- Opisthorchiasis
-
Opisthorchiasis Classification and external resources ICD-10 B66.0 ICD-9 121.0 DiseasesDB 29303 MeSH D009889 Opisthorchiasis is an parasitic disease caused by species in the genus Opisthorchis (specifically, Opisthorchis viverrini and Opisthorchis felineus).
Medical care and loss of wages caused by Opisthorchis viverrini in Laos and in Thailand costs about $120 million annually[1] or $120 million per year can cost Northeast Thailand only.[2]
Infection of Opisthorchis viverrini and of other liver flukes in Asia affect the poor and poorest people.[3] Opisthorchiasis have received less attention in comparison of other diseases and it is a neglected disease in Asia.[3]
Contents
Prevalence
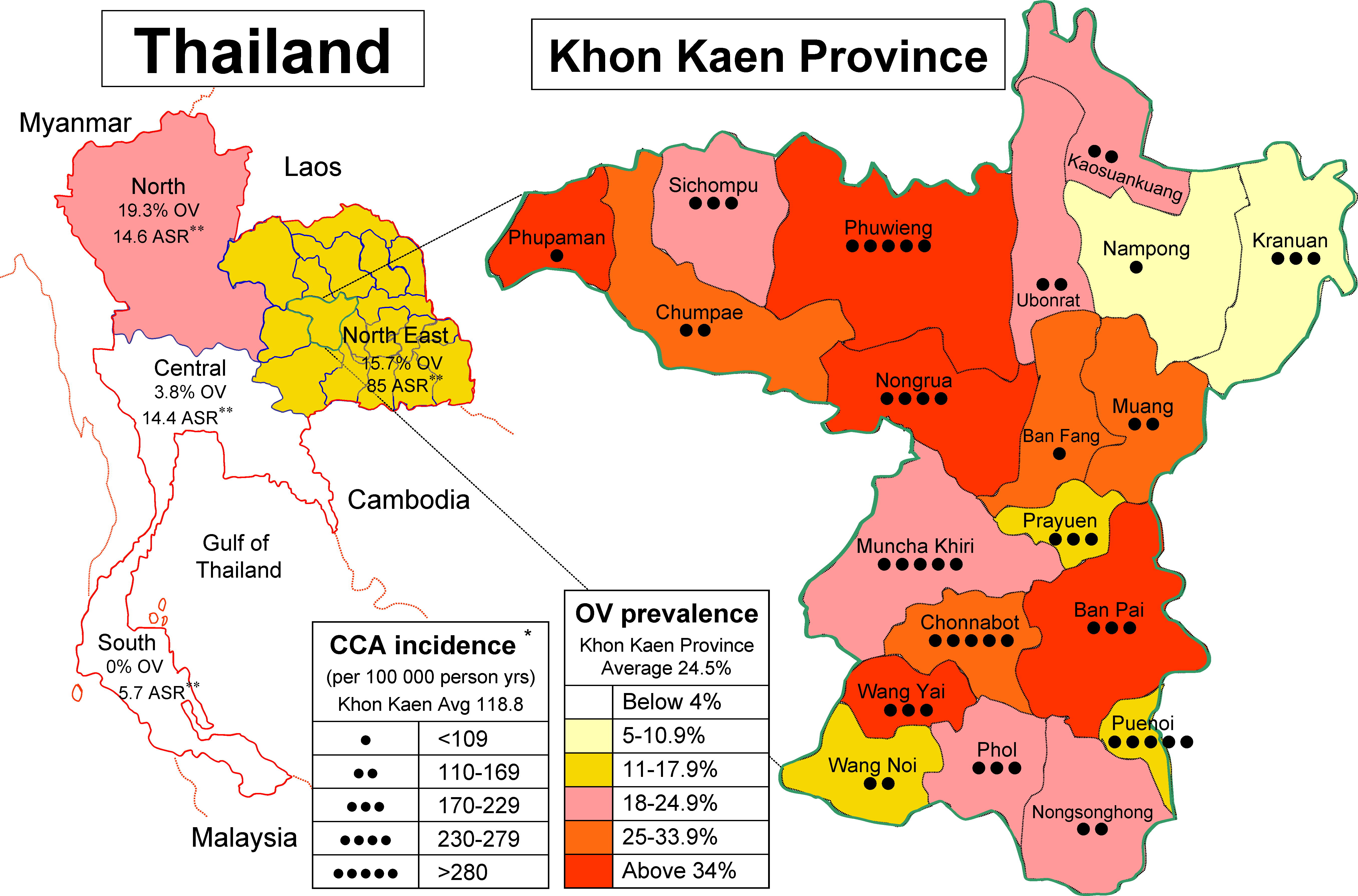
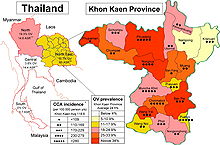 Prevalence of Opisthorchis viverrini in Thailand in 1990–2001 correlates with a higher cholangiocarcinoma:
Prevalence of Opisthorchis viverrini in Thailand in 1990–2001 correlates with a higher cholangiocarcinoma:
19.3% in North Thailand,
15.7% in North East Thailand,
3.8% in Central Thailand,
0% in Southern Thailand.[4]Opisthorchiasis is prevalent in geographical regions where raw cyprinid fishes are a staple of the diet of humans.[5] The prevalence of human infection can be as high as 70% in some regions, for example in Khon Kaen Province in Thailand.[5] The parasite establishes in the bile ducts of the liver as well as extrahepatic ducts and the gall bladder of the mammalian (definitive) host.[5]
Children under the age of 5 are rarely infected by Opisthorchis viverrini.[1]
In the Lao People's Democratic Republic, the prevalence of opisthorchiasis was:
- 40% in 1992 causing about 1 744 000 people infected[6]
In Thailand, the prevalence of opisthorchiasis was:
- scaterred reports by Verdun & Bruyant (1908), Leiper (1911), Prommas (1927), Bedier & Chesneau (1929)[7]
- The national control programme have started in Thailand in 1950.[8]
- 25% in 1953 causing about 2 million infected people.[6] The first widespread report of opisthorchiasis in Thailand was in 1953.[6]
- 1965: over 3.5 millions infected people[7]
- 14% in 1980-1981 causing about 7 million infected people.[9]
- 63.6% in 1984-1987,[10][8] but another WHO report mention prevalence 35% in Nort-east Thailand for 1984.[6]
- 35.6% in 1988[10]
- 30% in 1989[8]
- The decline of opisthorchiasis was caused by opisthorchiasis control programme, that includes health education including mass distribution of cooking pots[6] and using praziquantel, that was available since 1984.[6]
- 15.2% in 1991 causing 7 million infected people.[6] About 45 million people were at risk of infection.[6] There was prevalence 22.8% in North Thailand, 24.0% in North East Thailand, 7.3% in Central Thailand and 0.3% in Southern Thailand.[6]
- 12% in 1996[8]
- In 1992-1996 the National Public Health Development Plan used the strategy by the Faculty of Tropical Medicine, Mahidol University against opisthorchiasis.[6]
- 7% in 2000[8]
- 9.4% in 2001[10] In Thailand, the prevalence of opisthorchiasis is 9.4 % in 2001,[10] causing about 6 million people are infected with Opisthorchis viverrini.[11][4]
Opisthorchis viverrini was thought to be the only species of liver fluke in Thailand,[9] but PCR techniques have revealed also Clonorchis sinensis in (central) Thailand in 2008.[12]
