- Uterine fibroid
-
Uterine fibroids Classification and external resources 
Uterine FibroidsICD-10 D25 ICD-9 218.9 OMIM 150699 DiseasesDB 4806 eMedicine radio/777 MeSH D007889 A uterine fibroid (also uterine leiomyoma,[1] myoma, fibromyoma, leiofibromyoma, fibroleiomyoma, and fibroma) (the plural of myoma is myomas or myomata) is a benign (non-cancerous) tumor that originates from the smooth muscle layer (myometrium) and the accompanying connective tissue of the uterus.
Fibroids are the most common benign tumors in females and typically found during the middle and later reproductive years. While most fibroids are asymptomatic, they can grow and cause heavy and painful menstruation, painful sexual intercourse, and urinary frequency and urgency. Some fibroids may interfere with pregnancy although this appears to be very rare.[2]
In the US, symptoms caused by uterine fibroids are a very frequent indication for hysterectomy.[3] Fibroids are often multiple and if the uterus contains too many leiomyomata to count, it is referred to as diffuse uterine leiomyomatosis. The malignant version of a fibroid is extremely uncommon and termed a leiomyosarcoma.
Contents
Signs and symptoms
Fibroids, particularly when small, may be entirely asymptomatic. Symptoms depend on the location of the lesion and its size. Important symptoms include abnormal gynecologic hemorrhage, heavy or painful periods, abdominal discomfort or bloating, painful defecation, back ache, urinary frequency or retention, and in some cases, infertility.[4] There may also be pain during intercourse, depending on the location of the fibroid. During pregnancy they may be the cause of miscarriage, bleeding, premature labor, or interference with the position of the fetus.
The U.S. Department of Health & Human Services states that "Fibroids are almost always benign (not cancerous). Rarely (less than one in 1,000) a cancerous fibroid will occur. This is called leiomyosarcoma. Doctors think that these cancers do not arise from an already-existing fibroid. Having fibroids does not increase the risk of developing a cancerous fibroid. Having fibroids also does not increase a woman's chances of getting other forms of cancer in the uterus."[5]
While fibroids are common, they are not a typical cause for infertility accounting for about 3% of reasons why a woman may not have a child.[6] Typically in such cases a fibroid is located in a submucosal position and it is thought that this location may interfere with the function of the lining and the ability of the embryo to implant.[6] Also larger fibroids may distort or block the fallopian tubes.
Pathophysiology
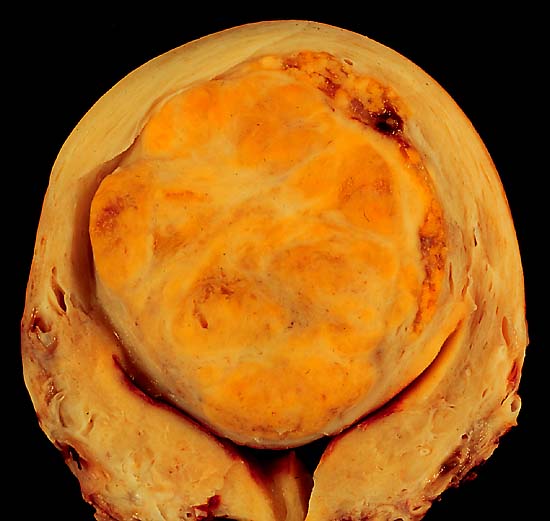
Leiomyomas grossly appear as round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and show whorled appearance on histological section. The size varies, from microscopic to lesions of considerable size. Typically lesions the size of a grapefruit or bigger are felt by the patient herself through the abdominal wall.

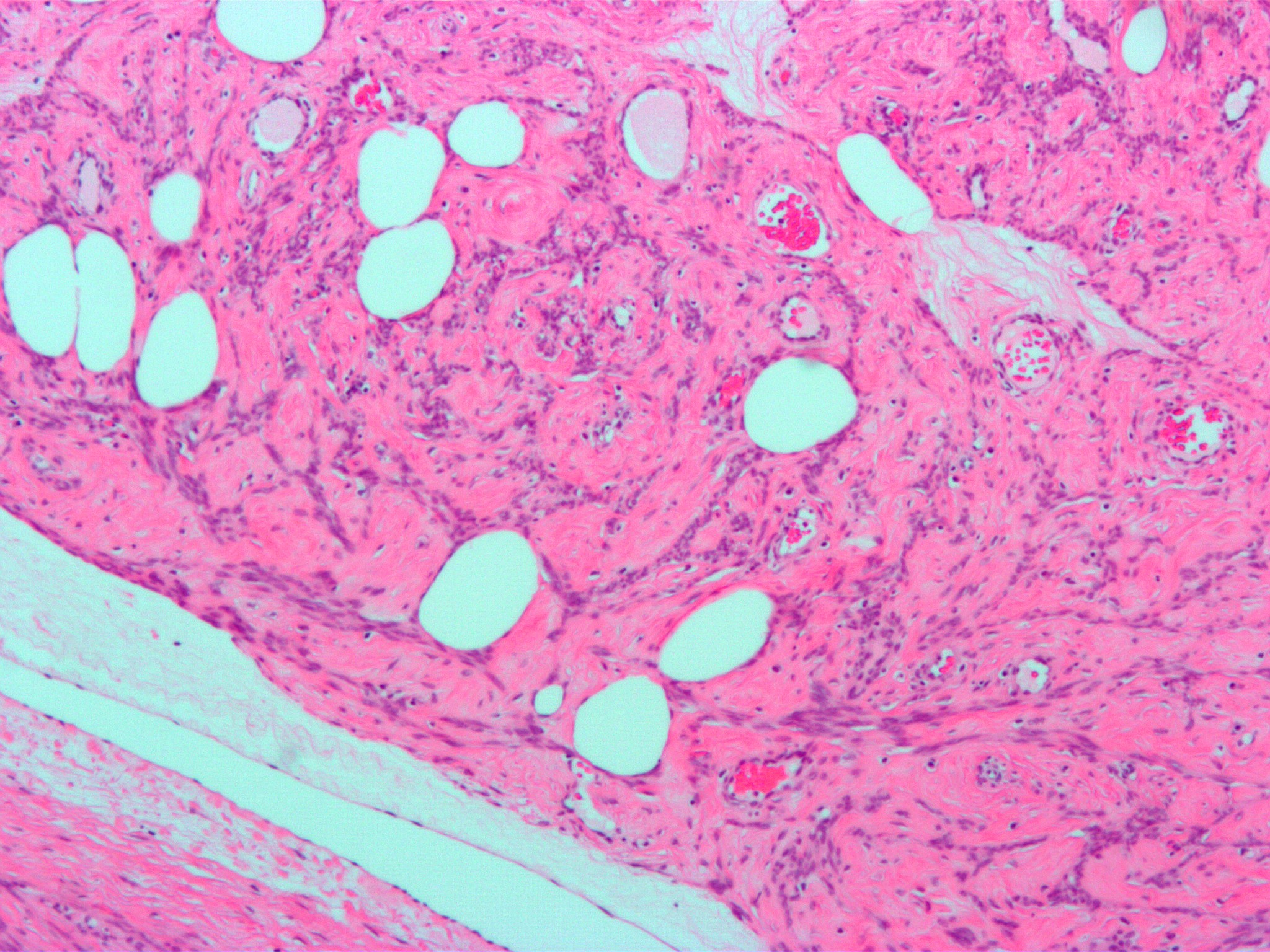
Microscopically, tumor cells resemble normal cells (elongated, spindle-shaped, with a cigar-shaped nucleus) and form bundles with different directions (whorled). These cells are uniform in size and shape, with scarce mitoses. There are three benign variants: bizarre (atypical); cellular; and mitotically active.
