- Dydrogesterone
-
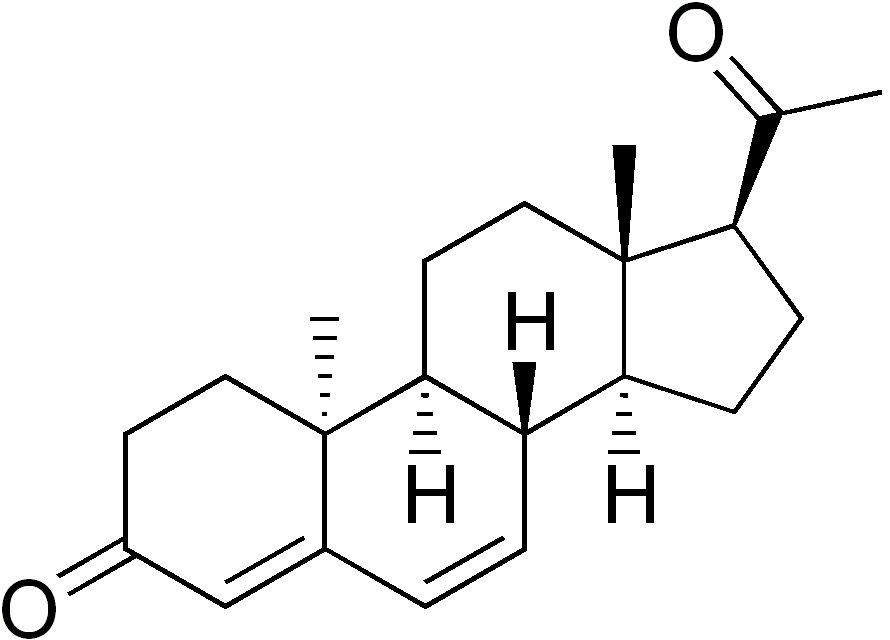
Dydrogesterone 
Systematic (IUPAC) name 17-acetyl-10, 13-dimethyl-1,2,8,9,11,12,14,15,16,17- decahydrocyclopenta[a] phenanthren- 3-one Clinical data AHFS/Drugs.com International Drug Names Pregnancy cat. ? Legal status ? Pharmacokinetic data Bioavailability 28% Metabolism complete, 20-dihydrodydrogesterone (DHD) metabolite Half-life dydrogesterone (5-7 hours) & DHD (14-17 hours) Excretion urine Identifiers CAS number 152-62-5 
ATC code G03DB01 PubChem CID 9051 DrugBank APRD00941 ChemSpider 8699 UNII 90I02KLE8K KEGG D01217 ChEBI CHEBI:31527 ChEMBL CHEMBL1200853 
Chemical data Formula C21H28O2 Mol. mass 312.446 g/mol SMILES eMolecules & PubChem - InChI=1S/C21H28O2/c1-13(22)17-6-7-18-16-5-4-14-12-15(23)8-10-20(14,2)19(16)9-11-21(17,18)3/h4-5,12,16-19H,6-11H2,1-3H3/t16-,17+,18-,19+,20+,21+/m0/s1
Key:JGMOKGBVKVMRFX-HQZYFCCVSA-N
 (what is this?) (verify)
(what is this?) (verify)Dydrogesterone is a progestogen hormone. The brand name is Duphaston and manufactured by Abbott (formerly Solvay Pharmaceuticals).
Dydrogesterone was first introduced to the market in 1961, and is currently approved in over 100 countries worldwide. It has an estimated cumulative exposure of more than 28 million patients.
Dydrogesterone is a potent, orally active progestogen indicated in a wide variety of gynaecological conditions. Although similar in molecular structure and pharmacological effects to endogenous progesterone. It is orally active at far lower doses. Its freedom from oestrogenic, androgenic, anabolic, corticoid and other undesirable hormonal effects gives it additional benefits over most other synthetic progestogens. The therapeutic use of dydrogesterone is closely related to its physiological action on the neuro-endocrine control of ovarian function, as well as on the endometrium. As such, it is indicated in all cases of relative or absolute endogeneous progesterone deficiency.
