- Nasogastric intubation
-
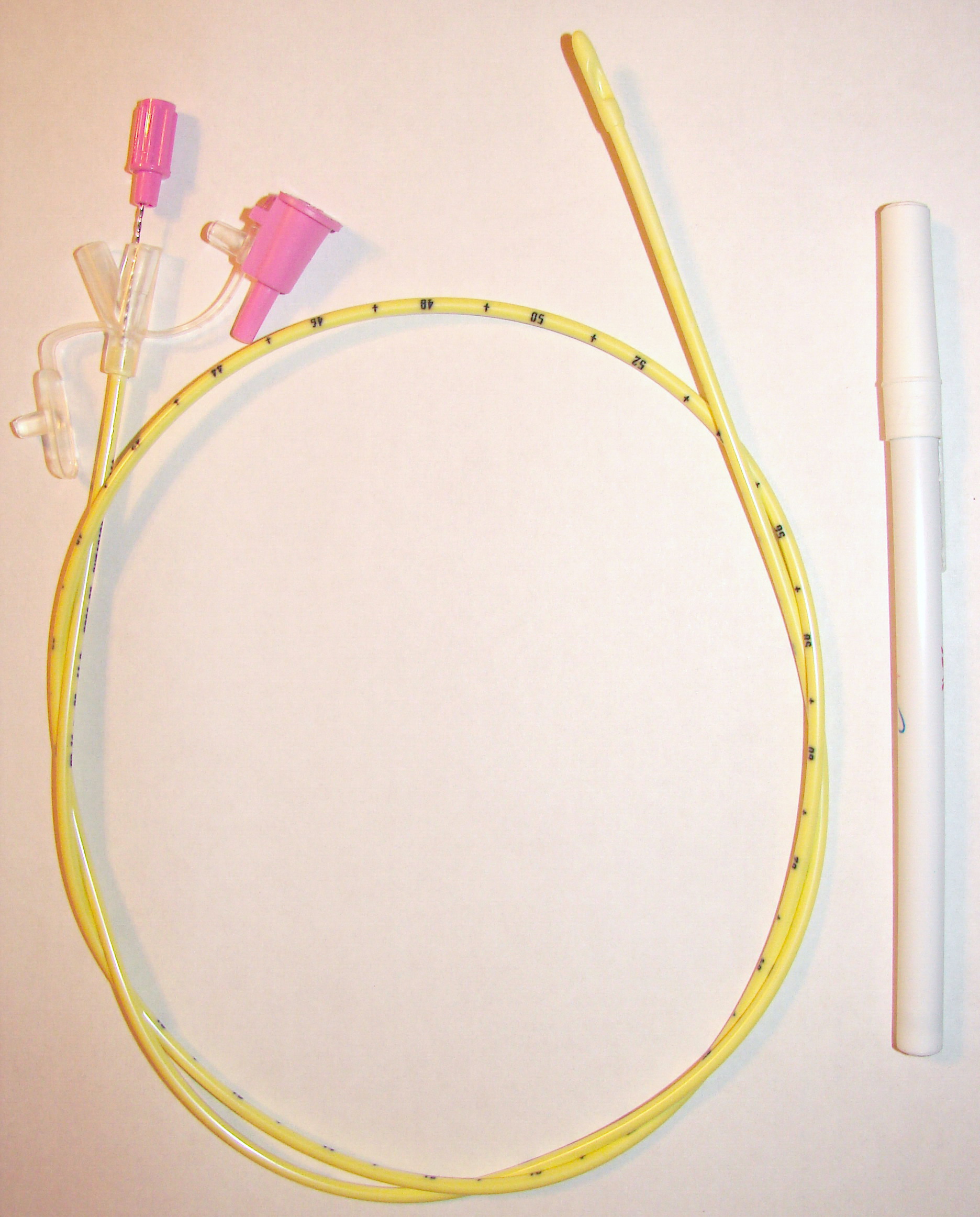
Nasogastric intubation Intervention 
Stomach tube (Levin type), 18 Fr × 48 in (121 cm)ICD-9-CM 96.07, 96.6 Nasogastric intubation is a medical process involving the insertion of a plastic tube (nasogastric tube or NG tube) through the nose, past the throat, and down into the stomach.
Contents
Uses
A nasogastric tube is used for feeding and administering drugs and other oral agents such as activated charcoal. For drugs and for minimal quantities of liquid, a syringe is used for injection into the tube. For continuous feeding, a gravity based system is employed, with the solution placed higher than the patient's stomach. If accrued supervision is required for the feeding, the tube is often connected to an electronic pump which can control and measure the patient's intake and signal any interruption in the feeding.
Nasogastric aspiration (suction) is the process of draining the stomach's contents via the tube. Nasogastric aspiration is mainly used to remove gastric secretions and swallowed air in patients with gastrointestinal obstructions. Nasogastric aspiration can also be used in poisoning situations when a potentially toxic liquid has been ingested, for preparation before surgery under anesthesia, and to extract samples of gastric liquid for analysis.