Location
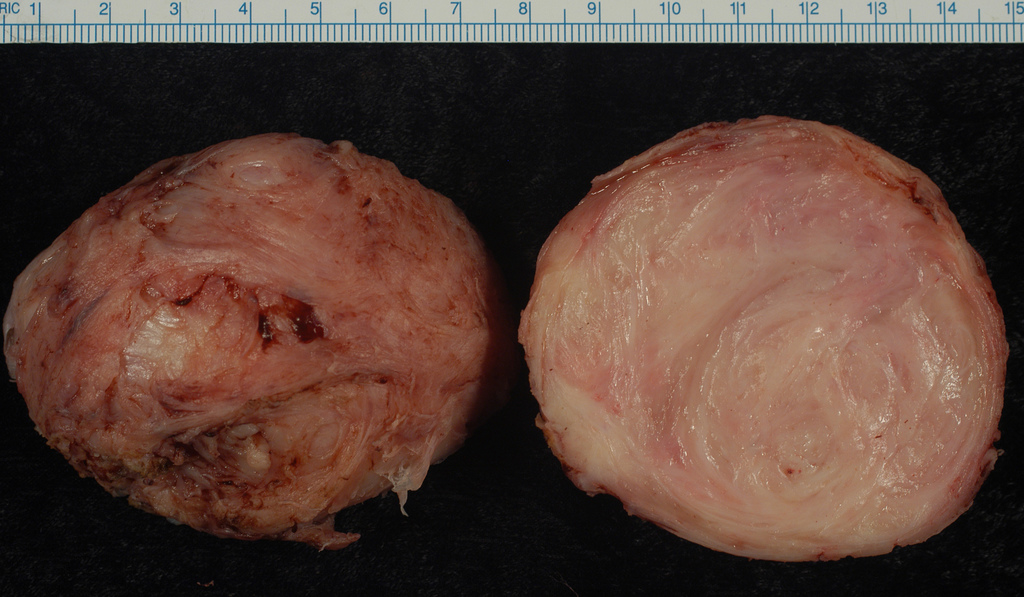
 An enucleated uterine leiomyoma – external surface on left, cut surface on right.
An enucleated uterine leiomyoma – external surface on left, cut surface on right.
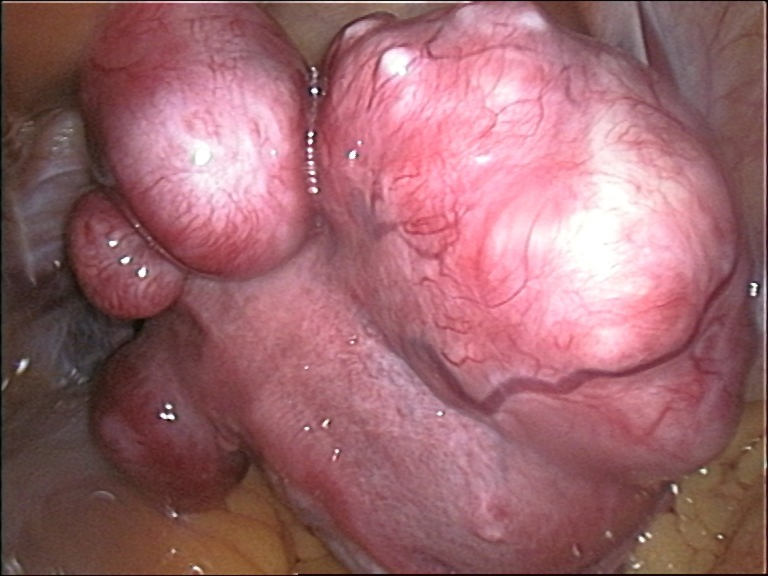
 large subserosal fibroid
large subserosal fibroidGrowth and location are the main factors that determine if a fibroid leads to symptoms and problems.[3] A small lesion can be symptomatic if located within the uterine cavity while a large lesion on the outside of the uterus may go unnoticed. Different locations are classified as follows:
- Intramural fibroids are located within the wall of the uterus and are the most common type; unless large, they may be asymptomatic. Intramural fibroids begin as small nodules in the muscular wall of the uterus. With time, intramural fibroids may expand inwards, causing distortion and elongation of the uterine cavity.
- Subserosal fibroids are located underneath the mucosal (peritoneal) surface of the uterus and can become very large. They can also grow out in a papillary manner to become pedunculated fibroids. These pedunculated growths can actually detach from the uterus to become a parasitic leiomyoma.
- Submucosal fibroids are located in the muscle beneath the endometrium of the uterus and distort the uterine cavity; even small lesion in this location may lead to bleeding and infertility. A pedunculated lesion within the cavity is termed an intracavitary fibroid and can be passed through the cervix.
- Cervical fibroids are located in the wall of the cervix (neck of the uterus). Rarely fibroids are found in the supporting structures (round ligament, broad ligament, or uterosacral ligament) of the uterus that also contain smooth muscle tissue.
Fibroids may be single or multiple. Most fibroids start in an intramural location, that is the layer of the muscle of the uterus. With further growth, some lesions may develop towards the outside of the uterus or towards the internal cavity. Secondary changes that may develop within fibroids are hemorrhage, necrosis, calcification, and cystic changes.
