- Fasciolosis
-
Fasciolosis Classification and external resources ICD-10 B66.3 ICD-9 121.3 DiseasesDB 4757 eMedicine ped/760 MeSH D005211 Fasciolosis also known as Fascioliasis, Fasciolasis, distomatosis and liver rot, is an important helminth disease caused by two trematodes Fasciola hepatica (the common liver fluke) and Fasciola gigantica. This disease belongs to the plant-borne trematode zoonoses. In Europe, the Americas and Oceania only F. hepatica is a concern, but the distributions of both species overlap in many areas of Africa and Asia.[1]
The definitive host range is very broad and includes many herbivorous mammals, including humans. The life cycle includes freshwater snails as an intermediate host of the parasite.[2] Recently, worldwide losses in animal productivity due to fasciolosis were conservatively estimated at over US$3.2 billion per annum.[3] In addition, fasciolosis is now recognized as an emerging human disease: the World Health Organization (WHO) has estimated that 2.4 million people are infected with Fasciola, and a further 180 million are at risk of infection.[4]
 Fasciola hepatica
Fasciola hepatica
Contents
Etiology
Fasciolosis is caused by two digenetic trematodes F. hepatica and F. gigantica. Adult flukes of both species are localized in the bile ducts of the liver or gallbladder. F. hepatica measures 2 to 3 cm and has a cosmopolitan distribution. F. gigantica measures 4 to 10 cm in length and the distribution of the species is limited to the tropics and has been recorded in Africa, the Middle East, Eastern Europe and south and eastern Asia.[2] In domestic livestock in Japan, diploid (2n = 20), triploid (3n = 30) and chimeric flukes (2n/3n) have been described, many of which reproduce parthenogenetically. As a result of this unclear classification, flukes in Japan are normally referred to as Fasciola spp.[5] Recent reports based on mitochondrial genes analysis has shown that Japanese Fasciola spp. is more closely related to F. gigantica than to F. hepatica.[6] In India, a species called F. jacksoni was described in elephants.[7]
Geographic Distribution
Human and animal fasciolosis occurs worldwide.[2] While animal fasciolosis is distributed in countries with high cattle and sheep production, human fasciolosis occurs, excepting Western Europe, in developing countries. Fasciolosis occurs only in areas where suitable conditions for intermediate hosts exist.
Human fasciolosis
Studies carried out in recent years have shown human fasciolosis to be an important public health problem.[8] Human fasciolosis has been reported from countries in Europe, America, Asia, Africa and Oceania. The incidence of human cases has been increasing in 51 countries of the five continents.[9][10] A global analysis shows that the expected correlation between animal and human fasciolosis only appears at a basic level. High prevalences in humans are not necessarily found in areas where fasciolosis is a great veterinary problem. For instance, in South America, hyperendemics and mesoendemics are found in Bolivia and Peru where the veterinary problem is less important, while in countries such as Uruguay, Argentina and Chile, human fasciolosis is only sporadic or hypoendemic.[10]
Europe
In Europe, human fasciolosis occur mainly in France, Spain, Portugal, and the former USSR.[10] France is considered an important human endemic area. A total of 5863 cases of human fasciolosis were recorded from nine French hospitals from 1970 to 1982.[11] Concerning the former Soviet Union, almost all reported cases were from the Tajik Republic.[10] Several papers referred to human fasciolosis in Turkey.[12] Recently, serological survey of human fasciolosis was performed in some parts of Turkey. The prevalence of the disease was serologically found to be 3.01% in Antalya Province, and between 0.9 and 6.1% in Isparta Province, Mediterranean region of Turkey.[13] In other European countries, fasciolosis is sporadic and the occurrence of the disease is usually combined with travelling to endemic areas.
Americas
In North America, the disease is very sporadic. In Mexico, 53 cases have been reported. In Central America, fasciolosis is a human health problem in the Caribbean islands, especially in zones of Puerto Rico and Cuba. Pinar del Rio Province and Villa Clara Province are Cuban regions where fasciolosis was hyperendemic. In South America, human fasciolosis is a serious problem in Bolivia, Peru, and Ecuador. These Andean countries are considered to be the area with the highest prevalence of human fasciolosis in the world. Well-known human hyperendemic areas are localized predominately in the high plain called altiplano. In the Northern Bolivian Altiplano, prevalences detected in some communities were up to 72% and 100% in coprological and serological surveys, respectively.[9] In Peru, F. hepatica in humans occurs throughout the country. The highest prevalences were reported in Arequipa, Mantaro Valley, Cajamarca Valley, and Puno Region.[1] In other South American countries like Argentina, Uruguay, Brazil, Venezuela and Colombia, human fasciolosis appear to be sporadic, despite the high prevalences of fasciolosis in cattle.
