- Common carotid artery
-
Artery: Common carotid artery 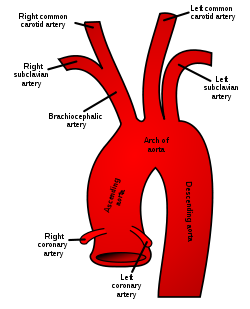
Schematic of the proximal aorta and its branches. 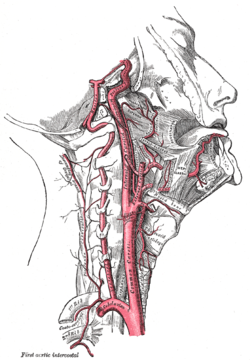
Arteries of the neck. The internal carotid arteries arise from the common carotid arteries - labeled Common caroti on the figure. Latin a. carotis communis Gray's subject #143 549 Supplies head and neck Source aortic arch, brachiocephalic artery Branches internal carotid artery, external carotid artery Vein internal jugular vein Precursor aortic arch 3 MeSH Carotid+Artery,+Common In human anatomy, the common carotid artery is an artery that supplies the head and neck with oxygenated blood; it divides in the neck to form the external and internal carotid arteries.[1] [2]
Contents
Structure
The common carotid artery is a paired structure, meaning that there are two in the body, one for each half. The left and right common carotid arteries follow the same course with the exception of their origin. The right common carotid originates in the neck from the brachiocephalic trunk. The left arises from the aortic arch in the thoracic region.
The left common carotid artery can be thought of as having two parts: a thoracic (chest) part and a cervical (neck) part. The right common carotid originates in or close to the neck, so contains a small thoracic portion. There are studies in the bioengineering literature that has looked into characterizing the geometric structure of the common carotid artery from both a qualitative and mathematical quantitative stand point. [3]
Thoracic part
Only the left common carotid artery has a substantial presence in the thoracic region. It originates along the aortic arch, and travels upward through the superior mediastinum to the level of the left sternoclavicular joint, where it is continuous with the cervical portion.
During the thoracic part of its course, the left common carotid artery is related to the following structures: In front, it is separated from the manubrium of the sternum by the sternohyoid and sternothyroid muscles, the anterior portions of the left pleura and lung, the left brachiocephalic vein, and the remains of the thymus; behind, it lies on the trachea, esophagus, left recurrent laryngeal nerve, and thoracic duct.
To its right side below is the brachiocephalic trunk, and above, the trachea, the inferior thyroid veins, and the remains of the thymus; to its left side are the left vagus and phrenic nerves, left pleura, and lung. The left subclavian artery is posterior and slightly lateral to it.
Cervical part
 Diagram showing the origins of the main branches of the carotid arteries.
Diagram showing the origins of the main branches of the carotid arteries.
The cervical portions of the common carotids resemble each other so closely that one description will apply to both.
Each vessel passes obliquely upward, from behind the sternoclavicular joint to the level of the upper border of the thyroid cartilage, where it divides.
At the lower part of the neck the two common carotid arteries are separated from each other by a very narrow interval which contains the trachea; but at the upper part, the thyroid gland, the larynx and pharynx project forward between the two vessels.
The common carotid artery is contained in a sheath known as the carotid sheath, which is derived from the deep cervical fascia and encloses also the internal jugular vein and vagus nerve, the vein lying lateral to the artery, and the nerve between the artery and vein, on a plane posterior to both. On opening the sheath, each of these three structures is seen to have a separate fibrous investment.
At approximately the level of the fourth cervical vertebra, the common carotid artery bifurcates into an internal carotid artery (ICA) and an external carotid artery (ECA). While both branches travel upward, the internal carotid takes a deeper (more internal) path, eventually travelling up into the skull to supply the brain via the carotid canal. The external carotid artery travels more closely to the surface, and sends off numerous branches that supply the neck and face.