Pathogenesis
Fibroids are monoclonal tumors, approximately 40 to 50% show karyotypically detectable chromosomal abnormalities. When multiple fibroids are present they frequently have unrelated genetic defects. Specific mutations of the MED12 protein, have been noted in 70 percent of fibroids.[7]
Exact aetiology is not clearly understood, current working hypothesis is that genetic predispositions, prenatal hormone exposure and the effects of hormones, growth factors and xenoestrogens cause fibroid growth. Known risk factors are African-American descent, nulliparity, obesity, polycystic ovary syndrome, diabetes and hypertension.[8]
Fibroid growth is strongly dependent on estrogen and progesterone. Although both estrogen and progesterone are usually regarded as growth promoting they will also cause growth restriction in some circumstances. Paradoxically fibroids will rarely grow during pregnancy despite very high steroid hormone levels and pregnancy appears to exert a certain protective effect.[2] This protective effect might be partially mediated by an interaction estrogen and the oxytocin receptor.[9]
It is believed that estrogen and progesterone have both mitogenic effect on leiomyoma cells and also act by influencing (directly and indirectly) a large number of growth factors, cytokines and apoptotic factors as well as other hormones. Furthermore the actions of estrogen and progesterone are modulated by the cross-talk between estrogen, progesterone and prolactin signalling which controls the expression of the respective nuclear receptors. It is believed that estrogen is growth promoting by up-regulating IGF-1, EGFR, TGF-beta1, TGF-beta3 and PDGF, promotes aberrant survival of leiomyoma cells by down-regulating p53, increasing expression of the anti-apoptotic factor PCP4 and antagonizing PPAR-gamma signalling. Progesterone is thought to promote the growth of leiomyoma through up-regulating EGF, TGF-beta1 and TGF-beta3, and the survival through up-regulating Bcl-2 expression and down-regulating TNF-alpha. Progesterone is believed to counteract growth by downregulating IGF-1.[10][11][12] Expression of transforming growth interacting factor (TGIF) is increased in leiomyoma compared with myometrium.[13] TGIF is a potential repressor of TGF-β pathways in myometrial cells.[13]
Whereas in premenopausal fibroids the ER-beta, ER-alpha and progesterone receptors are found overexpressed, in the rare postmenopausal fibroids only ER-beta was found significantly overexpressed.[14] Most studies found that polymorphisms in ER and PR gene encodings are not correlated with incidence of fibroids in Caucasian populations[15][16] however a special ER-alpha genotype was found correlated with incidence and size of fibroids. The higher prevalence of this genotype in black women may also explain the high incidence of fibroids in this group.[17]
Uterine leiomyoma was more sensitive than normal myometrium to PPAR-gamma receptor activation resulting in reduced survival and apoptosis of leiomyoma cells. The mechanism is thought to involve negative cross-talk between ER and PPAR signaling pathways. Several PPAR-gamma ligands were considered as potential treatment.[18] PPAR-gamma agonists may also counteract leiomyoma growth by several other mechanisms of action such as TGF-beta3 expression inhibition.[19]
Hypertension is significantly correlated with fibroids. Although a causal relationships is not at all clear the hypothesis has been formulated that atherosclerotic injury to uterine blood vessels and the resulting inflammatory state may play a role. Furthermore endocrine factors related to blood pressure such as angiotensin II are suspected to cause fibroid proliferation via angiotensin II type 1 receptor.[20][21]
Aromatase and 17beta-hydroxysteroid dehydrogenase are aberrantly expressed in fibroids, indicating that fibroids can convert circulating androstenedione into estradiol.[22] Similar mechanism of action has been elucidated in endometriosis and other endometrial diseases.[23] Aromatase inhibotors are currently considered for treatment, at certain doses they would completely inhibit estrogen production in the fibroid while not largely affecting ovarian production of estrogen (and thus systemic levels of it). Aromatase overexpression is particularly pronounced in Afro-American women[24]
Genetic and hereditary causes are being considered and several epidemiologic findings indicate considerable genetic influence especially for early onset cases. First degree relatives have a 2.5-fold risk, and nearly 6-fold risk when considering early onset cases. Monozygotic twins have double concordance rate for hysterectomy compared to dizygotic twins.[25]
Like keloids, fibroids have disregulated production of extracellular matrix. Recent studies suggest that this production may represent an abnormal response to ischemic and mechanical tissue stress.[26] Several factors indicate significant involvement of extracellular signaling pathways such as ERK1 and ERK2, which in fibroids are prominently influenced by hormones.[27] Paradoxically and unlike most other conditions involving significant fibrosis the Cyr61 gene has been found downregulated in fibroids.[28]
Cyr61 is also known for its role as tumor suppressing factor and in angiogenesis. Hence fibroids are one of the very few tumors with reduced vascular density.[28]
Diagnosis
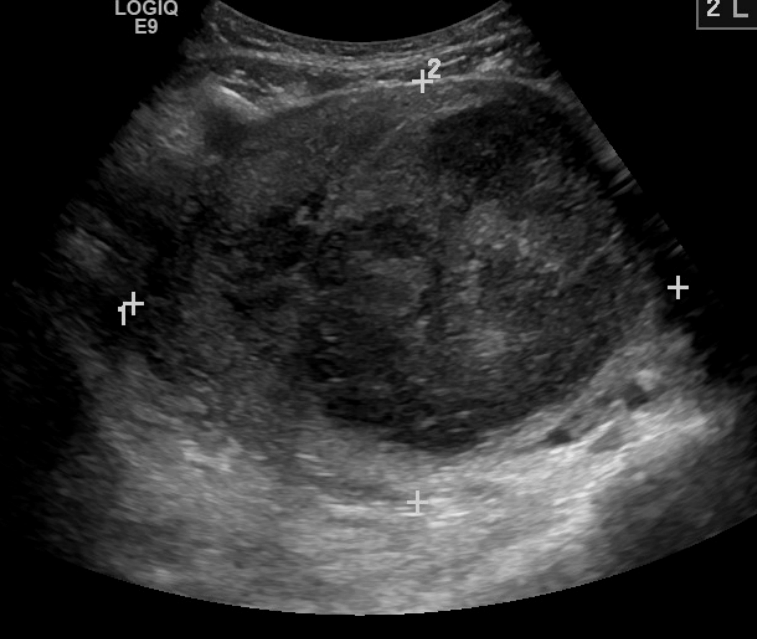
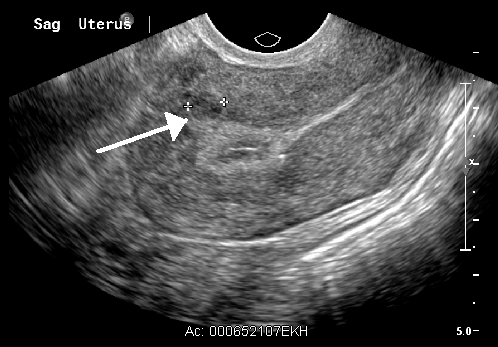
While a bimanual examination typically can identify the presence of larger fibroids, gynecologic ultrasonography (ultrasound) has evolved as the standard tool to evaluate the uterus for fibroids. Sonography will depict the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam. The location can be determined and dimensions of the lesion measured. Also magnetic resonance imaging (MRI) can be used to define the depiction of the size and location of the fibroids within the uterus.
Imaging modalities cannot clearly distinguish between the benign uterine leiomyoma and the malignant uterine leiomyosarcoma, however, the latter is quite rare. Fast growth or unexpected growth, such as enlargement of a lesion after menopause, raise the level of suspicion that the lesion might be a sarcoma. Also, with advanced malignant lesions there may be evidence of local invasion. A more recent study has suggested that diagnostic capabilities using MRI have improved the ability to detect sarcomatous lesions.[29] Biopsy is rarely performed and if performed, is rarely diagnostic. Should there be an uncertain diagnosis after ultrasounds and MRI imaging, surgery is generally indicated.
Other imaging techniques that may be helpful specifically in the evaluation of lesions that affect the uterine cavity are hysterosalpingography or sonohysterography.
-

A very large (9cm) fibroid of the uterus which is causing pelvic congestion syndrome as seen on CT
-

A very large (9cm) fibroid of the uterus which is causing pelvic congestion syndrome as seen on US]]
-

A relatively large submucosal leiomyoma; it fills out the major part of the endometrial cavity
-

A small uterine fibroid seen within the wall of the myometrium on a cross sectional ultrasound view
Coexisting disorders
Fibroids that lead to heavy vaginal bleeding lead to anemia and iron deficiency. Due to pressure effects gastrointestinal problems are possible such as constipation and bloatedness. Compression of the ureter may lead to hydronephrosis. Fibroids may also present alongside endometriosis, which itself may cause infertility. Adenomyosis may be mistaken for or coexist with fibroids.