Another reference from 2002 lists worldwide number of cases about 9 million (without year of estimation).[1] In Thailand, about 7.3 million.[1] About 50 million people are at risk of infection.[1]
In 2005, 67.3 million of people worldwide are at risk of infection.[13]
Keiser & Utzinger (2005)[13] have speculated that aquaculture development is the key risk factor for foodborne trematodiases including opisthorchiasis caused by Opisthorchis viverrini.[13]
Symptoms
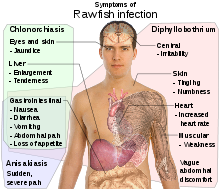 Symptoms of opisthorchiasis/clonorchiasis.Main article: clonorchiasis
Symptoms of opisthorchiasis/clonorchiasis.Main article: clonorchiasisSymptoms of opisthorchiasis (caused by Opisthorchis spp.) are indistinguishable from clonorchiasis (caused by Clonorchis sinensis),[2] so the disease should be referred as clonorchiasis.[2]
About 80% of infected people have no symptoms, though they can have eosinophilia.[1] This is when the infection is weak and there are less than 1000 eggs in one gram in feces.[1]
When there are 10.000-30.000 eggs in one gram of feces, then the infection is heavy.[1] Symptoms of heavier infections with Opisthorchis viverrini may include: diarrhoea, pain in epigastric and pain in the upper right quadrant, lack of appetite (anorexia), fatigue, yellowing of the eyes and skin (jaundice) and mild fever.[1]
These parasites are long-lived and cause heavy chronic infections may led to accumulation of fluid in legs (edema) and in the peritoneal cavity (ascites),[1] enlarged non-functional gall-bladder[1] and also cholangitis,[5] which can lead to periductal fibrosis, cholecystitis and cholelithiasis, obstructive jaundice, hepatomegaly and/or fibrosis of the periportal system.[5]
Importantly, both experimental and epidemiological evidence strongly implicates Opisthorchis viverrini infections in the etiology of a malignant cancer of the bile ducts (cholangiocarcinoma) in humans which has a very poor prognosis.[5] Indeed, Clonorchis sinensis and Opisthorchis viverrini are both categorized by the International Agency for Research on Cancer (IARC) as Group 1 carcinogens.[5]
In humans, the onset of cholangiocarcinoma occurs with chronic opisthorchiasis, associated with hepatobiliary damage, inflammation, periductal fibrosis and/or cellular responses to antigens from the infecting fluke.[5] These conditions predispose to cholangiocarcinoma, possibly through an enhanced susceptibility of DNA to damage by carcinogens.[5] Chronic hepatobiliary damage is reported to be multi-factorial and considered to arise from a continued mechanical irritation of the epithelium by the flukes present, particularly via their suckers, metabolites and excreted/secreted antigens as well as immunopathological processes.[5] In regions where Opisthorchis viverrini is highly endemic, the incidence of cholangiocarcinoma is unprecedented.[5] For instance, cholangiocarcinomas represent 15% of primary liver cancer worldwide, but in Thailand's Khon Kaen region, this figure escalates to 90%, the highest recorded incidence of this cancer in the world.[5] Of all cancers worldwide from 2002, 0.02% were cholangiocarcinoma caused by Opisthorchis viverrini.[4]