Africa
In Africa, human cases of fasciolosis, except in northern parts, have not been frequently reported. The highest prevalence was recorded in Egypt where the disease is distributed in communities living in the Nile Delta.[1]
Asia
In Asia, the most human cases were reported in Iran, especially in Gīlān Province, on the Caspian Sea. It was mentioned that more than 10,000 human cases were detected in Iran. In eastern Asia, human fasciolosis appears to be sporadic. Few cases were documented in Japan, Koreas, Vietnam, and Thailand.[9]
Australia and the Oceania
In Australia, human fasciolosis is very rare (only 12 cases documented). In New Zealand, F. hepatica has never been detected in humans.[9]
Animal fasciolosis
Countries where fasciolosis in livestock was repeatedly reported:
- Europe: UK, Ireland, France, Portugal, Spain, Switzerland, Italy, Netherlands, Turkey, Germany, Poland
- Asia: Russia, Thailand, Iraq, Iran, China, Vietnam, India, Nepal, Japan, Korea,[Philippines
- Africa: Kenya, Zimbabwe, Nigeria, Egypt, Gambia, Morocco
- Australia and the Oceania: Australia, New Zealand
- Americas:United States, Mexico, Cuba, Peru, Chile, Uruguay, Argentina, Jamaica, Brazil
On September 8, 2007, Veterinary officials in South Cotabato, Philippines said that laboratory tests on samples from cows, carabaos, and horses in the province's 10 towns and lone city showed the level of infection at 89.5%, a sudden increase of positive cases among large livestock due to the errati] weather condition in the area. They mus be treated forthwih to prevent complications with surra and hemorrhagic septicemia diseases. Surra already affected all barangays of the Surallah town.[14]
Source of infection for humans and transmission
Human F. hepatica infection is determined by the presence of the intermediate snail hosts, domestic herbivorous animals, climatic conditions and the dietary habits of man.[8] Sheep, goats and cattle are considered the predominant animal reservoirs. While other animals can be infected, they are usually not very important for human disease transmission. On the other hand, some authors have observed that donkeys and pigs contribute to disease transmission in Bolivia.[15] Among wild animals, it has been demonstrated that the peridomestic rat (Rattus rattus) may play an important role in the spread as well as in the transmission of the parasite in Corsica.[16] In France, nutria (Myocastor coypus) was confirmed as a wild reservoir host of F. hepatica.[17] Humans are infected by ingestion of aquatic plants that contain the infected metacercariae.[18] Several species of aquatic vegetables are known as a vehicle of human infection. In Europe, Nasturtium officinale (common watercress), N. silvestris, Rorippa amphibia (wild watercress), Taraxacum dens leonis (dandelion leaves), Valerianella olitora (lamb's lettuce), and Mentha viridis (spearmint) were reported as a source of human infections.[9] In the Northern Bolivian Altiplano, some authors suggested that several aquatic plants such as bero-bero (watercress), algas (algae), kjosco and tortora could act as a source of infection for humans.[19] Because F. hepatica cercariae also encyst on water surface, humans can be infected by drinking of fresh untreated water containing metacercariae.[8] In addition, an experimental study suggested that humans consuming raw liver dishes from fresh livers infected with juvenile flukes could become infected.[20]
Intermediate hosts

Intermediate hosts of F. hepatica are freshwater snails from family Lymnaeidae.[2][21] Snails from family Planorbidae act as an intermediate host of F. hepatica very occasionally.[1]
Pathogenesis
The development of infection in definitive host is divided into two phases: the parenchymal (migratory) phase and the biliary phase.[22] The parenchymal phase begins when excysted juvenile flukes penetrate the intestinal wall. After the penetration of the intestine, flukes migrate within the abdominal cavity and penetrate the liver or other organs. F. hepatica has a strong predilection for the tissues of the liver.[23] Occasionally, ectopic locations of flukes such as the lungs, diaphragm, intestinal wall, kidneys, and subcutaneous tissue can occur.[8][24] During the migration of flukes, tissues are mechanically destroyed and inflammation appears around migratory tracks of flukes. The second phase (the biliary phase) begins when parasites enter the biliary ducts of the liver. In biliary ducts, flukes mature, feed on blood, and produce eggs. Hypertrophy of biliar ducts associated with obstruction of the lumen occurs as a result of tissue damage.
