription. Pethidine (with or without promethazine) may be used early in labour, as well as other opioids such as fentanyl, but if given too close to birth there is a risk of respiratory depression in the infant.
Popular medical pain control in hospitals include the regional anesthetics epidural blocks, and spinal anaesthesia. Epidural analgesia is a generally safe and effective method of relieving pain in labour, but is associated with longer labour, more operative intervention (particularly instrument delivery), and increases in cost.[20] Generally, pain and cortisol increased throughout labor in women without EDA. Pain and stress hormones rise throughout labor for women without epidurals, while pain, fear, and stress hormones decrease upon administration of epidural analgesia, but may rise again later.[21] Medicine administered via epidural can cross the placenta and enter the bloodstream of the fetus.[22] Epidural analgesia has no statistically significant impact on the risk of caesarean section, and does not appear to have an immediate effect on neonatal status as determined by Apgar scores.[23]
Augmentation
Augmentation is a procedure which attempts to speed up the process of labour. Oxytocin has been used to increase the rate of vaginal delivery in those with a slow progress of labor.[24]
Instrumental delivery
Obstetric forceps or ventouse may be used to facilitate childbirth.
- The woman will have her legs supported in stirrups.
- If an anaesthetic is not already in place it will be given.
- Episiotomy might be needed.
- A trial forceps might be performed, which is abandoned in favor of a caesarean section if delivery is not optimal.
Multiple births
Twins can be delivered vaginally. In some cases twin delivery is done in a larger delivery room or in the theatre, just in case complications occur e.g.
- Both twins born vaginally - this can occur both presented head first or where one comes head first and the other is breech and/or helped by a forceps/ventouse delivery
- One twin born vaginally and the other by caesarean section.
- If the twins are joined at any part of the body - called conjoined twins, delivery is mostly by caesarean section.
Support
See also: Men's role in childbirth Baby on warming tray attended to by her father.
Baby on warming tray attended to by her father.There is increasing evidence to show that the participation of the woman's partner in the birth leads to better birth and also post-birth outcomes, providing the partner does not exhibit excessive anxiety.[25] Research also shows that when a laboring woman was supported by a female helper such as a family member or doula during labor, she had less need for chemical pain relief, the likelihood of caesarean section was reduced, use of forceps and other instrumental deliveries were reduced, there was a reduction in the length of labor, and the baby had a higher Apgar score (Dellman 2004, Vernon 2006). However, little research has been conducted to date about the conflicts between partners, professionals, and the mother.
Collecting stem cells
It is possible to collect two types of stem cells during childbirth: amniotic stem cells or umbilical cord blood stem cells. To collect amniotic stem cells, it is necessary to do amniocentesis before or during the birth. Amniotic stem cells are multipotent and very active, useful for both autologous or donor use. There are private banks in US; the first is Biocell Center in Boston.[26][27][28]
Umbilical cord blood stem cells are also active, but less multipotent than amniotic stem cells. There are a lot of banks of cord blood, both private and public and for autologous or eterologous use.
Complications
See also: Birth trauma (disambiguation) Disability-adjusted life year for maternal conditions per 100,000 inhabitants in 2002.[29]no dataless than 100100-400400-800800-12001200-16001600-20002000-24002400-28002800-32003200-36003600-4000more than 4000
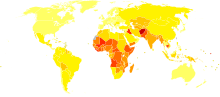
Disability-adjusted life year for maternal conditions per 100,000 inhabitants in 2002.[29]no dataless than 100100-400400-800800-12001200-16001600-20002000-24002400-28002800-32003200-36003600-4000more than 4000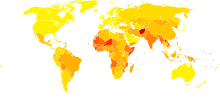 Disability-adjusted life year for perinatal conditions per 100,000 inhabitants in 2002.[29]no dataless than 100100-400400-800800-12001200-16001600-20002000-24002400-28002800-32003200-36003600-4000more than 4000
Disability-adjusted life year for perinatal conditions per 100,000 inhabitants in 2002.[29]no dataless than 100100-400400-800800-12001200-16001600-20002000-24002400-28002800-32003200-36003600-4000more than 4000Childbirth is an inherently dangerous and risky activity, subject to many complications. The "natural" mortality rate of childbirth—where nothing is done to avert maternal death—has been estimated as being 1500 deaths per 100,000 births.[30] (See main article: neonatal death, maternal death). Modern medicine has greatly alleviated the risk of childbirth. In modern Western countries, such as the United States or Sweden, the current maternal mortality rate is around 10 deaths per 100,000 births.[31]
Birthing complications may be maternal or fetal, and long term or short term.