In very rare cases, malignant (cancerous) growths, leiomyosarcoma, of the myometrium can develop.[30]
Treatment
Most fibroids do not require treatment unless they are causing symptoms. After menopause fibroids shrink and it is unusual for fibroids to cause problems.
Symptomatic uterine fibroids can be treated by:
- medication to control symptoms
- medication aimed at shrinking tumours
- ultrasound fibroid destruction
- various surgically aided methods to reduce blood supply of fibroids
- myomectomy or radio frequency ablation
- hysterectomy
- treatment for infection and anemia
- embolization
Medication
A number of medications are in use to control symptoms caused by fibroids. NSAIDs can be used to reduce painful menses. Oral contraceptive pills are prescribed to reduce uterine bleeding and cramps.[6] Anemia may have to be treated with iron supplementation.
Levonorgestrel intrauterine devices are highly effective in limiting menstrual blood flow. Side effects are typically very moderate because the levonorgestrel (a progestin) is released in low concentration locally. There is now substantial evidence that Levongestrel-IUDs provide good symptomatic relief for women with fibroids.[31] While most Levongestrel-IUD studies concentrated on treatment of women without fibroids a few reported very good results specifically for women with fibroids including a substantial regression of fibroids.[32] One reported problem is that women with large fibroids had more frequently spontaneous expulsion of the IUD, however many of those asked for reinsertion of the device indicating a high rate of satisfaction despite the expulsion.[33][34]
Danazol is an effective treatment to shrink fibroids and control symptoms. Its use is limited by unpleasant side effects. Mechanism of action is thought to be antiestrogenic effects. Recent experience indicates that safety and side effect profile can be improved by more cautious dosing.[33]
Dostinex in a moderate and well tolerated dosis has been shown in 2 studies to shrink fibroids effectively. Mechanism of action is completely unclear.[33][35]
Gonadotropin-releasing hormone analogs cause temporary regression of fibroids by decreasing estrogen levels. Because of the limitations and side effects of this medication it is rarely recommended other than for preoperative use to shrink the size of the fibroids and uterus before surgery. Its is typically used for a maximum of 6 months or shorter because after longer use they could cause osteoporosis and other typically postmenopausal complications. The main side effects are transient postmenopausal symptoms. In many cases the fibroids will regrow after cessation of treatment, however significant benefits may persists for much longer time in some cases. Several variations are possible, such as GnRH agonists with add-back regimens intended to decrease the adverse effects of estrogen deficiency. Several add-back regimes are possible, tibolone, raloxifene, progestogens alone, estrogen alone, and combined estrogens and progestogens.[33]
Aromatase inhibitors have been used experimentally to reduce fibroids. The effect is believed to be due partially by lowering systemic estrogen levels and partially by inhibiting locally overexpressed aromatase in fibroids.[33] Experience from experimental aromatase inhibitor treatment of endometriosis indicates that aromatase inhibitors might be particularly useful in combination with a progestogenic ovulation inhibitor.
Progesterone antagonists have been shown in small studies to decrease the size of uterine fibroids. Mifepristone was effective in a placebo-controlled pilot study.[36][37]Selective progesterone receptor modulators, such as Progenta, have been under investigation.
The selective progesterone receptor modulator Asoprisnil is currently tested with very promising results as a possible use as a treatment for fibroids - the hope is that it will provide the advantages of progesterone antangonitst without their adverse effects.[33]
The long term safety of progesterone antagonists as well as selective progesterone receptor modulators has yet to be established.[38][39]
Uterine artery embolization
Uterine artery embolization (UAE): Using interventional radiology techniques, the interventional radiologist occludes both uterine arteries, thus reducing blood supply to the fibroid.[40] This intervention is not usually recommended when fertility should be preserved although subsequent pregnancies are usually possible. A small catheter (1 mm in diameter) is inserted into the femoral artery at the level of the groin under local anesthesia. Under imaging guidance, the interventional radiologist will enter selectively into both uterine arteries and inject small (500 µm) particles that will block the blood supply to the fibroids. A patient will usually recover from the procedure within a few days. The UAE procedure should result in limited blood supply to the fibroids which should prevent them from further growth, heavy bleeding and possibly shrink them.
A retrospective cohort study showed that UAE has much fewer serious adverse effects than hysterectomy (odds ratio 0.25) and similar rates of satisfaction. In this study, 86% of women treated with UAE would recommend the treatment to a friend compared to 70% of those treated by hysterectomy.[41]
Uterine artery ligation
Uterine artery ligation, sometimes also laparoscopic occlusion of uterine arteries are minimally invasive methods to limit blood supply of the uterus by a small surgery that can be performed transvaginally or laparoscopically. The principal mechanism of action may be similar like in UAE. This is a relatively new[when?] method which demonstrated similar efficacy similar like UAE but is easier to perform and for this reason fewer side effects are expected.[42][43][44] UAE currently appears much more effective than this method in direct comparison.[45]
Radio frequency ablation
Radiofrequency ablation is one of the newest minimally invasive treatments for fibroids.[46] In this technique the fibroid is shrunk by inserting a needle-like device into the fibroid through the abdomen and heating it with radio-frequency (RF) electrical energy to cause necrosis of cells. The treatment is a potential option for women who have fibroids, have completed child-bearing and want to avoid a hysterectomy.
Myomectomy
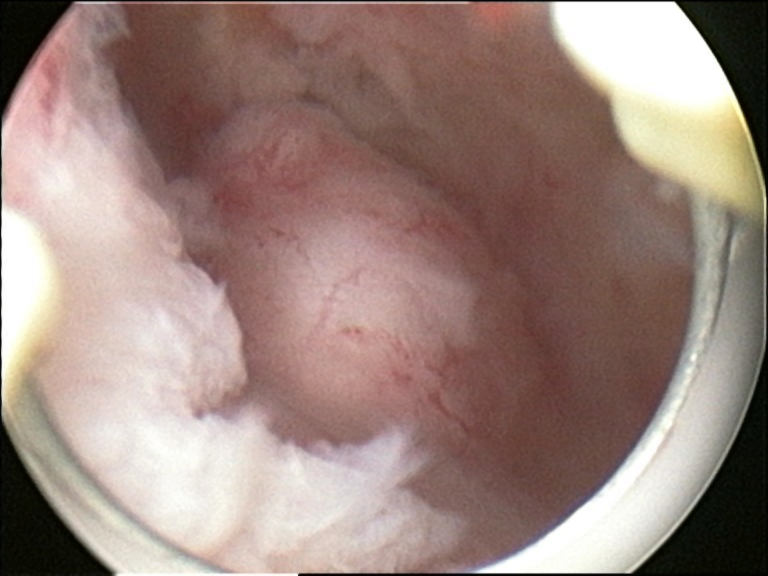
 submucosal fibroid in hysteroscopy
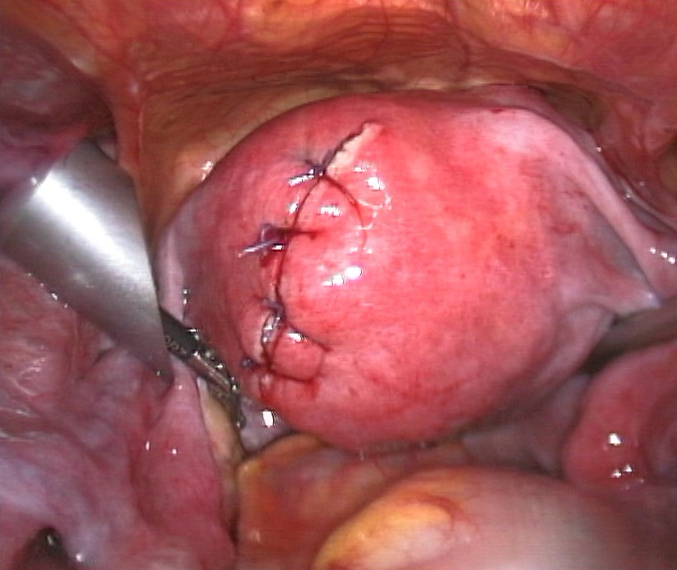
submucosal fibroid in hysteroscopy Treatment of an intramural fibroid by laparoscopic surgery
Treatment of an intramural fibroid by laparoscopic surgery After treatment of an intramural fibroid by laparoscopic surgery
After treatment of an intramural fibroid by laparoscopic surgeryMyomectomy is a surgery to remove one or more fibroids. It is usually recommended when more conservative treatment options fail for women who want fertility preserving surgery or who express desire to retain the uterus. This surgery is fertility preserving although in some circumstances subsequent pregnancies can be difficult or impossible.