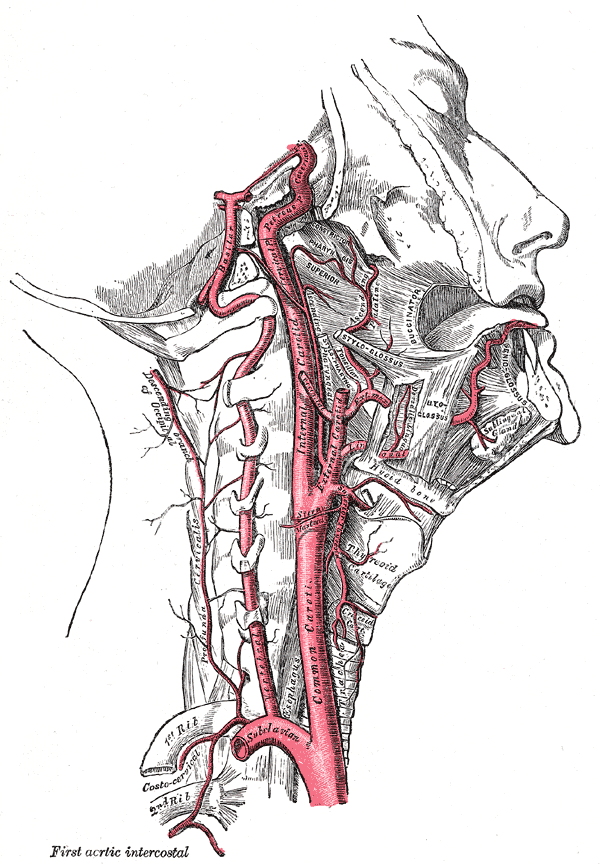
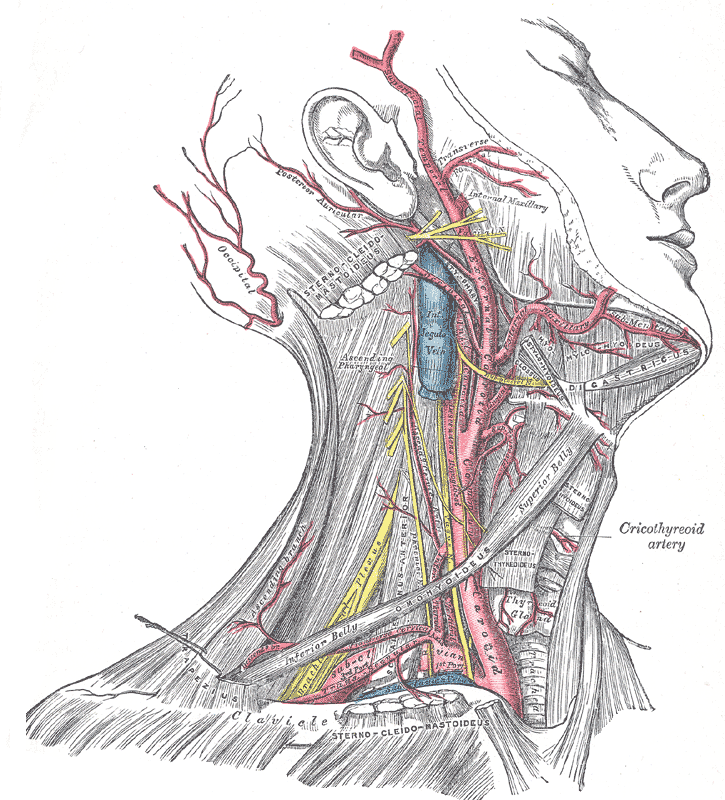
 Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries.
Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries.At the lower part of the neck the common carotid artery is very deeply seated, being covered by the integument, superficial fascia, the platysma muscle, deep cervical fascia, the sternocleidomastoid muscle, the sternohyoid, sternothyroid, and the omohyoid; in the upper part of its course it is more superficial, being covered merely by the integument, the superficial fascia, the platysma, deep cervical fascia, and medial margin of the sternocleidomastoid.
When the sternocleidomastoid muscle is drawn backward, the artery is seen to be contained in a triangular space known as the carotid triangle. This space is bounded behind by the sternocleidomastoid, above by the stylohyoid and the posterior belly of the digastric muscle, and below by the superior belly of the omohyoid.