Labor complications
The second stage of labor may be delayed or lengthy due to:
- malpresentation (breech birth (i.e. buttocks or feet first), face, brow, or other)
- failure of descent of the fetal head through the pelvic brim or the interspinous diameter
- poor uterine contraction strength
- active phase arrest
- cephalo-pelvic disproportion (CPD)
- shoulder dystocia
Secondary changes may be observed: swelling of the tissues, maternal exhaustion, fetal heart rate abnormalities. Left untreated, severe complications include death of mother and/or baby, and genitovaginal fistula.
Dystocia (obstructed labour)
Dystocia is an abnormal or difficult childbirth or labour. Approximately one fifth of human labours have dystocia. Dystocia may arise due to incoordinate uterine activity, abnormal fetal lie or presentation, absolute or relative cephalopelvic disproportion, or (rarely) a massive fetal tumor such as a sacrococcygeal teratoma. Oxytocin is commonly used to treat incoordinate uterine activity, but pregnancies complicated by dystocia often end with assisted deliveries, including forceps, ventouse or, commonly, caesarean section. Recognized complications of dystocia include fetal death, respiratory depression, Hypoxic Ischaemic Encephalopathy (HIE), and brachial nerve damage. A prolonged interval between pregnancies, primigravid birth, and multiple birth have also been associated with increased risk for labour dystocia.[32]
Shoulder dystocia is a dystocia in which the anterior shoulder of the infant cannot pass below the pubic symphysis or requires significant manipulation to pass below it. It can also be described as delivery requiring additional manoeuvres after gentle downward traction on the head has failed to deliver the shoulders.
A prolonged second stage of labour is another type of dystocia whereby the fetus has not been delivered within three hours in a nulliparous woman, or two hours in multiparous woman, after her cervix has become fully dilated.he
Synonyms for dystocia include difficult labour, abnormal labour, difficult childbirth, abnormal childbirth, and dysfunctional labour.
Maternal complications
Vaginal birth injury with visible tears or episiotomies are common. Internal tissue tearing as well as nerve damage to the pelvic structures lead in a proportion of women to problems with prolapse, incontinence of stool or urine and sexual dysfunction. Fifteen percent of women become incontinent, to some degree, of stool or urine after normal delivery, this number rising considerably after these women reach menopause. Vaginal birth injury is a necessary, but not sufficient, cause of all non hysterectomy related prolapse in later life. Risk factors for significant vaginal birth injury include:
- A baby weighing more than 9 pounds.
- The use of forceps or vacuum for delivery. These markers are more likely to be signals for other abnormalities as forceps or vacuum are not used in normal deliveries.
- The need to repair large tears after delivery.
Pelvic girdle pain. Hormones and enzymes work together to produce ligamentous relaxation and widening of the symphysis pubis during the last trimester of pregnancy. Most girdle pain occurs before birthing, and is known as diastasis of the pubic symphysis. Predisposing factors for girdle pain include maternal obesity.
Infection remains a major cause of maternal mortality and morbidity in the developing world. The work of Ignaz Semmelweis was seminal in the pathophysiology and treatment of puerperal fever and saved many lives.
Hemorrhage, or heavy blood loss, is still the leading cause of death of birthing mothers in the world today, especially in the developing world. Heavy blood loss leads to hypovolemic shock, insufficient perfusion of vital organs and death if not rapidly treated. Blood transfusion may be life saving. Rare sequelae include Hypopituitarism Sheehan's syndrome.