There are three techniques types of myomectomy:
- In a hysteroscopic myomectomy, the fibroid is removed by the use of a resectoscope, an endoscopic instrument inserted through the vagina and cervix that can use high-frequency electrical energy to cut tissue. Hysteroscopic myomectomies can be done as an outpatient procedure, with either local or general anesthesia used. Hysteroscopic myomectomy is most often recommended for submucosal fibroids. A French study collected results from 235 patients suffering from submucous myomas who were treated with hysteroscopic myomectomies; in none of these cases was the fibroid greater than 5 cm.[47]
- A laparoscopic myomectomy requires a small incision near the navel. The physician then inserts a laparoscope into the uterus and uses surgical instruments to remove the fibroids. Studies have suggested that laparoscopic myomectomy leads to lower morbidity rates and faster recovery than does laparotomic myomectomy.[48] As with hysteroscopic myomectomy, laparoscopic myomectomy is not generally used on very large fibroids. A study of laparoscopic myomectomies conducted between January 1990 and October 1998 examined 106 cases of laparoscopic myomectomy, in which the fibroids were intramural or subserous and ranged in size from 3 to 10 cm.[49]
- A laparotomic myomectomy (also known as an open or abdominal myomectomy) is the most invasive surgical procedure to remove fibroids. The physician makes an incision in the abdominal wall and removes the fibroid from the uterus. A particularly extensive laparotomic procedure may necessitate that any future births be conducted by Caesarean section.[6] Recovery time from a laparatomic procedure is generally expected to be four to six weeks.
Hysterectomy
Hysterectomy is the classical method of treating fibroids. Although it is now recommended only as last option, fibroids are still the leading cause of hysterectomies in the US.
Endometrial ablation
Endometrial ablation can be used if the fibroids are only within the uterus and not intramural and relatively small. High failure and recurrence rates are expected in the presence of larger or intramural fibroids.
Magnetic resonance guided focused ultrasound
Magnetic Resonance guided Focused Ultrasound, is a non-invasive intervention (requiring no incision) that uses high intensity focused ultrasound waves to destroy tissue in combination with magnetic resonance imaging (MRI), which guides and monitors the treatment. During the procedure, delivery of focused ultrasound energy is guided and controlled using MR thermal imaging.[50] Patients who have symptomatic fibroids, who desire a non-invasive treatment option and who do not have contraindictions for MRI are candidates for MRgFUS. About 60% of patients qualify. It is an outpatient procedure and takes one to three hours depending on the size of the fibroids. It is safe and about 75% effective.[51] Symptomatic improvement is sustained for two plus years.[52] Need for additional treatment varies from 16-20% and is largely dependent on the amount of fibroid that can be safely ablated; the higher the ablated volume, the lower the re-treatment rate.[53] In comparison to available treatment options, the cost effectiveness of MRgFUS in the U.S. and U.K. has been found to be reasonable and comparable to alternative treatments (hysterectomy, pharmacotherapy, uterine artery embolization).[54][55] There are currently no randomized trial between MRgFUS and UAE. A multi-center trial is underway to investigate the efficacy of MRgFUS vs. UAE.
Epidemiology
About 20–40% of women will be diagnosed with leiomyoma but only a fraction of those will cause problems or require treatment.[3]
The condition is about twice as common in black women as white women.[56][57]
Leiomyoma are more common in obese women.[56] Fibroids are dependent on estrogen and progesterone to grow and therefore relevant only during the reproductive years, they are expected to shrink after menopause.
In African-Americans
Eighty percent of African-American women will develop benign uterine fibroid tumors by their late 40s, according to the National Institute of Environmental Health Sciences.[58] African American women are three times more likely to get fibroids than Caucasian women.[59] Also, in African-American women, fibroids also seem to occur at a younger age, grow more quickly, and are more likely to cause symptoms.[60] This leads to higher rates of surgery for African-Americans, both myomectomy and hysterectomy.[61] Furthermore, increased risk of fibroids in African- Americans causes them to fare worse in in-vitro fertility treatments and raises their risk of premature births and delivery by Cesarean section.[61]
Research has not proven why fibroids are more common in African American women but there are some speculations. Some studies suggest that black women who are obese and who have high blood pressure are more likely to have fibroids.[61] Additionally, national surveys show that black women consume fewer servings of dairy than white women and have lower intake of calcium, magnesium and phosphorus.[62] Boston University School of Medicine researchers found that increased dairy intake in African American woman decreases their risk of fibroids.[62] Additionally, research evidence has demonstrated that women with a family history of fibroids are twice more likely to develop fibroids than women with no family history- thus perpetuating the cycle of fibroid prevalence in African Americans.[61] However, although there is much speculation much more research must be done to determine why fibroid prevalence is higher in African American women.
Prognosis
About 1 out of 1000 lesions[6] are or become malignant, typically as a leiomyosarcoma on histology. A sign that a lesion may be malignant is growth after menopause.[6] There is no consensus among pathologists regarding the transformation of leiomyoma into a sarcoma. Most pathologists believe that a Leiomyosarcoma is a de novo disease[citation needed].
Metastasis
There are a number of rare conditions in which fibroids metastasize. They still grow in a benign fashion, but can be dangerous depending on their location.[63]
- In leiomyoma with vascular invasion, an ordinary-appearing fibroid invades into a vessel but there is no risk of recurrence.
- In Intravenous leiomyomatosis, leiomyomata grow in veins with uterine fibroids as their source. Cardiac involvement can be fatal.
- In benign metastasizing leiomyoma, leiomyomata grow in more distant sites such as the lungs and lymph nodes. The source is not entirely clear. Pulmonary involvement can be fatal.
- In disseminated intraperitoneal leiomyomatosis, leiomyomata grow diffusely on the peritoneal and omental surfaces, with uterine fibroids as their source. This can simulate a malignant tumor but behaves benignly.