Clinical signs
In humans
 Hypertrophia of bile ducts in liver caused by F. hepatica (liver section; goat)
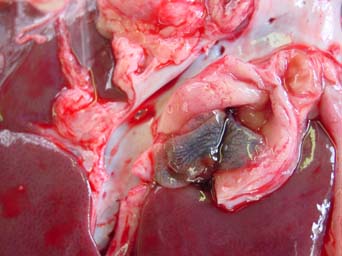
Hypertrophia of bile ducts in liver caused by F. hepatica (liver section; goat)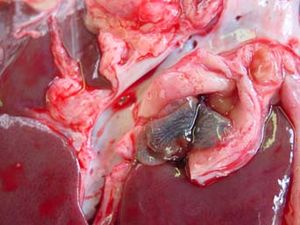 Adult flukes Fasciola hepatica in bile ducts (liver of goat)
Adult flukes Fasciola hepatica in bile ducts (liver of goat)The course of fasciolosis in humans has 4 main phases:[9]
- Incubation phase: from the ingestion of metacercariae to the appearance of the first symptoms; time period: few days to 3 months; depends on number of ingested metacercariae and immune status of host
- Invasive or acute phase: fluke migration up to the bile ducts. This phase is a result of mechanical destruction of the hepatic tissue and the peritoneum by migrating juvenile flukes causing localized and or generalized toxic and allergic reactions.[25] The major symptoms of this phase are:
- Fever: usually the first symptom of the disease; 40-42°C
- Abdominal pain
- Gastrointestinal disturbances: loss of appetite, flatulence, nausea, diarrhoea
- Urticaria
- Respiratory symptoms (very rare): cough, dyspnoea, chest pain, hemoptysis
- Hepatomegaly and splenomegaly
- Ascites
- Anaemia
- Jaundice
- Latent phase: This phase can last for months or years. The proportion of asymptomatic subjects in this phase is unknown. They are often discovered during family screening after a patient is diagnosed.[9]
- Chronic or obstructive phase:
This phase may develop months or years after initial infection. Adult flukes in the bile ducts cause inflammation and hyperplasia of the epithelium. The resulting cholangitis and cholecystitis, combined with the large body of the flukes, are sufficient to cause mechanical obstruction of the biliary duct. In this phase, biliary colic, epigastric pain, fatty food intolerance, nausea, jaundice, pruritus, right upper-quadrant abdominal tenderness, etc., are clinical manifestations indistinguishable from cholangitis, cholecystitis and cholelithiasis of other origins. Hepatic enlargement may be associated with an enlarged spleen or ascites. In case of obstruction, the gall bladder is usually enlarged and edematous with thickening of the wall. Fibrous adhesions of the gall bladder to adjacent organs are common. Lithiasis of the bile duct or gall bladder is frequent and the stones are usually small and multiple.[9]
In animals
Clinical signs of fasciolosis are always closely associated with infectious dose (amount of ingested metacercariae). In sheep, as the most common definitive host, clinical presentation is divided into 4 types:[22][23]
- Acute Type I Fasciolosis: infectious dose is more than 5000 ingested metacercariae. Sheep suddenly die without any previous clinical signs. Ascites, abdominal haemorrhage, icterus, pallor of membranes, weakness may be observed in sheep.
- Acute Type II Fasciolosis: infectious dose is 1000-5000 ingested metacercariae. As above, sheep die but briefly show pallor, loss of condition and ascites.
- Subacute Fasciolosis: infectious dose is 800-1000 ingested metacercariae. Sheep are lethargic, anemic and may die. Weight loss is dominant feature.
- Chronic Fasciolosis: infectious dose is 200-800 ingested metacercariae. Asymptomatic or gradual development of bottle jaw and ascites (ventral edema), emaciation, weight loss.