The maternal mortality rate (MMR) varies from 9 per 100,000 live births in the US and Europe to 900 per 100,000 live births in Sub-Saharan Africa.[33] Every year, more than half a million women die in pregnancy or childbirth.[34]
Fetal complications
Mechanical fetal injury
Risk factors for fetal birth injury include fetal macrosomia (big baby), maternal obesity, the need for instrumental delivery, and an inexperienced attendant. Specific situations that can contribute to birth injury include breech presentation and shoulder dystocia. Most fetal birth injuries resolve without long term harm, but brachial plexus injury may lead to Erb's palsy or Klumpke's paralysis.[35]
Neonatal infection
 Disability-adjusted life year for neonatal infections and other (perinatal) conditions per 100,000 inhabitants in 2004. Excludes prematurity and low birth weight, birth asphyxia and birth trauma which have their own maps/data.[36]no dataless than 150150-300300-450450-600600-750750-900900-10501050-12001200-13501350-15001500-1850more than 1850
Disability-adjusted life year for neonatal infections and other (perinatal) conditions per 100,000 inhabitants in 2004. Excludes prematurity and low birth weight, birth asphyxia and birth trauma which have their own maps/data.[36]no dataless than 150150-300300-450450-600600-750750-900900-10501050-12001200-13501350-15001500-1850more than 1850Neonates are prone to infection in the first month of life. Some organisms such as S. agalactiae (Group B Streptococcus) or (GBS) are more prone to cause these occasionally fatal infections. Risk factors for GBS infection include:
- prematurity (birth prior to 37 weeks gestation)
- a sibling who has had a GBS infection
- prolonged labour or rupture of membranes
Untreated sexually transmitted infections are associated with congenital and perinatal infections in neonates, particularly in the areas where rates of infection remain high. The overall perinatal mortality rate associated with untreated syphilis, for example, approached 40%.[37]
Neonatal death
Infant deaths (neonatal deaths from birth to 28 days, or perinatal deaths if including fetal deaths at 28 weeks gestation and later) are around 1% in modernized countries.
The most important factors affecting mortality in childbirth are adequate nutrition and access to quality medical care ("access" is affected both by the cost of available care, and distance from health services).[citation needed]
A 1983-1989 study by the Texas Department of State Health Services highlighted the differences in neonatal mortality (NMR) between high risk and low risk pregnancies. NMR was 0.57% for doctor-attended high risk births, and 0.19% for low risk births attended by non-nurse midwives. Conversely, some studies demonstrate a higher perinatal mortality rate with assisted home births.[38] Around 80% of pregnancies are low-risk. Factors that may make a birth high risk include prematurity, high blood pressure, gestational diabetes and a previous cesarean section.
Intrapartum asphyxia
Intrapartum asphyxia is the impairment of the delivery of oxygen to the brain and vital tissues during the progress of labour. This may exist in a pregnancy already impaired by maternal or fetal disease, or may rarely arise de novo in labour. This can be termed fetal distress, but this term may be emotive and misleading. True intrapartum asphyxia is not as common as previously believed, and is usually accompanied by multiple other symptoms during the immediate period after delivery. Monitoring might show up problems during birthing, but the interpretation and use of monitoring devices is complex and prone to misinterpretation. Intrapartum asphyxia can cause long-term impairment, particularly when this results in tissue damage through encephalopathy.[39]
Professions associated with childbirth
 Model of pelvis used in the beginning of the 20th century to teach technical procedures for a successful childbirth. Museum of the History of Medicine, Porto Alegre, Brazil
Model of pelvis used in the beginning of the 20th century to teach technical procedures for a successful childbirth. Museum of the History of Medicine, Porto Alegre, BrazilDifferent categories of birth attendants may provide support and care during pregnancy and childbirth, although there are important differences across categories based on professional training and skills, practice regulations, as well as nature of care delivered.
“Childbirth educators” are instructors who aim to educate pregnant women and their partners about the nature of pregnancy, labour signs and stages, techniques for giving birth, breastfeeding and newborn baby care. In the United States and elsewhere, classes for training as a childbirth educator can be found in hospital settings or through many independent certifying organizations such as Birthing From Within, BirthWorks, Brio Birth, CAPPA, HypBirth, HypnoBabies, HypnoBirthing, ICTC, ICEA, Lamaze, The Bradley Method, etc. Each organization teaches its own curriculum and each emphasizes different techniques. Information about each can be obtained through their individual websites.
Doulas are assistants who support mothers during pregnancy, labour, birth, and postpartum. They are not medical attendants; rather, they provide emotional support and non-medical pain relief for women during labour. Like childbirth educators and other assistive personnel, certification to become a doula is not compulsory, thus, anyone can call themself a doula or a childbirth educator.