Dydrogesterone has proven effective in the following conditions:[citation needed]
- menstrual disorders
- infertility
- threatened and habitual abortion. Dydrogesterone is not approved for this indication by any regulatory body in US, Canada, EU or Australia.
- endometriosis
- premenstrual syndrome
Dydrogesterone has also been registered as hormone replacement therapy (HRT) to counteract the negative effects of unopposed oestrogen on the endometrium. Dydrogesterone is relatively safe and well-tolerated, and does not exhibit the androgenic side effects that are common with some other progestins, like medroxyprogesterone.
Contents
Indications
Dydrogesterone In Menstrual Disorders
Dysmenorrhoea Primary or essential dysmenorrhoea is one of the most common gynaecological complaints of women during their reproductive years. Dydrogesterone relieves the pain associated with incapacitating dysmenorrhoea, decreases the need for analgesics and reduces absenteeism from work.
Secondary amenorrhoea Secondary amenorrhoea is a symptom rather than a specific disease. Dydrogesterone adequately induces bleeding when the endometrium is sufficiently primed with oestrogens. When oestradiol levels are low, dydrogesterone treatment should be supplemented with oestrogens.
Dysfunctional uterine bleeding and irregular cycles Of the wide range of medications used to reduce heavy menstrual bleeding in patients with ovulatory cycles, oral progestogens like dydrogesterone are the most commonly prescribed. It prevents heavy bleeding.
Dydrogesterone in Infertility and Threatened and Habitual Abortion
Luteal insufficiency Luteal insufficiency leads to inadequate ovarian progesterone production, which in turn results in an incomplete secretory endometrium and ineffective ovum implantation. Dydrogesterone almost doubles pregnancy rates compared to placebo.
Threatened and habitual abortion The incidence of spontaneous abortion is about 15% of all clinically recognised pregnancies. Progestogens are commonly used in threatened and habitual abortion. They are thought to exert their effect in two ways. Firstly, by restoring luteal function, thereby decreasing the incidence of first trimester abortions. Secondly, through relaxation of the smooth musculature of the uterus. More recently, the evidence indicates that modulation of the maternal immune response during early pregnancy also contributes to the anti-abortive effects of dydrogesterone. In clinical practise, dydrogesterone achieved success rates of 70% or higher.[citation needed] Dydrogesterone is not approved for this indication by any regulatory body in US, Canada, EU or Australia.
Dydrogesterone is recommended in the treatment of infertility for several reasons:
- it has no inhibitory effect on ovulation
- it does not alter the normal pattern of secretory transformation of the endometrium
- it does not inhibit the formation of progesterone in the human placenta during early pregnancy
- it does not cause masculinisation of the female foetus.
Dydrogesterone in Endometriosis
Endometriosis is a chronic disease which can cause severe, progressive, and at times, incapacitating dysmenorrhoea, pelvic pain, dyspareunia and infertility. Dydrogesterone relieves pain without inhibiting ovulation, so that patients are able to become pregnant during treatment. The efficacy of dydrogesterone on the lesions of endometriosis is less clear, but their number and severity does not seem to correlate with the severity of symptoms.
Dydrogesterone in Premenstrual Syndrome
Premenstrual syndrome (PMS) is characterised by a range of mood swings and physical symptoms.
Dydrogesterone effectively relieves a number of these and is especially indicated when:
- PMS is associated with hypermenorrhoea and dysmenorrhoea
- other treatments such as oral contraceptives for ovulation suppression, or psychotropic medication are contraindicated.
Dydrogesterone in Hormone Replacement Therapy
The principle behind HRT is twofold:
- to actively increase the circulating levels of oestrogens to control hot flushes
- to prevent the long-term effects of the menopause, such as bone resorption and unfavourable changes in blood lipids
The administration of 17β-oestradiol halts, or reverses atrophic changes that occur due to the loss of endogenous oestradiol during the menopause.