If the tube is to be used for continuous drainage, it is usually appended to a collector bag placed below the level of the patient's stomach; gravity empties the stomach's contents. It can also be appended to a suction system, however this method is often restricted to emergency situations, as the constant suction can easily damage the stomach's lining. In non-emergent situations, intermittent suction may be applied giving the benefits of suction without the untoward effects of damage to the stomach lining.
Suction drainage is used for patients who have undergone a pneumonectomy in order to prevent anesthesia-related vomiting and possible aspiration of any stomach contents. Such aspiration would represent a serious risk of complications to patients recovering from this surgery.
Technique
Before an NG tube is inserted the health care provider must measure with the tube from the tip of the patient's nose to their ear and down to the xyphoid process. Then the tube is marked at this level to ensure that the tube has been inserted far enough into the patient's stomach. Many commercially available stomach and duodenal tubes have several standard depth markings, for example 18" (46 cm), 22" (56 cm), 26" (66 cm) and 30" (76 cm) from distal end; infant feeding tubes often come with 1 cm depth markings. The end of a plastic tube is lubricated (local anesthetic, such as 2% xylocaine gel, may be used; in addition, nasal vasoconstrictor spray may be applied before the insertion) and inserted into one of the patient's anterior nares. The tube should be directed aiming down and back as it is moved through the nasal cavity and down into the throat. When the tube enters the oropharynx and glides down the posterior pharyngeal wall, the patient may gag; in this situation the patient, if awake and alert, is asked to mimic swallowing or is given some water to sip through a straw, and the tube continues to be inserted as the patient swallows. Once the tube is past the pharynx and enters the esophagus, it is easily inserted down into the stomach.
Great care must be taken to ensure that the tube has not passed through the larynx into the trachea and down into the bronchi. To ensure proper placement it is recommended (though not unequivocally confirmed) that injection of air into the tube be performed,[1] if the air is heard in the stomach with a stethoscope, then the tube is in the correct position. Another more reliable method is to aspirate some fluid from the tube with a syringe. This fluid is then tested with pH paper (note not litmus paper) to determine the acidity of the fluid. If the pH is 5.5 or below then the tube is in the correct position. If this is not possible then correct verification of tube position is obtained with an X-ray of the chest/abdomen. This is the most reliable means of ensuring proper placement of an NG tube.[2] Future techniques may include measuring the concentration of enzymes such as trypsin, pepsin, and bilirubin to confirm the correct placement of the NG tube. As enzyme testing becomes more practical, allowing measurements to be taken quickly and cheaply at the bedside, this technique may be used in combination with pH testing as an effective, less harmful replacement of X-ray confirmation.[3] If the tube is to remain in place then a tube position check is recommended before each feed and at least once per day.
 Polyurethane NG tube (Viasys Corflo), 8 Fr × 36 in (91 cm). This fine bore tube is appropriate for longer use (up to 4 weeks).
Polyurethane NG tube (Viasys Corflo), 8 Fr × 36 in (91 cm). This fine bore tube is appropriate for longer use (up to 4 weeks).
Only smaller diameter (12 Fr or less in adults) nasogastric tubes are appropriate for long-term feeding, so as to avoid irritation and erosion of the nasal mucosa. These tubes often have guidewires to facilitate insertion. If feeding is required for a longer period of time, other options, such as placement of a PEG tube, should be considered.
Contraindications
The use of nasogastric intubation is contraindicated in patients with base of skull fractures, severe facial fractures especially to the nose and obstructed esophagus, esophageal varices, and/or obstructed airway.
The use of an NG tube is also contraindicated in patients who have had gastric bypass surgery.
Complications
Minor complications include nose bleeds, sinusitis, and a sore throat.
Sometimes more significant complications occur including erosion of the nose where the tube is anchored, esophageal perforation, pulmonary aspiration, a collapsed lung, or intracranial placement of the tube.
See also
- Force feeding
- Tubefeeding
References
- ^ Thomsen TW, Shaffer RW, Setnik GS. (2006). "Videos in clinical medicine. Nasogastric intubation". N Engl J Med 354 (17): e16. doi:10.1056/NEJMvcm050183. PMID 16641390.
- ^ Thomas B, Cummin D, Falcone RE. (1996). "Accidental pneumothorax from a nasogastric tube". N Engl J Med 335 (17): 1325. doi:10.1056/NEJM199610243351717. PMID 8992337.
- ^ Cincinnatti Children's Hospital Medical Center (2009). "Best evidence statement (BESt). Confirmation of nasogastric tube placement in pediatric patients.". National Guidelines Clearing House: 11.
Categories:- Medical equipment
- Enteral feeding
- Medical treatments

Wikimedia Foundation. 2010.