Midwives are autonomous practitioners who provide basic and emergency health care before, during and after pregnancy and childbirth, generally to women with low-risk pregnancies. Midwives are trained to assist during labour and birth, either through direct-entry or nurse-midwifery education programs. Jurisdictions where midwifery is a regulated profession will typically have a registering and disciplinary body for quality control, such as the College of Midwives of British Columbia (CMBC) in Canada[40] or the Nursing and Midwifery Council (NMC) in the United Kingdom.[41]
In jurisdictions where midwifery is not a regulated profession, traditional or lay midwives may assist women during childbirth, although they do not typically receive formal health care education and training.
Medical doctors who practice obstetrics include categorically specialized obstetricians; family practitioners and general practitioners whose training, skills and practices include obstetrics; and in some contexts general surgeons. These physicians and surgeons variously provide care across the whole spectrum of normal and abnormal births and pathological labour conditions. Categorically specialized obstetricians are qualified surgeons, so they can undertake surgical procedures relating to childbirth. Some family practitioners or general practitioners also perform obstetrical surgery. Obstetrical procedures include cesarean sections, episiotomies, and assisted delivery. Categorical specialists in obstetrics are commonly dually trained in obstetrics and gynecology (OB/GYN), and may provide other medical and surgical gynecological care, and may incorporate more general, well-woman, primary care elements in their practices. Maternal-fetal medicine specialists are obstetrician/gynecologists subspecialized in managing and treating high-risk pregnancy and delivery.
Obstetric nurses assist midwives, doctors, women, and babies prior to, during, and after the birth process, in the hospital system. Some midwives are also obstetric nurses. Obstetric nurses hold various certifications and typically undergo additional obstetric training in addition to standard nursing training.
Society and culture
Childbirth routinely occurs in hospitals in much of Western society. Prior to the 20th century and in some countries to the present day it has more typically occurred at home.[42]
In Western and other cultures, age is reckoned from the date of birth, and sometimes the birthday is celebrated annually. East Asian age reckoning starts newborns at "1", incrementing each Lunar New Year.
Some families view the placenta as a special part of birth, since it has been the child's life support for so many months. Some parents like to see and touch this organ. In some cultures, parents plant a tree along with the placenta on the child's first birthday. The placenta may be eaten by the newborn's family, ceremonially or otherwise (for nutrition; the great majority of animals in fact do this naturally).[43] Most recently there is a category of birth professionals available who will encapsulate placenta for use as placenta medicine by postpartum mothers. The placenta is believed to provide hormones which ease the emotional roller coaster of the postpartum period and even prevent some cases of postpartum depression. The placenta is steamed and then dried in a dehydrator, after which it is made into gel caps that are taken for weeks or months. There is some research showing benefits for milk production in women and other positive studies in animal populations. Anecdotal reports suggest that women say that they suffer less postpartum blues, depression and anxiety using placenta medicine.
The exact location in which childbirth takes place is an important factor in determining nationality, in particular for birth aboard aircraft and ships.
Further information: AgeingSee also
- Advanced maternal age, an increase in age at first birth
- Amniotic stem cells
- Asynclitic birth, an abnormal birth position
- Coffin birth
- Homebirth
- Lamaze
- Bradley method of natural childbirth
- Natalism
- Natural childbirth
- Obstetrical Dilemma
- Partogram
- Postpartum depression (PPD)
- Postnatal
- Pre- and perinatal psychology
- Pre-labor
- Health care provider
- Traditional birth attendant
- Unassisted childbirth
- Vernix caseosa
- Waterbirth
References
- ^ The Columbia Encyclopedia, Sixth Edition. Copyright 2006 Columbia University Press.
- ^ ChildbirthConnection.org 50% increase in US Caesarean section from 1996-2006
- ^ CDD.gov
- ^ CTV.ca CTV News on caesarean sections
- ^ Zlotnick C, Johnson SL, Miller IW, Pearlstein T, Howard M. (Apr 2001). "Postpartum depression in women receiving public assistance: pilot study of an interpersonal-therapy-oriented group intervention". Am J Psychiatry 158 (4): 638–40. doi:10.1176/appi.ajp.158.4.638. PMID 11282702.
- ^ Healthline > Types of Forceps Used in Delivery February 2006. Reviewer: Douglas Levine, Gynecology Service/Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY.
- ^ Zhang J, Troendle JF, Yancey MK (2002). "Reassessing the labor curve in nulliparous women". American journal of obstetrics and gynecology 187 (4): 824–8. doi:10.1067/mob.2002.127142. PMID 12388957. http://www.medscape.com/viewarticle/450311.