The cancer of the bile ducts caused by opisthorchiasis occur in the ages 25–44 years in Thailand.[6]
Diagnosis
For medical diagnosis there is need to find eggs of Opisthorchis viverrini in feces[1] using Kato technique.[6]
An antigen 89 kDa of Opisthorchis viverrini can be detected by ELISA test.[1]
A PCR test capable of amplifying a segment of the internal transcribed spacer region of ribosomal DNA for the opisthorchiid and heterophyid flukes eggs taken directly from faeces was developed and evaluated in a rural community in central Thailand.[12] The lowest quantity of DNA that could be amplified from individual adults of Opisthorchis viverrini was estimated to 0.6 pg.[12]
Prevention
Currently, there is no effective chemotherapy to combat cholangiocarcinoma, such that intervention strategies need to rely on the prevention or treatment of liver fluke infection/disease.[5] Although effective prevention could be readily achieved by persuading people to consume cooked fish (via education programs), the ancient cultural custom to consume raw, undercooked or freshly pickled fish persists in endemic areas.[5] Cooking or deep-freezing (-20 °C for 7 days)[8] of food made of fish is sure method of prevention.[1] Methods for prevention of Opisthorchis viverrini in aquaculture fish ponds were proposed by Khamboonruang et al. (1997).[14]
Treatment
There was unsuccessful use of chloroquine for opisthorchiasis treatment in 1951-1968.[6]
Thus, currently, the control of opisthorchiasis relies predominantly on anthelmintic treatment with praziquantel.[5] The single dose of praziquantel of 40 mg/kg is effective against opisthorchiasis and also against schistosomiasis.[6] A randomised-controlled trial published in 2011 showed that the broad-spectrum anti-helminthic, tribendimidine, appears to be at least as efficacious as praziquantel.[15]
Artemisinin was also found to have anthelmintic activity against Opisthorchis viverrini.[16]
Despite the efficacy of this compound, the lack of an acquired immunity to infection predisposes humans to reinfections in endemic regions.[5] In addition, under experimental conditions, the short-term treatment of Opisthorchis viverrini-infected hamsters with praziquantel (400 mg per kg of live weight) has been shown to induce a dispersion of parasite antigens, resulting in adverse immunopathological changes as a result of oxidative and nitrative stresses following re-infection with Opisthorchis viverrini, a process which has been proposed to initiate and/or promote the development of cholangiocarcinoma in humans.[5]
Given the current reliance on a single trematocidal drug against Opisthorchis viverrini, there is substantial merit in searching for new intervention methods, built on a detailed understanding of the interplay between the parasites and their hosts as well as the biology of the parasites themselves at the molecular level.[5] Furthermore, the characterization of the genes expressed in these parasites should assist in elucidating the molecular mechanisms by which opisthorchiasis initiate and enhance the development of cholangiocarcinoma.[5]
References
- ^ a b c d e f g h i j k l m n Muller R. & Wakelin D. (2002). Worms and human disease. CABI. page 43-44.
