- Cat scratch disease
-
Cat Scratch Disease Classification and external resources 
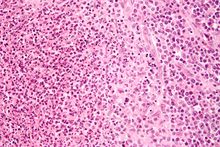
Micrograph of a lymph node affected by cat scratch disease. H&E stain.ICD-10 A28.1 ICD-9 078.3 DiseasesDB 2173 eMedicine emerg/84 MeSH D002372 Cat scratch disease (CSD) (also known as "Cat scratch fever",[1] "Inoculation lymphoreticulosis",[1] and "Subacute regional lymphadenitis"[1]) is a usually benign infectious disease caused by the intracellular bacterium Bartonella. It is most commonly found in children following a scratch or bite from a cat by about one to two weeks. It was first discovered in 1889 by Henri Parinaud.[2]
Contents
Transmission
The cat was recognized as the natural reservoir of the disease in 1950 by Dr. Robert Debré.[3][4] Judy Dolan was the first person to be diagnosed with the disease in the United States of America.
The causative organism was first thought to be Afipia felis, but this was disproved by immunological studies demonstrating that cat scratch fever patients developed antibodies to two other organisms, Bartonella henselae (B. henselae) and Bartonella clarridgeiae, which are rod-shaped Gram-negative bacteria.
Kittens are more likely to carry the bacteria in their blood, and may therefore be more likely to transmit the disease rather than an adult cats. However, the results of experimental studies showed that fleas serve as a vector for transmission of B. henselae among cats,[5] and that viable B. henselae are excreted in the feces of Ctenocephalides felis, the cat flea.[6] Another study showed that cats could be infected with B. henselae through intradermal inoculation using flea feces containing B. henselae.[7] As a consequence, it is believed that a likely means of transmission of B. henselae from cats to humans may be inoculation with flea feces containing B. henselae through a contaminated cat scratch wound or across a mucosal surface. Although Bartonella DNA has been reported in ticks, there is no evidence that CSD can be transmitted by tick bites.[8]Other names
The condition has also been termed Cat-Scratch Adenitis, Cat-Scratch-Oculoglandular Syndrome, Debre's Syndrome, Debre-Mollaret Syndrome, Foshay-Mollaret Cat Scratch Fever, Foshay-Mollaret syndrome, Foshay-Mollaret Cat-Scratch Fever Syndrome, Lymphadenitis-Regional Non-bacterial, Lymphoreticulosis-Benign Inoculation, maladie des griffes du chat, Parinaud oculoglandular disease, and Petzetakis' disease.[citation needed]
Signs and symptoms
Manifestations of cat scratch disease can be divided into classic and atypical.
Classic cat scratch disease presents as tender and swollen regional lymph nodes, a condition referred to as regional lymphadenopathy. There may be a papule at the site of initial infection. While some patients have fever and other systemic symptoms, many do not. Other associated complaints include headache, chills, backache and abdominal pain. It may take 7 to 14 days, or as long as two months, before symptoms appear. Most cases are benign and self-limiting, but lymphadenopathy may persist for several months after other symptoms disappear. In general, the prognosis is favorable. In temperate climates, most cases occur in fall and winter. The disease usually resolves spontaneously, with or without treatment, in one month. In immunocompromised patients more severe complications sometimes occur.
Atypical cat scratch disease takes several different forms depending on organ systems involved. Atypical forms of disease are becoming increasingly recognized in clinical practice.
Parinaud's oculoglandular syndrome is a granulomatous conjunctivitis with concurrent swelling of the lymph node near the ear.
Optic neuritis, involvement of the retina, and neuropathy can also occur.
Bacillary angiomatosis is caused by Bartonella henselae, the causative organism of cat scratch disease. It is primarily a vascular skin lesion that may extend to bone or be present in other areas of the body. In the typical scenario, the patient has HIV or another cause of severe immune dysfunction.