In blood, anemia, hypoalbuminemia, and eosinophilia may be observed in all types of fasciolosis.[23] Elevation of liver enzyme activities, such a glutamate dehydrogenase (GLDH), gamma-glutamyl transferase (GGT), and lactate dehydrogenase (LDH), is detected in subacute or chronic fasciolosis from 12-15 week after ingestion of metacercariae.[26][27] Economical effect of fasciolosis in sheep consists in sudden deaths of animals as well as in reduction of weight gain and wool production.[28][29] In goats and cattle, the clinical manifestation is similar to sheep. However, acquired resistance to F. hepatica infection is well-known in adult cattle.[30][31] Calves are susceptible to disease but in excess of 1000 metacercariae are usually required to cause clinical fasciolosis. In this case the disease is similar to sheep and is characterized by weight loss, anemia, hypoalbuminemia and (after infection with 10,000 metacercariae) death.[24] Importance of cattle fasciolosis consist in economic losses caused by condemnation of livers at slaughter and production losses especially due to reduced weight gain.[32]
In sheep and sometimes cattle, the damaged liver tissue may become infected by the Clostridium bacteria C. novyi type B. The bacteria will release toxins into the bloodstream resulting in what is known as black disease. There is no cure and death follows quickly. As C. novyi is common in the environment, black disease is found wherever populations of liver flukes and sheep overlap.[33]
Resistance to infection
Mechanisms of resistance have been studied by several authors in different animal species. These studies may help to better understand the immune response to F. hepatica in host and are necessary in development of vaccine against the parasite. It has been established that cattle acquire resistance to challenge infection with F. hepatica and F. gigantica when they have been sensitized with primary patent or drug-abbreviated infection.[30] Resistance to fasciolosis was also documented in rats.[34] On the other hand, sheep and goats are not resistant to re-infection with F. hepatica.[35][36] However, there is evidence that two sheep breeds, in particular Indonesian thin tail sheep and Red maasai sheep, are resistant to F. gigantica.[37][38] No reports concerning the resistance in humans are available.
Diagnosis
In humans, diagnosis of fasciolosis is usually achieved parasitologically by findings the fluke eggs in stool, and immunologically by ELISA and Western blot. Coprological examinations of stool alone are generally not adequate because infected humans have important clinical presentations long before eggs are found in the stools. Moreover, in many human infections, the fluke eggs are often not found in the faeces, even after multiple faecal examinations.[8][39] Furthermore, eggs of F. hepatica, F. gigantica and Fasciolopsis buski are morphologically indistinguishable.[39] Therefore, immunonological methods such ELISA and enzyme-linked immunoelectrotransfer blot, also called Western blot, are the most important methods in diagnosis of F. hepatica infection. These immunological tests are based on detection of species-specific antibodies from sera. The antigenic preparations used have been primarily derived from extracts of excretory/secretory products from adult worms, or with partially purified fractions.[40] Recently, purified native and recombinant antigens have been used, e.g. recombinant F. hepatica cathepsin L-like protease.[41] Methods based on antigen detection (circulating in serum or in faeces) are less frequent. In addition, biochemical and haematological examinations of human sera support the exact diagnosis (eosinophilia, elevation of liver enzymes). Ultrasonography and RTG of the abdominal cavity, biopsy of liver, and gallbladder punctuate can also be used. False fasciolosis (pseudofasciolosis) refers to the presence of eggs in the stool resulting not from an actual infection but from recent ingestion of infected livers containing eggs. This situation (with its potential for misdiagnosis) can be avoided by having the patient follow a liver-free diet several days before a repeat stool examination.[40] In animals, intravital diagnosis is based predominantly on faeces examinations and immunological methods. However, clinical signs, biochemical and haematological profile, season, climate conditions, epidemiology situation, and examinations of snails must be considered.[2][22] Similarly to humans, faeces examinations are not reliable. Moreover, the fluke eggs are detectable in faeces 8–12 weeks post-infection. In spite of that fact, faecal examination is still the only used diagnostic tool in some countries. While coprological diagnosis of fasciolosis is possible from 8-12 week post-infection (WPI) F. hepatica specific-antibodies are recognized using ELISA or Western blot since 2-4 week post-infection.[42][43] Therefore, these methods provide early detection of the infection.