- ^ Peisner DB, Rosen MG (1986). "Transition from latent to active labor.". Obstetrics and gynecology 68 (4): 448–51. PMID 3748488.
- ^ McDonald Susan J, Middleton Philippa, McDonald Susan J (2008). McDonald, Susan J. ed. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. doi:10.1002/14651858.CD004074.pub2.
- ^ Prendiville, W. J.; Elbourne, D.; McDonald, S. J.; Begley, C. M. (2000). Active versus expectant management in the third stage of labour. In Begley, Cecily M. "Cochrane Database of Systematic Reviews". Cochrane Database of Systematic Reviews (3). doi:10.1002/14651858.CD000007.
- ^ Zapardiel I, Delafuente-Valero J, Diaz-Miguel V, Godoy-Tundidor V, Bajo-Arenas JM (2009). "Pneumomediastinum during the fourth stage of labor". Gynecol. Obstet. Invest. 67 (1): 70–2. doi:10.1159/000162103. PMID 18843189.
- ^ "Technical Issues In Reproductive Health". http://www.columbia.edu/itc/hs/pubhealth/modules/reproductiveHealth/pregnancy.html. Retrieved 2010-01-24.
- ^ Gjerdingen DK, Froberg DG (January 1991). "The fourth stage of labor: the health of birth mothers and adoptive mothers at six-weeks postpartum". Fam Med 23 (1): 29–35. PMID 2001778.
- ^ Pillitteri, Adele (2009). Maternal and Child Health Nursing: Care of the Childbearing and Childrearing Family. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 1-58255-999-6.
- ^ Tranmer JE, Hodnett ED, Hannah ME, Stevens BJ (2005). "The effect of unrestricted oral carbohydrate intake on labor progress". J Obstet Gynecol Neonatal Nurs 34 (3): 319–28. doi:10.1177/0884217505276155. PMID 15890830.
- ^ a b Brinsmead M; Smith R, Singh B, Lewin T, Owens P (August 1985). "Peripartum concentrations of beta endorphin and cortisol and maternal mood states". Aust N Z J Obstet Gynaecol 25 (3): 194–7. doi:10.1111/j.1479-828X.1985.tb00642.x. PMID 2935137.
- ^ Kindredmedia.com.au, Giving Birth: The Endocrinology of Ecstacy
- ^ Eberhard J, Stein S, Geissbuehler V (2005). "Experience of pain and analgesia with water and land births". Journal of psychosomatic obstetrics and gynecology 26 (2): 127–33. doi:10.1080/01443610400023080. PMID 16050538.
- ^ Bahasadri Shohreh, Ahmadi-Abhari Sara, Dehghani-Nik Mojghan, Habibi Gholam Reza (2006). "Subcutaneous sterile water injection for labour pain: A randomised controlled trial". The Australian and New Zealand Journal of Obstetrics and Gynaecology 46 (2): 102. doi:10.1111/j.1479-828X.2006.00536.x.
- ^ Thorp JA, Breedlove G (1996). "Epidural analgesia in labour: an evaluation of risks and benefits". Birth (Berkeley, Calif.) 23 (2): 63–83. doi:10.1111/j.1523-536X.1996.tb00833.x. PMID 8826170. "Epidural analgesia is a safe and effective method of relieving pain in labour, but is associated with longer labour, more operative intervention, and increases in cost. It must remain an option; however, caregivers and consumers should be aware of associated risks. Women should be counseled about these risks and other pain-relieving options before the duress of labour."
- ^ Alehagen S, Wijma B, Lundberg U, Wijma K (2005). "Fear, pain and stress hormones during childbirth". Journal of psychosomatic obstetrics and gynaecology 26 (3): 153–65. doi:10.1080/01443610400023072. PMID 16295513.
- ^ Loftus JR, Hill H, Cohen SE (1995). "Placental transfer and neonatal effects of epidural sufentanil and fentanyl administered with bupivacaine during labor". Anesthesiology 83 (2): 300–8. doi:10.1097/00000542-199508000-00010. PMID 7631952.
- ^ Anim-Somuah M; Smyth R, Howell C (October 19, 2005). Anim-Somuah, Millicent. ed. "Epidural versus non-epidural or no analgesia in labour". Cochrane Database Syst Rev. 4 (4): CD000331. doi:10.1002/14651858.CD000331.pub2. PMID 16235275.