This part of the artery is crossed obliquely, from its medial to its lateral side, by the sternocleidomastoid branch of the superior thyroid artery; it is also crossed by the superior and middle thyroid veins (which end in the internal jugular vein); descending in front of its sheath is the descending branch of the hypoglossal nerve, this filament being joined by one or two branches from the cervical nerves, which cross the vessel obliquely.
Sometimes the descending branch of the hypoglossal nerve is contained within the sheath.
The superior thyroid vein crosses the artery near its termination, and the middle thyroid vein a little below the level of the cricoid cartilage; the anterior jugular vein crosses the artery just above the clavicle, but is separated from it by the sternohyoid and sternothyroid.
Behind, the artery is separated from the transverse processes of the cervical vertebrae by the longus colli and longus capitis muscles, the sympathetic trunk being interposed between it and the muscles. The inferior thyroid artery crosses behind the lower part of the vessel.
Medially, it is in relation with the esophagus, trachea, and thyroid gland (which overlaps it), the inferior thyroid artery and recurrent laryngeal nerve being interposed; higher up, with the larynx and pharynx. Lateral to the artery, inside the carotid sheath with the common carotid, are the internal jugular vein and vagus nerve.
At the lower part of the neck, on the right side of the body, the right recurrent laryngeal nerve crosses obliquely behind the artery; the right internal jugular vein diverges from the artery. On the left side, however, the left internal jugular vein approaches and often overlaps the lower part of the artery.
Behind the angle of bifurcation of the common carotid artery is a reddish-brown oval body known as the carotid body. It is similar in structure to the coccygeal body which is situated on the median sacral artery.
The relations of the cervical region of the common carotid artery may be discussed in two points:
- Internal relations of organs present inside the carotid sheath
- two external relations of carotid sheath
Collateral circulation
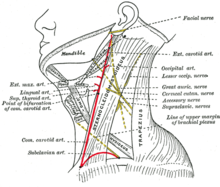 Side of neck, showing chief surface markings.
Side of neck, showing chief surface markings.After ligature of the common carotid, the collateral circulation can be perfectly established, by the free communication which exists between the carotid arteries of opposite sides, both without and within the cranium, and by enlargement of the branches of the subclavian artery on the side corresponding to that on which the vessel has been tied.
The chief communications outside the skull take place between the superior and inferior thyroid arteries, and the deep cervical artery and the descending branch of the occipital artery; the vertebral artery takes the place of the internal carotid artery within the cranium.
Variation
Origin
The right common carotid may arise above the level of the upper border of the sternoclavicular joint; this variation occurs in about 12 percent of cases.
In other cases the artery on the right side may arise as a separate branch from the arch of the aorta, or in conjunction with the left carotid.
The left common carotid varies in its origin more than the right.
In the majority of abnormal cases it arises with the brachiocephalic trunk; if that artery is absent, the two carotids arise usually by a single trunk.
It is rarely joined with the left subclavian artery, except in cases of transposition of the aortic arch.
Point of division
In the majority of abnormal cases, the bifurcation occurs higher than usual, the artery dividing opposite or even above the hyoid bone; more rarely, it occurs below, opposite the middle of the larynx, or the lower border of the cricoid cartilage. In at least one reported case, the artery was only 4 cm in length and divided at the root of the neck.
 Common carotid artery
Common carotid arteryVery rarely, the common carotid artery ascends in the neck without any subdivision, either the external or the internal carotid being absent; and in a few cases the common carotid has itself been found to be absent, the external and internal carotids arising directly from the arch of the aorta.
This peculiarity existed on both sides in some instances, on one side in others.
Occasional branches
The common carotid usually gives off no branch previous to its bifurcation, but it occasionally gives origin to the superior thyroid artery or its laryngeal branch, the ascending pharyngeal artery, the inferior thyroid artery, or, more rarely, the vertebral artery.
Clinical significance
The common carotid artery is often used in measuring the pulse,[4] especially in patients who are in shock and who lack a detectable pulse in the more peripheral arteries of the body.