Treatment and prevention
Anthelmintics
In humans
For high efficacy and safety, triclabendazole (Egaten) in dose 10–12 mg/kg is drug of choice in human fasciolosis.[44] No drug alternatives are available for humans. On the other hand, nitazoxanide were successfully used in human fasciolosis treatment in Mexico.[45] Bithionol is another drug of choice used for treatment of F. hepatica.[46] More recently, Mirazid, an Egyptian drug made from myrrh, has been investigated as an oral treatment of trematode-caused ailments including fascioliasis.[47]
In animals
 Formula of triclabendazole
Formula of triclabendazoleA number of drugs have been used in control fasciolosis in animals. Drugs differ in their efficacy, mode of action, price, and viability. Fasciolicides (drugs against Fasciola spp.) fall into five main chemical groups:[48]
- Halogenated phenols: bithionol (Bitin), hexachlorophene (Bilevon), nitroxynil (Trodax)
- Salicylanilides: closantel (Flukiver, Supaverm), rafoxanide (Flukanide, Ranizole)
- Benzimidazoles: triclabendazole (Fasinex), albendazole (Vermitan, Valbazen), mebendazol (Telmin), luxabendazole (Fluxacur)
- Sulphonamides: clorsulon (Ivomec Plus)
- Phenoxyalkanes: diamphenetide (Coriban)
Triclabendazole (Fasinex) is considered as the most common drug due to its high efficacy against adult as well as juvenile flukes. Triclabendazole is used in control of fasciolosis of livestock in many countries. Nevertheless, long-term veterinary use of triclabendazole has caused appearance of resistance to F. hepatica. In animals, triclabendazole resistance was first described in Australia,[49] later in Ireland[50] and Scotland[51] and more recently in the Netherlands.[52] Considering this fact, scientists have started to work on the development of new drug. Recently, a new fasciolicide was successfully tested in naturally and experimentally infected cattle in Mexico. This new drug is called 'Compound Alpha' and is chemically very similar to triclabendazole.[53]
See also
References
- ^ a b c d Mas-Coma S, Bargues MD, Valero MA (October 2005). "Fascioliasis and other plant-borne trematode zoonoses". Int. J. Parasitol. 35 (11-12): 1255–78. doi:10.1016/j.ijpara.2005.07.010. PMID 16150452. http://linkinghub.elsevier.com/retrieve/pii/S0020-7519(05)00272-9.
- ^ a b c d e Torgerson, P; Claxton J (1999). "Epidemiology and control.". In Dalton, JP. Fasciolosis. Wallingford, Oxon, UK: CABI Pub. pp. 113–49. ISBN 0-85199-260-9.
- ^ Spithill, TW; Smooker PM, Copeman DB (1999). "Fasciola gigantica: epidemiology, control, immunology and molecular biology". In Dalton, JP. Fasciolosis. Wallingford, Oxon, UK: CABI Pub. pp. 465–525. ISBN 0-85199-260-9.
- ^ Anonymus 1995. Control of Foodborne Trematode Infections. WHO Technical Series No. 849. WHO, Geneva, 157 pp.
- ^ Sakaguchi, Y. (1980). "Karyotype and gametogenesis of the common liver fluke, Fasciola sp., in Japan. Jap". J. Parasitol 29: 507–513.
- ^ Itagaki T, Tsutsumi K (May 1998). "Triploid form of Fasciola in Japan: genetic relationships between Fasciola hepatica and Fasciola gigantica determined by ITS-2 sequence of nuclear rDNA". Int. J. Parasitol. 28 (5): 777–81. doi:10.1016/S0020-7519(98)00037-X. PMID 9650058. http://linkinghub.elsevier.com/retrieve/pii/S002075199800037X.
- ^ Singh, K.P.; Srivastava, V.K.; Prasad, A.; Pandey, A.P. (1994). "Pathology due to Fasciola jacksoni in Indian elephants Elephas indicus". Ind. J. Anim. Scien 64: 802–804.
- ^ a b c d e Chen, M.G., Mott, K.E., 1990. "Progress in assessment of morbidity due to Fasciola hepatica infection: a review of recent literature". Trop. Dis. Bull. 87, R1–R38.