- ^ Wei SQ, Luo ZC, Xu H, Fraser WD (September 2009). "The effect of early oxytocin augmentation in labor: a meta-analysis". Obstet Gynecol 114 (3): 641–9. doi:10.1097/AOG.0b013e3181b11cb8. PMID 19701046.
- ^ BellyBelly.com.au, Men at Birth - Should your bloke be there?
- ^ "European Biotech Company Biocell Center Opens First U.S. Facility for Preservation of Amniotic Stem Cells in Medford, Massachusetts | Reuters". 2009-10-22. http://www.reuters.com/article/pressRelease/idUS166682+22-Oct-2009+PRN20091022. Retrieved 2010-01-11.
- ^ "Europe's Biocell Center opens Medford office - Daily Business Update - The Boston Globe". 2009-10-22. http://www.boston.com/business/ticker/2009/10/europes_biocell.html. Retrieved 2010-01-11.
- ^ "The Ticker - BostonHerald.com". http://www.bostonherald.com/business/general/view/20091022the_ticker. Retrieved 2010-01-11.
- ^ a b "Mortality and Burden of Disease Estimates for WHO Member States in 2002" (xls). World Health Organization. 2002. http://www.who.int/entity/healthinfo/statistics/bodgbddeathdalyestimates.xls.
- ^ Van Lerberghe W, De Brouwere V. Of blind alleys and things that have worked: history’s lessons on reducing maternal mortality. In: De Brouwere V, Van Lerberghe W, eds. Safe motherhood strategies: a review of the evidence. Antwerp, ITG Press, 2001 (Studies in Health Services Organisation and Policy, 17:7–33). "Where nothing effective is done to avert maternal death, “natural” mortality is probably of the order of magnitude of 1,500/100,000."
- ^ ibid, p10
- ^ Zhu, BP; Grigorescu V, Le T, Lin M, Copeland G; Barone M; Turabelidze G (2006). "Labor dystocia and its association with interpregnancy interval". American Journal of Obstetrics and Gynecology 85: 810–814.
- ^ Maternal mortality in 2005. World Health Organization (2008).
- ^ "Maternal mortality ratio falling too slowly to meet goal". WHO. October 12, 2007.
- ^ Warwick, R., & Williams, P.L, ed (1973). Gray’s Anatomy (35th ed.). London: Longman. pp.1046
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Retrieved Nov. 11, 2009.
- ^ "Sexually transmitted infections: Infections and Transmission". World Health Organization. http://www.who.int/mediacentre/factsheets/fs110/en/.
- ^ Bastian, H.; Keirse, M.; Lancaster, P. (1998). "Perinatal death associated with planned home birth in Australia: population based study". BMJ 317 (7155): 384–388. doi:10.1136/bmj.317.7155.384. PMC 28632. PMID 9694754. http://bmj.bmjjournals.com/cgi/content/short/317/7155/384.
- ^ van Handel M, Swaab H, de Vries LS, Jongmans MJ (July 2007). "Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal asphyxia: a review". Eur. J. Pediatr. 166 (7): 645–54. doi:10.1007/s00431-007-0437-8. PMC 1914268. PMID 17426984. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1914268.
- ^ College of Midwives of British Columbia. Accessed 14 March 2011
- ^ UK Nursing and Midwifery Council. Accessed 14 March 2011
- ^ Stearns, Peter N. (1994). Encyclopedia of Social History. ISBN 0815303424. http://books.google.com/?id=kkIeyCEedrsC.
- ^ Having a Great Birth in Australia, David Vernon, Australian College of Midwives, 2005 p56
External links
- Child's growth after birth
- Medical Video showing Childbirth from the American Medical Video Journal
- Childbirth (Parto) - Spanish
Family planning and reproductive health Rights Education Planning Reproductive life plan · Childfree · Parenting (Childbirth, Adoption, Foster care) · Birth control · Safe sexHealth Pregnancy Medicine Disorder By country Related navboxes {{Birth control methods}} · {{Pregnancy}} · {{Sex}} · {{sexual abuse}} · {{STD/STI}} · {{Assisted reproductive technology}}
Pregnancy and childbirth Planning Conception Testing Prenatal AnatomyProceduresChildbirth PreparationRolesDeliveryPostpartum Obstetric history









Wikimedia Foundation. 2010.