Bacillary peliosis is a condition that most-often affects patients with HIV and other conditions causing severe immune compromise. The liver and spleen are primarily affected, with findings of blood-filled cystic spaces on pathology [9]
Acute encephalopathy (generalized dysfunction of the brain) can occur. The New York Times Magazine described a case, presenting as a meningitis, with fever, headache, and impaired vision (due to swelling of the optic nerves).[10] Despite the severity of initial presentation, patient outcome can be favorable.
Enlarged spleen and sore throat can also occur in rare cases [11]
Pathology
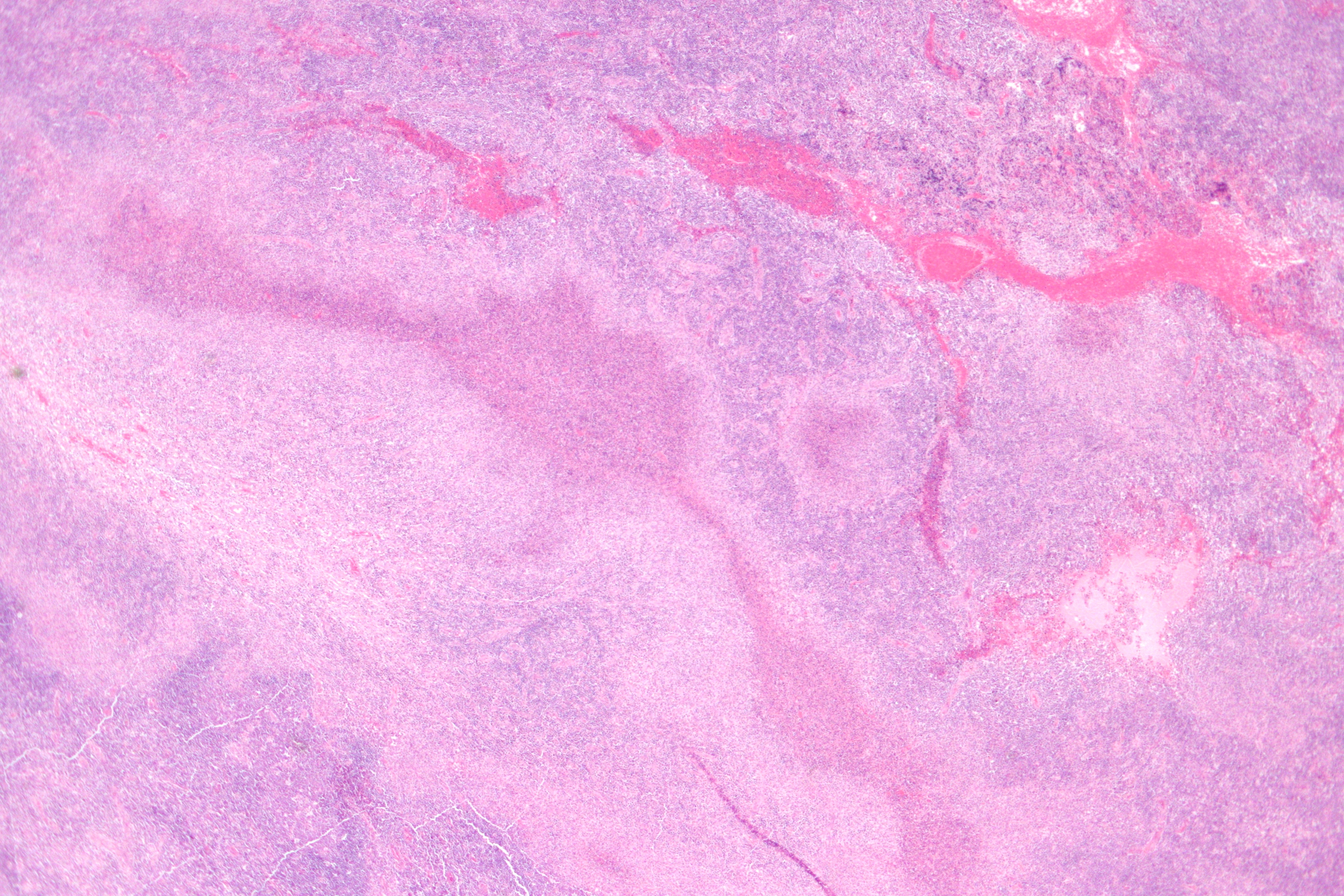
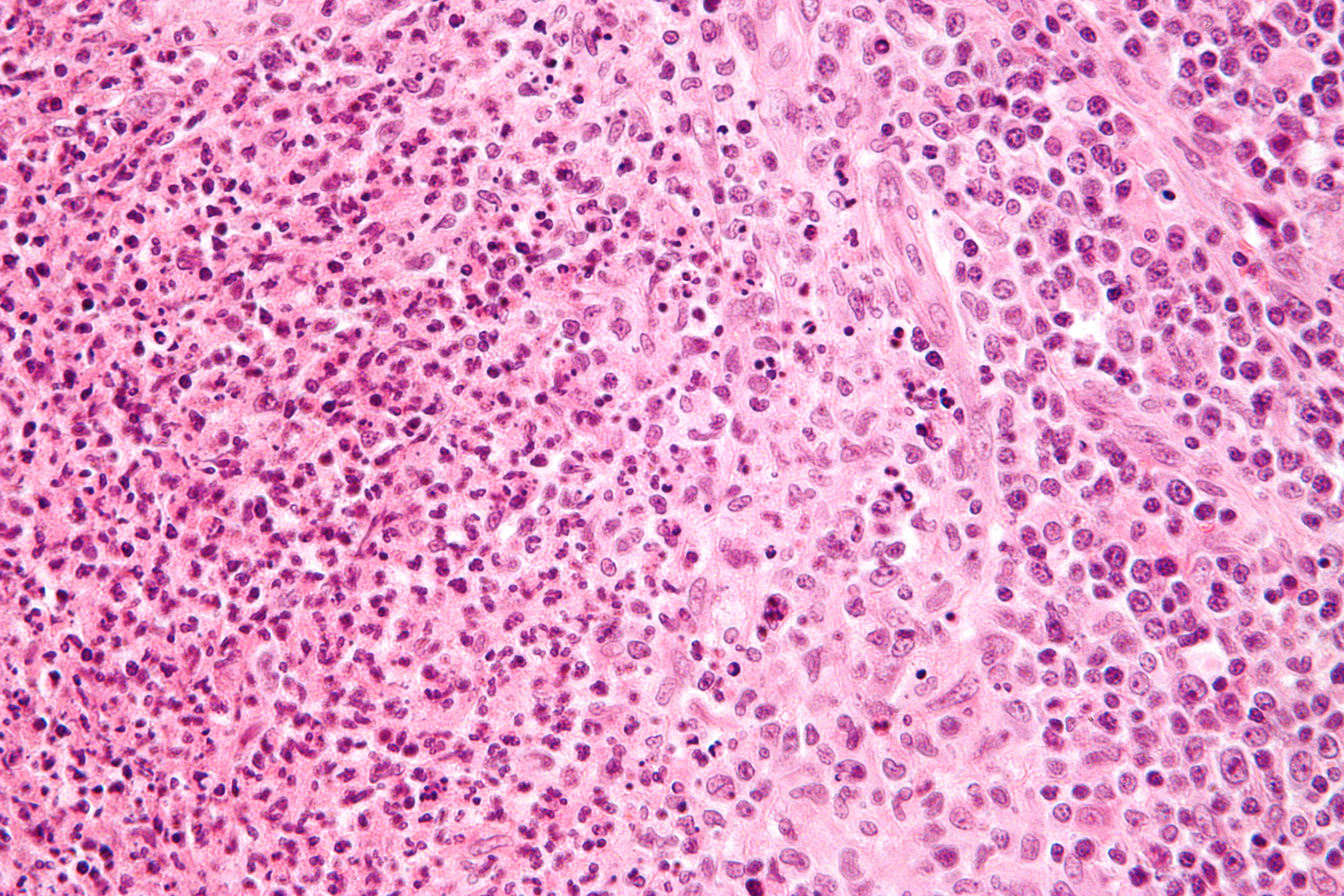
 High magnification micrograph of cat scratch disease showing a granuloma (pale cells - right of center on image) and a microabscess with neutrophils (left of image). H&E stain.