- ^ a b c d e f g h Mas-Coma, S; Bargues MD, Esteban JG (1999). "Human fasciolosis.". In Dalton, JP. Fasciolosis. Wallingford, Oxon, UK: CABI Pub. pp. 411–34. ISBN 0-85199-260-9.
- ^ a b c d Esteban, J.G., Bargues, M.D., Mas-Coma, S., 1998. "Geographical distribution, diagnosis and treatment of human fascioliasis: a review". Res. Rev. Parasitol. 58, 13–42.
- ^ Danis, M., Nozais, J.P., Chandenier, J., 1985. "La distomatose à Fasciola hepatica, II: La fasciolose humaine en France". Action Vet. 907.
- ^ Yilmaz H, Gödekmerdan A (October 2004). "Human fasciolosis in Van Province, Turkey". Acta Trop. 92 (2): 161–2. doi:10.1016/j.actatropica.2004.04.009. PMID 15350869. http://linkinghub.elsevier.com/retrieve/pii/S0001-706X(04)00152-4.
- ^ Demirci, M., 2003. Insanlarda epidemiyoloji. In: Tinar, R., Korkmaz, M. (Eds.), Fasciolosis. Türkiye Parazitoloji Derněgi, META Basim, İzmir, pp. 343–358 (in Turkish).
- ^ GMA NEWS.TV, Rise in animal liver fluke cases alarms South Cotabato
- ^ Mas-Coma, S.; Rodriguez, A.; Bargues, M.D.; Valero, M.A.; Coello, J.; Angles, R. (1998). "Secondary reservoir role of domestic animals other than sheep and cattle in fascioliasis transmission on the northern Bolivian Altiplano". Res. Rev. Parasitol 57: 39–46.
- ^ Mas-Coma, S.; Fons, R.; Feliu, C.; Bargues, M.D.; Valero, M.A.; Galán-Puchades, M.T. (1988). "Small mammals as natural definitive hosts of the liver fluke, Fasciola hepatica Linnaeus, 1758 (Trematoda: Fasciolidae): a review and two new records of epidemiologic interest on the island of Corsica". Rivista di Parassitologia 5: 73–78.
- ^ Menard, A.; Agoulon, A.; L'Hostis, M.; Rondelaud, D.; Collard, S.; Chauvin, A. (2001). "Myocastor coypus as a reservoir host of Fasciola hepatica in France". Vet. Res. 32 (5): 499–508. doi:10.1051/vetres:2001141. PMID 11592619.
- ^ Markell, E.K., Voge, M., 1999. Medical Parasitology, eighth ed.. Saunders Company Publication, pp. 185–188.
- ^ Bjorland, J.; Bryan, R.T.; Strauss, W.; Hillyer, G.V.; McAuley, J.B. (1995). "An outbreak of acute fascioliasis among Aymara Indians in the Bolivian Altiplano". Clin. Infect. Dis. 21 (5): 1228–1233. doi:10.1093/clinids/21.5.1228. PMID 8589147.
- ^ Taira, N.; Yoshifuji, H.; Boray, J.C. (1997). "Zoonotic potential of infection with Fasciola spp. by consumption of freshly prepared raw liver containing immature flukes". Int. J. Parasitol 27 (7): 775–779. doi:10.1016/S0020-7519(97)00038-6. PMID 9279579.
- ^ Graczyk, TK; Fried B (1999). "Development of Fasciola hepatica in the intermediate host.". In Dalton, JP. Fasciolosis. Wallingford, Oxon, UK: CABI Pub. pp. 31–46. ISBN 0-85199-260-9.
- ^ a b c Dubinský, P., 1993. Trematódy a trematodózy. In: Jurášek, V., Dubinský, P. a kolektív, Veterinárna parazitológia. Príroda a.s., Bratislava, 158–187. (in Slovakian)
- ^ a b c Behm, C.A., Sangster, N.C., 1999. Pathology, pathophysiology and clinical aspects. In: Dalton, J.P. (Ed.), Fasciolosis. CAB International Publishing, Wallingford, pp. 185–224.
- ^ a b Boray JC (1969). "Experimental fascioliasis in Australia". Adv. Parasitol. 7: 95–210. doi:10.1016/S0065-308X(08)60435-2. PMID 4935272.
- ^ Facey, R.V., Marsden, P.D., 1960. Fascioliasis in man: an outbreak in Hampshire. Brit. Med. J. ii, 619–625.