- ^ a b c King1 S. & Scholz T. (2001). "Trematodes of the family Opisthorchiidae: a minireview". Korean Journal of Parasitology 39(3): 209–221. doi:10.3347/kjp.2001.39.3.209, PMC PMC2721069.
- ^ a b Sripa B. (2008) "Concerted Action Is Needed to Tackle Liver Fluke Infections in Asia". PLoS Neglected Tropical Diseases 2(5): e232. doi:10.1371/journal.pntd.0000232.
- ^ a b c Sripa B., Kaewkes S., Sithithaworn P., Mairiang E., Laha T., et al. (2007). "Liver Fluke Induces Cholangiocarcinoma". PLoS Medicine 4(7): e201. doi:10.1371/journal.pmed.0040201.
- ^ a b c d e f g h i j k l m n o p q r s Young N.D., Campbell B.E., Hall R.S., Jex A.R., Cantacessi C., et al. (2010). "Unlocking the Transcriptomes of Two Carcinogenic Parasites, Clonorchis sinensis and Opisthorchis viverrini. PLoS Neglected Tropical Diseases 4(6): e719. doi:10.1371/journal.pntd.0000719.
- ^ a b c d e f g h i j k l m n World Health Organization (1995). Control of Foodborne Trematode Infection. WHO Technical Report Series. 849. PDF part 1, PDF part 2. page 89-91.
- ^ a b Wykoff D.E., Harinasuta C., Juttijudata P. & Winn M.M. (1965). "Opisthorchis viverrini in Thailand: The Life Cycle and Comparison with O. felineus". The Journal of Parasitology 51(2): 207-214. PubMed, JSTOR.
- ^ a b c d e f World Health Organization (2004). REPORT JOINT WHO/FAO WORKSHOP ON FOOD-BORNE TREMATODE INFECTIONS IN ASIA. Report series number: RS/2002/GE/40(VTN). 55 pp. PDF. pages 15-17.
- ^ a b Harinasuta C. & Harinasuta T. (1984). "Opisthorchis viverrini: life cycle, intermediate hosts, transmission to man and geographical distribution in Thailand". Arzneimittelforschung 34(9B): 1164-1167. PubMed
- ^ a b c d Jongsuksuntigul P. & Imsomboon T. (2003). "Opisthorchiasis control in Thailand". Acta Tropica 88(3): 229–232. doi:10.1016/j.actatropica.2003.01.002.
- ^ Laha T., Pinlaor P., Mulvenna J., Sripa B., Sripa M., et al. (2007). "Gene discovery for the carcinogenic human liver fluke, Opisthorchis viverrini. BMC Genomics 8: 189. doi:10.1186/1471-2164-8-189.
- ^ a b c Traub R.J., Macaranas J., Mungthin M., Leelayoova S., Cribb T., et al. (2009). "A New PCR-Based Approach Indicates the Range of Clonorchis sinensis Now Extends to Central Thailand". PLoS Neglected Tropical Diseases 3(1): e367. doi:10.1371/journal.pntd.0000367.
- ^ a b c Keiser J. & Utzinger J. (2005). "Emerging foodborne trematodiasis". Emerging Infectious Diseases [serial on the Internet]. 2005 Oct. Available from http://www.cdc.gov/ncidod/EID/vol11no10/05-0614.htm
- ^ Khamboonruang C., Keawvichit R., Wongworapat K., Suwanrangsi S., Hongpromyart M., Sukhawat K., Tonguthai K. & Lima dos Santos C. A. (1997). "Application of hazard analysis critical control point (HACCP) as a possible control measure for Opisthorchis viverrini infection in cultured carp (Puntius gonionotus)". The Southeast Asian journal of tropical medicine and public health 28(Suppl 1): 65-72. PubMed.
- ^ Soukhathammavong P, Odermatt P, Sayasone S, et al. (2011). "Efficacy and safety of mefloquine, artesunate, mefloquine—artesunate, tribendimidine, and praziquantel in patients with Opisthorchis viverrini: a randomised, exploratory, open-label, phase 2 trial". Lancet Infect Dis 11 (2): 110–118. doi:10.1016/S1473-3099(10)70250-4.
- ^ Keiser J. & Utzinger J. (2007). "Artemisinins and synthetic trioxolanes in the treatment of helminth infections". Current opinion in infectious diseases 20(6):605-612. PubMed.
Categories:- Medicine stubs
- Helminthiases

Wikimedia Foundation. 2010.