The carotid artery should be palpated gently and while the patient is sitting or lying down. Stimulating its baroreceptors with low palpitation can provoke severe bradycardia or even stop the heart in some sensitive persons. Also, a person's two carotid arteries should not be palpated at the same time. Doing so may limit the flow of blood to the head, possibly leading to fainting or brain ischemia. It can be felt between the anterior border of the sternocleidomastoid muscle, above the hyoid bone and lateral to the thyroid cartilage.
Presence of a carotid pulse has been estimated to indicate a systolic blood pressure of more than 40 mmHg, as given by the 50% percentile.[5]
Pathophysiology
Carotidynia is a syndrome marked by soreness of the carotid artery near the bifurcation.
Carotid stenosis may occur in patients with atherosclerosis.
Gallery
-

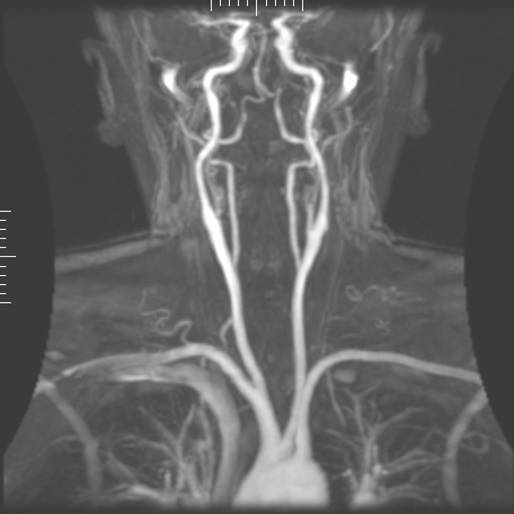
Magnetic Resonance Angiography
-

Normal carotidal arteriography
See also
References
- ^ Ashrafian H. Anatomically specific clinical examination of the carotid arterial tree. Anat Sci Int. 2007 Mar;82(1):16–23.
- ^ Manbachi, A., Hoi, Y., Wasserman, B. A. Lakatta, E.G. and Steinman. D.A. (November 2011). ""On the shape of the common carotid artery with implications for blood velocity profiles."". Physiol. Meas. 32 (12): 1885–1897. doi:10.1088/0967-3334/32/12/001. PMID 22031538. http://iopscience.iop.org/0967-3334/32/12/001/.
- ^ Manbachi, A., Hoi, Y., Wasserman, B. A. Lakatta, E.G. and Steinman. D.A. (November 2011). ""On the shape of the common carotid artery with implications for blood velocity profiles."". Physiol. Meas. 32 (12): 1885–1897. doi:10.1088/0967-3334/32/12/001. PMID 22031538. http://iopscience.iop.org/0967-3334/32/12/001/.
- ^ Ashrafian H. Anatomically specific clinical examination of the carotid arterial tree. Anat Sci Int. 2007 Mar;82(1):16-23.
- ^ Deakin CD, Low JL (September 2000). "Accuracy of the advanced trauma life support guidelines for predicting systolic blood pressure using carotid, femoral, and radial pulses: observational study". BMJ 321 (7262): 673–4. doi:10.1136/bmj.321.7262.673. PMC 27481. PMID 10987771. http://bmj.com/cgi/pmidlookup?view=long&pmid=10987771.
External links
List of arteries of torso · chest (TA A12.2.01–04,11, GA 6.598) Pulmonary Coronary Ascending aorta/
aortic archLeft common carotidInternal thoracic: Anterior intercostal · Thymic · Pericardiacophrenic · Perforating branches · terminal (Musculophrenic, superior epigastric)
Costocervical trunk: Highest intercostal (Posterior intercostal 1–2) · Deep cervicalOtherDescending/
thoracic aortavisceral: Bronchial · Esophageal · Mediastinal
parietal: Posterior intercostal 3·11 · Subcostal · Superior phrenicCategories:- Arteries of the head and neck
- Arteries of the thorax





Wikimedia Foundation. 2010.