High magnification micrograph of cat scratch disease showing a granuloma (pale cells - right of center on image) and a microabscess with neutrophils (left of image). H&E stain.
The primary cutaneous lesion consists of a red papule at site of inoculation, 1–2 weeks after contact, which may become pustular or crusted, which is accompanied by enlargement of regional – usually the cervical and axiallary – lymph nodes. Under the microscope, the skin lesion demonstrates a circumscribed focus of necrosis, surround by histiocytes, often accompanied by multinucleated giant cells, lymphocytes, and eosinophils. The regional lymph nodes demonstrate follicular hyperplasia with central stellate necrosis with neutrophils, surrounded by palisading histiocytes (suppurative granulomas) and sinuses packed with monocytoid B cells, usually without perifollicular and intrafollicular epithelioid cells
Treatment
The Warthin–Starry stain is used to confirm the presence of B. henselæ.
Azithromycin, ciprofloxacin, doxycycline, and multiple other antibiotics have been used successfully.[citation needed]
Azithromycin is especially used in pregnancy, to avoid the side-effects of doxycycline.
See also
References
- ^ a b c Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- ^ Jerris RC, Regnery RL (1996). "Will the real agent of cat-scratch disease please stand up?". Annu. Rev. Microbiol. 50: 707–25. doi:10.1146/annurev.micro.50.1.707. PMID 8905096.
- ^ Chomel BB (2000). "Cat-scratch disease". Rev. - Off. Int. Epizoot. 19 (1): 136–50. PMID 11189710.
- ^ Arlet G, Perol-Vauchez Y (1991). "The current status of cat-scratch disease: an update". Comp. Immunol. Microbiol. Infect. Dis. 14 (3): 223–8. doi:10.1016/0147-9571(91)90002-U. PMID 1959317.
- ^ Chomel BB, Kasten RW, Floyd-Hawkins K et al. (August 1996). "Experimental transmission of Bartonella henselae by the cat flea". J. Clin. Microbiol. 34 (8): 1952–6. PMC 229161. PMID 8818889. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=229161.
- ^ Higgins JA, Radulovic S, Jaworski DC, Azad AF (May 1996). "Acquisition of the cat scratch disease agent Bartonella henselae by cat fleas (Siphonaptera:Pulicidae)". J. Med. Entomol. 33 (3): 490–5. PMID 8667399.
- ^ Foil L, Andress E, Freeland RL et al. (September 1998). "Experimental infection of domestic cats with Bartonella henselae by inoculation of Ctenocephalides felis (Siphonaptera: Pulicidae) feces". J. Med. Entomol. 35 (5): 625–8. PMID 9775583.
- ^ Telford SR III, Wormser GP (March 2010). "Bartonella spp. transmission by ticks not established". Emerg Infect Dis 16 (3): 379–84. doi:10.3201/eid1603.090443. PMID 20202410.
- ^ Perkocha LA, Geaghan SM, Yen TS et al. (December 1990). "Clinical and pathological features of bacillary peliosis hepatis in association with human immunodeficiency virus infection". N. Engl. J. Med. 323 (23): 1581–6. doi:10.1056/NEJM199012063232302. PMID 2233946.
- ^ Sanders, L."Vision Quest", "The New York Times", 4/10/2009.
- ^ NLM.NIH.gov [1] Medline
External links
- CDC information
- DermNet bacterial/catscratch
- Cat Scratch Disease on National Organization for Rare Disorders site
- Cat Scratch Fever Disease
- Cat Scratch Fever
Categories:- Zoonotic bacterial diseases
- Bacterium-related cutaneous conditions
- Zoonoses
Wikimedia Foundation. 2010.