Oestrogens stimulate the growth of endometrial cells. In postmenopausal women with an intact uterus, oestrogen monotherapy results in continued endometrial proliferation without the physiological secretory transformation normally induced by progesterone. This process is associated with an increased incidence of endometrial hyperplasia and carcinoma. Additional protection with progestogens is therefore mandatory in patients with an intact uterus who receive oestrogen replacement therapy.
Dydrogesterone opposes the proliferative effect of oestrogens on the endometrium and ensures conversion to a secretory pattern and cyclical shedding of the endometrium in sequential HRT regimens. As such dydrogesterone effectively guards against the development of endometrial hyperplasia. Unlike androgenic progestogens, dydrogesterone does not reverse the beneficial effects of 17β-oestradiol on lipid profiles and carbohydrate metabolism. This make it a progestogen of choice, as illustrated by its excellent cycle control in sequential combined HRT. In a continuous combined HRT regimen, dydrogesterone inhibits the proliferation of the endometrium so that it remains atrophic or inactive. The majority of patients become amenorhhoeic after 6 months of treatment.
Chemistry
Dydrogesterone (9β,10α-pregna-4,6-diene-3,20-dione) was first synthesised by Duphar in the 1950s. Although its molecular structure is almost identical to that of natural progesterone, its unique design makes it a potent, orally active progestogen. In the dydrogesterone molecule, the hydrogen atom at carbon 9 is in the beta position and the methyl group at carbon 10 is in the alpha position - a reverse of the progesterone structure, hence the term 'retro' progesterone. Furthermore, it has a second double bond between carbon 6 and carbon 7 (the 4, 6-diene-3-one configuration). These small differences in chemical structure account for the improved oral activitity, metabolic stability, and the lack of oestrogenic, androgenic and mineralo-corticoid properties of dydrogesterone.
Pharmacokinetics
Dydrogesterone is readily absorbed after oral administration. Tmax values vary between 0.5 and 2.5 hours.
Metabolisation of dydrogesterone is virtually complete. The main metabolic reaction is hydrogenation of the 20-keto group, resulting in 20-dihydrodydrogesterone (DHD), another potent progestogen. The levels of the main active metabolite DHD also peak about 1.5 hours after dosing.
After oral administration, plasma concentrations of DHD are substantially higher than those of the parent drug. The ratios of DHD/Dydrogesterone for AUC and Cmax are in the order of 40 and 25, respectively. Absolute bio-availability is on average 28%.
All the metabolites of dydrogesterone retain the 4, 6-diene-3-one structure, and are metabolically stable. As such, dydrogesterone does not undergo aromatisation, which is consistent with its absence of oestrogenic effects. Furthermore, dydrogesterone does not undergo 17α-hydroxylation, which explains its lack of androgenic effects.
Dydrogesterone has predictable pharmacokinetics. The single-dose kinetics are linear in the oral dose range of 5–20 mg. The pharmacokinetics do not change during repeated administration of up to 20 mg dydrogesterone once daily. Steady state is attained after 3 days of treatment.
Dydrogesterone and its metabolites are excreted predominantly in urine. About 85% of an oral dose is excreted within 24 hours. The mean terminal half-lives od dydrogesterone and DHD vary between 5-7 and 14–17 hours, respectively.
In HRT, dydrogesterone is administered together with an oestrogen. Therefore, the interaction between dydrogesterone and oestrogens has been assessed, and no clinically significant interaction has been observed.
Pharmacology
When administered orally Dydrogesterone has advantageous pharmacological properties compared to endogenous progesterone:
- It is orally active at low dosages.
- It has selective progestogenic properties without any traditional hormonal activity.
- The amount absorbed is more predictable than for progesterone, since it is not broken down as easily when passing through the digestive system.