Society and culture
The Center for Uterine Fibroids which is associated with Brigham and Women’s Hospital in Boston MA ([1]) is currently recruiting volunteers for an investigation of all aspects of the aetiology, pathology of fibroids and development of treatment options. This institution also has a lot of clinical trials focused on African American women. The focus of one study is the search for a specific gene associated with the development of fibroids. Since one risk factor for uterine fibroids is having a family history of fibroids, the results of this study will provide some answers on the heredity of the illness. Some women may interact with the healthcare system by getting an ultrasound to diagnosis symptoms if they’ve had a mother, sister or grandmother who has previously suffered with these benign tumors.
United States law
The 2005 S.1289 bill was read twice and referred to the committee on Health, Labor and Pensions but never passed for a Senate or House vote. The proposed Uterine Fibroid Research and Education Act of 2005 mentioned that $5 billion dollars is spent annually on hysterectomy surgeries each year, which affect 22% of African Americans and 7% of Caucasian women. The bill also called for more funding for research and educational purposes. It also states that of the $28 billion dollars issued to NIH[64], $5 million was allocated for uterine fibroids in 2004.
In other animals
Uterine fibroids are rare in animals, although they have been observed in certain dogs and Baltic gray seals.[65]
References
- ^ "uterine leiomyoma" at Dorland's Medical Dictionary
- ^ a b Neiger, R.; Sonek, J.; Croom, C.; Ventolini, G. (2006). "Pregnancy-related changes in the size of uterine leiomyomas". The Journal of reproductive medicine 51 (9): 671–674. PMID 17039693.
- ^ a b c Wallach EE, Vlahos NF (August 2004). "Uterine myomas: an overview of development, clinical features, and management". Obstet Gynecol 104 (2): 393–406. doi:10.1097/01.AOG.0000136079.62513.39. PMID 15292018.
- ^ Fibroid Tumors
- ^ http://www.4woman.gov/faq/uterine-fibroids.cfm#1
- ^ a b c d e f American Society of Reproductive Medicine Patient Booklet: Uterine Fibroids, 2003
- ^ Makinen, N.; Mehine, M.; Tolvanen, J.; Kaasinen, E.; Li, Y.; Lehtonen, H. J.; Gentile, M.; Yan, J. et al. (2011). "MED12, the Mediator Complex Subunit 12 Gene, is Mutated at High Frequency in Uterine Leiomyomas". Science. doi:10.1126/science.1208930. PMID 21868628.
- ^ Okolo, S. (2008). "Incidence, aetiology and epidemiology of uterine fibroids". Best practice & research. Clinical obstetrics & gynaecology 22 (4): 571–588. doi:10.1016/j.bpobgyn.2008.04.002. PMID 18534913.
- ^ Cesen-Cummings, K.; Houston, K.; Copland, J.; Moorman, V.; Walker, C.; Davis, B. (2003). "Uterine leiomyomas express myometrial contractile-associated proteins involved in pregnancy-related hormone signaling". Journal of the Society for Gynecologic Investigation 10 (1): 11–20. doi:10.1016/S1071-5576(02)00191-0. PMID 12517588.
- ^ Rein, MS (2000). "Advances in uterine leiomyoma research: the progesterone hypothesis". Environmental health perspectives 108 Suppl 5: 791–3. PMID 11035984.
- ^ Maruo, T.; Ohara, N.; Wang, J.; Matsuo, H. (2004). "Sex steroidal regulation of uterine leiomyoma growth and apoptosis". Human reproduction update 10 (3): 207–220. doi:10.1093/humupd/dmh019. PMID 15140868.
- ^ Wei, T.; Geiser, A.; Qian, H.; Su, C.; Helvering, L.; Kulkarini, N.; Shou, J.; N'cho, M. et al. (2007). "DNA microarray data integration by ortholog gene analysis reveals potential molecular mechanisms of estrogen-dependent growth of human uterine fibroids". BMC women's health 7: 5. doi:10.1186/1472-6874-7-5. PMC 1852551. PMID 17407572. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1852551.
- ^ a b Yen-Ping Ho J, Man WC, Wen Y, Polan ML, Shih-Chu Ho E, Chen B (June 2009). "Transforming growth interacting factor expression in leiomyoma compared with myometrium". Fertil. Steril. 94 (3): 1078–83. doi:10.1016/j.fertnstert.2009.05.001. PMC 2888713. PMID 19524896. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2888713.
- ^ Strissel, P.; Swiatek, J.; Oppelt, P.; Renner, S.; Beckmann, M.; Strick, R. (2007). "Transcriptional analysis of steroid hormone receptors in smooth muscle uterine leiomyoma tumors of postmenopausal patients". The Journal of steroid biochemistry and molecular biology 107 (1-2): 42–47. doi:10.1016/j.jsbmb.2007.02.005. PMID 17646097.
- ^ Massart, F.; Becherini, L.; Marini, F.; Noci, I.; Piciocchi, L.; Del Monte, F.; Masi, L.; Falchetti, A. et al. (2003). "Analysis of estrogen receptor (ERalpha and ERbeta) and progesterone receptor (PR) polymorphisms in uterine leiomyomas". Medical science monitor : international medical journal of experimental and clinical research 9 (1): BR25–BR30. PMID 12552233.
- ^ Fischer, C.; Juhasz-Boess, I.; Lattrich, C.; Ortmann, O.; Treeck, O. (2010). "Estrogen receptor β gene polymorphisms and susceptibility to uterine fibroids". Gynecological Endocrinology 26 (1): 4. doi:10.3109/09513590903159573. PMID 19639498.
- ^ Alhendy, A.; Salama, S. (2006). "Ethnic distribution of estrogen receptor-α polymorphism is associated with a higher prevalence of uterine leiomyomas in black Americans". Fertility and Sterility 86 (3): 686. doi:10.1016/j.fertnstert.2006.01.052. PMID 16860797.
- ^ Nam, D. -H.; Ramachandran, S.; Song, D. -K.; Kwon, K. -Y.; Jeon, D. -S.; Shin, S. -J.; Kwon, S. -H.; Cha, S. -D. et al. (2007). "Growth inhibition and apoptosis induced in human leiomyoma cells by treatment with the PPAR gamma ligand ciglitizone". Molecular Human Reproduction 13 (11): 829–836. doi:10.1093/molehr/gam071. PMID 17893092.
- ^ Zhang, CH; Wen, ZQ; Li, JF; Li, CZ; Shi, M; Yang, GW; Lan, SM; Zhu, Y et al. (2008). "Inhibition of proliferation and transforming growth factor beta3 protein expression by peroxisome proliferators-activated receptor gamma ligands in human uterine leiomyoma cells". Chinese medical journal 121 (2): 166–71. PMID 18272045.
- ^ Boynton-Jarrett, R.; Rich-Edwards, J.; Malspeis, S.; Missmer, S. A.; Wright, R. (2005). "A Prospective Study of Hypertension and Risk of Uterine Leiomyomata". American Journal of Epidemiology 161 (7): 628. doi:10.1093/aje/kwi072. PMID 15781952.
- ^ Isobe, A.; Takeda, T.; Sakata, M.; Miyake, A.; Yamamoto, T.; Minekawa, R.; Nishimoto, F.; Oskamoto, Y. et al. (2007). "Dual repressive effect of angiotensin II-type 1 receptor blocker telmisartan on angiotensin II-induced and estradiol-induced uterine leiomyoma cell proliferation". Human Reproduction 23 (2): 440. doi:10.1093/humrep/dem247. PMID 17993476.