- ^ Anderson, P.H., Matthews, J.G., Berrett, S., Brush, P.J., Patterson, D.S., 1981. Changes in plasma enzyme activities and other blood components in response to acute and chronic liver damage in cattle. Res Vet Sci. 31, 1-4.
- ^ Sykes, A.R., Coop, A.R., Robinson, M.G., 1980. Chronic subclinical ovine fascioliasis: plasma glutamate dehydrogenase, gamma glutamyl transpeptidase and aspartate aminotransferase activities and their significance as diagnostic aids. Res. Vet. Sci. 28, 71–78.
- ^ Sinclair, K.B. (1962). "Observations on the clinical pathology of ovine fascioliasis. Brit". Vet. J. 118: 37–53.
- ^ Roseby, F.B. (1970). "The effect of fasciolosis on the wool production of merino sheep". Aust. Vet. J. 46 (8): 361–365. doi:10.1111/j.1751-0813.1970.tb15573.x. PMID 5471269.
- ^ a b Haroun ET, Hillyer GV (March 1986). "Resistance to fascioliasis--a review". Vet. Parasitol. 20 (1-3): 63–93. doi:10.1016/0304-4017(86)90093-2. PMID 3518218.
- ^ Doyle, J.J., 1973. The relationship between the duration of a primary infection and the subsequent development of an acquired resistance to experimental infections with Fasciola hepatica in calves. Res. Vet. Sci., 14, 97-103.
- ^ Phiri IK, Phiri AM, Harrison LJ (November 2006). "Serum antibody isotype responses of Fasciola-infected sheep and cattle to excretory and secretory products of Fasciola species". Vet. Parasitol. 141 (3-4): 234–42. doi:10.1016/j.vetpar.2006.05.019. PMID 16797844. http://linkinghub.elsevier.com/retrieve/pii/S0304-4017(06)00336-0.
- ^ Merck Veterinary Manual - Infectious Necrotic Hepatitis
- ^ van Milligen FJ, Cornelissen JB, Bokhout BA (August 1998). "Location of induction and expression of protective immunity against Fasciola hepatica at the gut level: a study using an ex vivo infection model with ligated gut segments". J. Parasitol. (The Journal of Parasitology, Vol. 84, No. 4) 84 (4): 771–7. doi:10.2307/3284586. JSTOR 3284586. PMID 9714209.
- ^ Chauvin A, Bouvet G, Boulard C (October 1995). "Humoral and cellular immune responses to Fasciola hepatica experimental primary and secondary infection in sheep". Int. J. Parasitol. 25 (10): 1227–41. doi:10.1016/0020-7519(95)00039-5. PMID 8557470. http://linkinghub.elsevier.com/retrieve/pii/0020-7519(95)00039-5.
- ^ Martínez-Moreno A, Martínez-Moreno FJ, Acosta I, Gutiérrez PN, Becerra C, Hernández S (1997). "Humoral and cellular immune responses to experimental Fasciola hepatica infections in goats". Parasitol. Res. 83 (7): 680–6. doi:10.1007/s004360050319. PMID 9272558. http://link.springer.de/link/service/journals/00436/bibs/7083007/70830680.htm.
- ^ Roberts JA, Estuningsih E, Wiedosari E, Spithill TW (December 1997). "Acquisition of resistance against Fasciola gigantica by Indonesian thin tail sheep". Vet. Parasitol. 73 (3-4): 215–24. doi:10.1016/S0304-4017(97)00119-2. PMID 9477508. http://linkinghub.elsevier.com/retrieve/pii/S0304-4017(97)00119-2.
- ^ Wamae, L.W., 1996. Comparative pathogenesis and immunochemistry analysis of Fasciola gigantica infection in cattle and sheep. PhD Thesis. University of Edinburgh.
- ^ a b Hillyer, GV (1988). "Fascioliasis and fasciolopsiasis.". In A. Turano; Balows, Albert; M. Ohashi. Laboratory diagnosis of infectious diseases: principles and practices. 1: Bacterial, mycotic, and parasitic diseases. Berlin: Springer-Verlag. pp. 856–62. ISBN 0-387-96755-9.