Dydrogesterone is characterised by progestational and anti-oestrogenic activity. This is demonstrated by its ability to induce a secretory transformation in the endometrium of immature or ovariectomised animals after they have been primed with oestrogens (cf. the Clauberg test). The oral progestogenic potency of dydrogesterone is 20 times higher than that of progesterone. The progestational efficacy and potency of dydrogesterone was confirmed by standard test (i.e. delay of menses and induction of withdrawal bleeding). The benefits of oestrogen or other target organs are not compromised by dydrogesterone.
Unlike other synthetic progestogens, dydrogesterone is not chemically related to testosterone. Its low affinity for the androgen receptor explains why it has no unwanted androgenic or anti-androgenic effects even at high doses and after prolonged treatment:
- no virilisation (acne, voice changes, hirsutism) of the adult female
- no virilising effects on the genital tract of the female foetus
- no effect on the fertility of the offspring.
Dydrogesterone is not converted into oestrogen, and has no adverse oestrogenic effects on fertility or sexual development.
At recommended doses, dydrogesterone has no effect on ovulation in healthy women:
- the biphasic pattern of the basal body temperature is maintained
- normal ovulatory rise in oestrogen and pregnanediol
- normal premenstrual biopsy
- no modification of vaginal cytology
- cytological evidence of ovulation
- the formation of the corpus luteum has been confirmed by laparotomy
These beneficial results are of particular relevance to the use of dydrogesterone in women who wish to become pregnant.
Dydrogesterone is free from adverse effects on carbohydrate metabolism. It does not cause changes in body weight, blood pressure, glucose tolerance or blood lipid ratios. No significant effects on blood coagulation or liver function tests have been reported. These favourable results are crucial in long-term therapy, e.g. postmenopausal HRT.
Toxicology
No serious or unexpected toxicity has been observed with dydrogesterone. In acute toxicity studies, the LD50 doses in rats exceeded 4,640 mg/kg for the oral route.
There was no evidence of mutagenic potential in the Ames test.
Adverse Reactions and Side effects
Like all hormonal medications Dydrogesterone can have side effects. These may include:
Breakthrough bleeding (increase dose), altered liver function with asthenia or malaise, jaundice & abdominal pain. Allergic rash, pruritus, urticaria, oedema, angioedema, haemolytic anaemia.
The use of progestins, in particular medroxyprogesterone, in treating post-menopausal symptoms have been associated with increased risk of blood clots and breast cancer in a study carried out by the Women's Health Initiative. While the study did not study dydrogesterone, it is possible, but not certain, that it too increases these risks.
Estrogens and progestogens (G03C-D, L02) Progestogens/
progestins
(progesterone)AgonistAndrostene (Drospirenone) • 19-norprogesterone (Nomegestrol • Promegestone • Trimegestone) • 19-nortestosterone (Dienogest)Other/
ungroupedPregnenedione (Gestonorone) • Pregnene (Ethisterone) • Pregnadiene (Medrogestone • Melengestrol) • Norpregnane (Norgestrienone) • Lynestrenol • Norethynodrel • Tibolone • Dydrogesterone • Quingestanolantagonist: MifepristoneAsoprisnil • CDB-4124 • Ulipristal acetateEstrogens AgonistDiosgenin • Estradiol (Ethinylestradiol#/Mestranol • Estradiol 17 beta-cypionate# • Polyestradiol phosphate) • Estrone (Estrone sulfate) • Estriol • Promestriene • Equilenin • EquilinAfimoxifene • Arzoxifene • Bazedoxifene • Cyclofenil • Lasofoxifene • Ormeloxifene • Raloxifene • Tamoxifen • Toremifenepure antagonist: FulvestrantCategories:- Progestagens
- InChI=1S/C21H28O2/c1-13(22)17-6-7-18-16-5-4-14-12-15(23)8-10-20(14,2)19(16)9-11-21(17,18)3/h4-5,12,16-19H,6-11H2,1-3H3/t16-,17+,18-,19+,20+,21+/m0/s1
Wikimedia Foundation. 2010.