- ^ Shozu, M.; Murakami, K.; Inoue, M. (2004). "Aromatase and Leiomyoma of the Uterus". Seminars in Reproductive Medicine 22 (1): 51. doi:10.1055/s-2004-823027. PMID 15083381.
- ^ Bulun, S.; Yang, S.; Fang, Z.; Gurates, B.; Tamura, M.; Zhou, J.; Sebastian, S. (2001). "Role of aromatase in endometrial disease". The Journal of steroid biochemistry and molecular biology 79 (1–5): 19–25. doi:10.1016/S0960-0760(01)00134-0. PMID 11850203.
- ^ Ishikawa, H.; Reierstad, S.; Demura, M.; Rademaker, A. W.; Kasai, T.; Inoue, M.; Usui, H.; Shozu, M. et al. (2009). "High Aromatase Expression in Uterine Leiomyoma Tissues of African-American Women". Journal of Clinical Endocrinology & Metabolism 94 (5): 1752. doi:10.1210/jc.2008-2327. PMC 2684481. PMID 19240151. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2684481.
- ^ Hodge, J.; Morton, C. (2007). "Genetic heterogeneity among uterine leiomyomata: insights into malignant progression". Human molecular genetics 16 Spec No 1: R7–13. doi:10.1093/hmg/ddm043. PMID 17613550.
- ^ Payson M, Malik M, Siti-Nur Morris S, Segars JH, Chason R, Catherino WH. (2009). "Activating transcription factor 3 gene expression suggests that tissue stress plays a role in leiomyoma development.". Fertil Steril. 2009 Aug;92(2):748-55. Epub 2008 Aug 9. 92 (2): 748–55. doi:10.1016/j.fertnstert.2008.06.030. PMID 18692824.
- ^ Nierth-Simpson, E.; Martin, M.; Chiang, T.; Melnik, L.; Rhodes, L.; Muir, S.; Burow, M.; McLachlan, J. (2009). "Human uterine smooth muscle and leiomyoma cells differ in their rapid 17beta-estradiol signaling: implications for proliferation". Endocrinology 150 (5): 2436–2445. doi:10.1210/en.2008-0224. PMC 2671893. PMID 19179429. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2671893.
- ^ a b Weston, G.; Trajstman, A.; Gargett, C.; Manuelpillai, U.; Vollenhoven, B.; Rogers, P. (2003). "Fibroids display an anti-angiogenic gene expression profile when compared with adjacent myometrium". Molecular human reproduction 9 (9): 541–549. doi:10.1093/molehr/gag066. PMID 12900513.
- ^ Goto A, Takeuchi S, Sugimura K, Maruo T (2002). "Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination of LDH and its isozymes in the differential diagnosis of leiomyosarcoma from degenerated leiomyoma of the uterus". Int. J. Gynecol. Cancer 12 (4): 354–61. doi:10.1046/j.1525-1438.2002.01086.x. PMID 12144683.
- ^ Fibroids – What is it? – Introduction
- ^ Zapata, Lauren B.; Whiteman, Maura K.; Tepper, Naomi K.; Jamieson, Denise J.; Marchbanks, Polly A.; Curtis, Kathryn M. (2010). "Intrauterine device use among women with uterine fibroids: a systematic review☆". Contraception 82 (1): 41–55. doi:10.1016/j.contraception.2010.02.011. PMID 20682142.
- ^ Jindabanjerd, K; Taneepanichskul, S (2006). "The use of levonorgestrel - IUD in the treatment of uterine myoma in Thai women". Journal of the Medical Association of Thailand = Chotmaihet thangphaet 89 Suppl 4: S147–51. PMID 17726816.
- ^ a b c d e f Sankaran, S.; Manyonda, I. (2008). "Medical management of fibroids". Best Practice & Research Clinical Obstetrics & Gynaecology 22 (4): 655. doi:10.1016/j.bpobgyn.2008.03.001. PMID 18468953. http://www.britishfibroidtrust.org.uk/journals/bft_Sankaran.pdf
- ^ Kailasam, C; Cahill, D (2008). "Review of the safety, efficacy and patient acceptability of the levonorgestrel-releasing intrauterine system". Patient preference and adherence 2: 293–302. PMC 2770406. PMID 19920976. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2770406.
- ^ Sayyah-Melli, M; Tehrani-Gadim, S; Dastranj-Tabrizi, A; Gatrehsamani, F; Morteza, G; Ouladesahebmadarek, E; Farzadi, L; Kazemi-Shishvan, M (2009). "Comparison of the effect of gonadotropin-releasing hormone agonist and dopamine receptor agonist on uterine myoma growth. Histologic, sonographic, and intra-operative changes". Saudi medical journal 30 (8): 1024–33. PMID 19668882.
- ^ Engman M, Granberg S, Williams ARW, Meng CX, Lalitkumar PGL, Gemzell-Danielsson K (August 2009). "Mifepristone for Treatment of Uterine Leiomyoma. A Prospective Randomized Placebo Controlled Trial". Human Reproduction 24 (8): 1870–9 24 (8): 1870–9. doi:10.1093/humrep/dep100. PMID 19389793.
- ^ Malartic, C.; Morel, O.; Akerman, G.; Tulpin, L.; Desfeux, P.; Barranger, E. (2008). "La mifépristone dans la prise en charge des fibromes utérins". Gynécologie Obstétrique & Fertilité 36: 668. doi:10.1016/j.gyobfe.2008.01.017.
- ^ Wilkens, J; Williams, AR; Chwalisz, K; Han, C; Cameron, IT; Critchley, HO (2009). "Effect of asoprisnil on uterine proliferation markers and endometrial expression of the tumour suppressor gene, PTEN". Human reproduction (Oxford, England) 24 (5): 1036–44. doi:10.1093/humrep/den494. PMID 19176543.
- ^ http://www.apmhealtheurope.com/story.php?include_profilDepsPage=197&numero=283&profil=94&ctx=6a15602f32780ba0e6037b5e94f2b272
- ^ The Embolisation Process: What's Involved
- ^ Hirst, A; Dutton, S; Wu, O; Briggs, A; Edwards, C; Waldenmaier, L; Maresh, M; Nicholson, A et al. (2008). "A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study". Health technology assessment (Winchester, England) 12 (5): 1–248, iii. PMID 18331704.
- ^ Liu, WM; Ng, HT; Wu, YC; Yen, YK; Yuan, CC (2001). "Laparoscopic bipolar coagulation of uterine vessels: a new method for treating symptomatic fibroids". Fertility and sterility 75 (2): 417–22. doi:10.1016/S0015-0282(00)01724-6. PMID 11172850.
- ^ Kim, HS; Kim, JW; Kim, MK; Chung, HH; Lee, TS; Jeon, YT; Kim, YB; Jeon, HW et al. (2009). "A randomized prospective trial of the postoperative quality of life between laparoscopic uterine artery ligation and laparoscopy-assisted vaginal hysterectomy for the treatment of symptomatic uterine fibroids: clinical trial design". Trials 10: 8. doi:10.1186/1745-6215-10-8. PMC 2645389. PMID 19178748. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2645389.