- ^ a b Hillyer, GV (1999). "Immunodiagnosis of human and animal fasciolosis.". In Dalton JP. Fasciolosis. Wallingford, Oxon, UK: CABI Pub. pp. 435–47. ISBN 0-85199-260-9.
- ^ O'Neill SM, Parkinson M, Strauss W, Angles R, Dalton JP (April 1998). "Immunodiagnosis of Fasciola hepatica infection (fascioliasis) in a human population in the Bolivian Altiplano using purified cathepsin L cysteine proteinase". Am. J. Trop. Med. Hyg. 58 (4): 417–23. PMID 9574785. http://www.ajtmh.org/cgi/pmidlookup?view=long&pmid=9574785.
- ^ Zimmerman GL, Jen LW, Cerro JE, Farnsworth KL, Wescott RB (December 1982). "Diagnosis of Fasciola hepatica infections in sheep by an enzyme-linked immunosorbent assay". Am. J. Vet. Res. 43 (12): 2097–100. PMID 7165155.
- ^ Duménigo BE, Espino AM, Finlay CM, Mezo M (March 2000). "Kinetics of antibody-based antigen detection in serum and faeces of sheep experimentally infected with Fasciola hepatica". Vet. Parasitol. 89 (1-2): 153–61. doi:10.1016/S0304-4017(00)00206-5. PMID 10729655. http://linkinghub.elsevier.com/retrieve/pii/S0304-4017(00)00206-5.
- ^ Savioli L, Chitsulo L, Montresor A (1999). "New opportunities for the control of fascioliasis". Bull. World Health Organ. 77 (4): 300. PMC 2557651. PMID 10327707. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2557651.
- ^ Rossignol JF, Abaza H, Friedman H (1998). "Successful treatment of human fascioliasis with nitazoxanide". Trans. R. Soc. Trop. Med. Hyg. 92 (1): 103–4. doi:10.1016/S0035-9203(98)90974-9. PMID 9692168.
- ^ Ramachandran, A., 2000. Pharmacology Recall.
- ^ See, for example, Soliman, OE et al., Evaluation of myrrh (Mirazid) therapy in fascioliasis and intestinal schistosomiasis in children: immunological and parasitological study. J Egypt Soc Parasitol. 2004 Dec;34(3):941-66.PubMed.gov
- ^ Fairweather I, Boray JC (September 1999). "Fasciolicides: efficacy, actions, resistance and its management". Vet. J. 158 (2): 81–112. doi:10.1053/tvjl.1999.0377. PMID 10489266. http://linkinghub.elsevier.com/retrieve/pii/S1090-0233(99)90377-5.
- ^ Overend DJ, Bowen FL (July 1995). "Resistance of Fasciola hepatica to triclabendazole". Aust. Vet. J. 72 (7): 275–6. doi:10.1111/j.1751-0813.1995.tb03546.x. PMID 8534235.
- ^ O’Brien, D.J., 1998. Fasciolosis: a threat to livestock. Irish Vet. J. 51, 539–541.
- ^ Mitchell GB, Maris L, Bonniwell MA (October 1998). "Triclabendazole-resistant liver fluke in Scottish sheep". Vet. Rec. 143 (14): 399. PMID 9802201.
- ^ Moll L, Gaasenbeek CP, Vellema P, Borgsteede FH (July 2000). "Resistance of Fasciola hepatica against triclabendazole in cattle and sheep in The netherlands". Vet. Parasitol. 91 (1-2): 153–8. doi:10.1016/S0304-4017(00)00267-3. PMID 10889368. http://linkinghub.elsevier.com/retrieve/pii/S0304-4017(00)00267-3.
- ^ Ibarra F, Vera Y, Quiroz H, et al. (February 2004). "Determination of the effective dose of an experimental fasciolicide in naturally and experimentally infected cattle". Vet. Parasitol. 120 (1-2): 65–74. doi:10.1016/j.vetpar.2003.12.005. PMID 15019144. http://linkinghub.elsevier.com/retrieve/pii/S0304401703005053.
External links
- Fasciolosis Overview at CDC
- Immunodiagnosis of fasciolosis in Bolivian Altiplano
- Fasciolosis
- Pictures of adult flukes
- Pictures of F. hepatica eggs
Categories:- Helminthiases
- Veterinary helminthology
- Animal diseases


Wikimedia Foundation. 2010.