- ^ Akinola, OI; Fabamwo, AO; Ottun, AT; Akinniyi, OA (2005). "Uterine artery ligation for management of uterine fibroids". International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 91 (2): 137–40. doi:10.1016/j.ijgo.2005.07.012. PMID 16168993.
- ^ Hald, K.; Noreng, H. J. �R.; Istre, O.; Kløw, N. E. (2009). "Uterine Artery Embolization versus Laparoscopic Occlusion of Uterine Arteries for Leiomyomas: Long-term Results of a Randomized Comparative Trial". Journal of Vascular and Interventional Radiology 20 (10): 1303. doi:10.1016/j.jvir.2009.07.022. PMID 19713130.
- ^ Beck, Melinda (2010-01-20). "A New Treatment to Help Women Avoid Hysterectomy". The Wall Street Journal. http://online.wsj.com/article/SB10001424052748704541004575010933671115028.html#video%3D4EEED67A-43A5-40DA-A45D-76FCC1279956%26articleTabs%3Darticle.
- ^ Polena V, Mergui JL, Perrot N, Poncelet C, Barranger E, Uzan S (February 2007). "Long-term results of hysteroscopic myomectomy in 235 patients". Eur. J. Obstet. Gynecol. Reprod. Biol. 130 (2): 232–7. doi:10.1016/j.ejogrb.2006.01.014. PMID 16530319. http://linkinghub.elsevier.com/retrieve/pii/S0301-2115(06)00051-0.
- ^ Agdi M, Tulandi T (August 2008). "Endoscopic management of uterine fibroids". Best Pract Res Clin Obstet Gynaecol 22 (4): 707–16. doi:10.1016/j.bpobgyn.2008.01.011. PMID 18325839. http://linkinghub.elsevier.com/retrieve/pii/S1521-6934(08)00024-2.
- ^ Soriano D, Dessolle L, Poncelet C, Benifla JL, Madelenat P, Darai E (June 2003). "Pregnancy outcome after laparoscopic and laparoconverted myomectomy". Eur. J. Obstet. Gynecol. Reprod. Biol. 108 (2): 194–8. PMID 12781410. http://linkinghub.elsevier.com/retrieve/pii/S0301211502004360.
- ^ "FDA Approves New Device to Treat Uterine Fibroids" (Press release). FDA. 2004-10-22. http://www.fda.gov/bbs/topics/answers/2004/ans01319.html. Retrieved 2008-05-26.
- ^ Shen, SH; Fennessy, F, McDannold, N, Jolesz, F, Tempany, C (2009 Apr). "Image-guided thermal therapy of uterine fibroids.". Seminars in ultrasound, CT, and MR 30 (2): 91–104. PMID 19358440.
- ^ Stewart EA, Rabinovici J, Tempany CM, et al. (January 2006). "Clinical outcomes of focused ultrasound surgery for the treatment of uterine fibroids". Fertil. Steril. 85 (1): 22–9. doi:10.1016/j.fertnstert.2005.04.072. PMID 16412721. http://linkinghub.elsevier.com/retrieve/pii/S0015-0282(05)03655-1.
- ^ Kurashvili, J., et al. (2010). "MRgFUS Treatment for Uterine Myomas: Safety, Effectiveness and Pathogenesis". MR-guided Focused Ultrasound 2010, 2nd International Symposium.
- ^ O'Sullivan AK, Thompson D, Chu P, Lee DW, Stewart EA, Weinstein MC (January 2009). "Cost-effectiveness of magnetic resonance guided focused ultrasound for the treatment of uterine fibroids". Int J Technol Assess Health Care 25 (1): 14–25. doi:10.1017/S0266462309090035. PMC 2811401. PMID 19126247. http://journals.cambridge.org/abstract_S0266462309090035.
- ^ Zowall H, Cairns JA, Brewer C, Lamping DL, Gedroyc WM, Regan L (April 2008). "Cost-effectiveness of magnetic resonance-guided focused ultrasound surgery for treatment of uterine fibroids". BJOG 115 (5): 653–62. doi:10.1111/j.1471-0528.2007.01657.x. PMC 2344162. PMID 18333948. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2344162.
- ^ a b Uterine Fibroids at Merck Manual of Diagnosis and Therapy Professional Edition
- ^ Wise LA, Palmer JR, Stewart EA, Rosenberg L (March 2005). "Age-specific incidence rates for self-reported uterine leiomyomata in the Black Women's Health Study". Obstet Gynecol 105 (3): 563–8. doi:10.1097/01.AOG.0000154161.03418.e3. PMC 1847590. PMID 15738025. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1847590.
- ^ "Helping Black Women Recognize, Treat Fibroids". NPR. http://www.npr.org/templates/story/story.php?storyId=89344394. Retrieved 30 March 2011.
- ^ "African American Women and Fibroids". Philadelphia Black Women's Health Project. http://www.blackwomenshealthproject.org/aafibroids.htm. Retrieved 30 March 2011.
- ^ "Minority Women's Health". Women's Health.gov. http://www.womenshealth.gov/minority/africanamerican/uterine-fibroids.cfm.
- ^ a b c d "Black Women and High Prevalence of Fibroids". Fibroid Treatment Collective. November 29, 2010. http://www.fibroids.com/news-blog/2010/11/black-women-fibroids/. Retrieved 30 March 2011.
- ^ a b "Increased Dairy Intake Reduces Risk of Uterine Fibroids in Black Women, Study Suggests". Science Daily. December 4, 2009. http://www.sciencedaily.com/releases/2009/12/091204092459.htm. Retrieved 30 March 2011.
- ^ Fletcher's Diagnostic Histopathology of Tumors (3rd ed.). pp. 692–4.
- ^ http://officeofbudget.od.nih.gov/pdfs/FY11/Approp.%20History%20by%20IC%20(FINAL).pdf
- ^ Bäcklin BM, Eriksson L, Olovsson M (March 2003). "Histology of uterine leiomyoma and occurrence in relation to reproductive activity in the Baltic gray seal (Halichoerus grypus)". Vet. Pathol. 40 (2): 175–80. doi:10.1354/vp.40-2-175. PMID 12637757. http://vet.sagepub.com/content/40/2/175.full.
Tumors: female urogenital neoplasia (C51–C58/D25–D28, 179–184/218–221) Adnexa Glandular and epithelial/
surface epithelial-
stromal tumorCMS: Ovarian serous cystadenoma · Mucinous cystadenoma · Cystadenocarcinoma (Papillary serous cystadenocarcinoma) · Krukenberg tumorSex cord-gonadal stromalLeydig cell tumour · Sertoli cell tumour · Sertoli-Leydig cell tumour · Thecoma · Granulosa cell tumour · LuteomaDysgerminoma · Nongerminomatous (Embryonal carcinoma, Endodermal sinus tumor, Gonadoblastoma, Teratoma/Struma ovarii, Choriocarcinoma)Uterus Endometrioid tumor · Uterine papillary serous carcinoma · Clear cell carcinoma · Endometrial intraepithelial neoplasiaGeneralVagina SCC · Botryoid rhabdomyosarcoma · Clear cell adenocarcinoma of the vagina · Vaginal intraepithelial neoplasiaVulva Categories:- Gynaecological neoplasia
- Benign neoplasms



Wikimedia Foundation. 2010.