- Health care in Canada
-
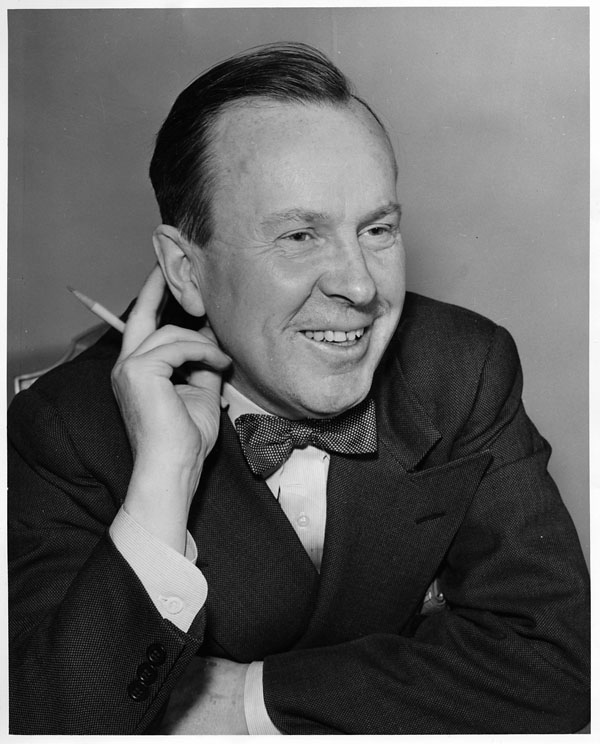
 Tommy Douglas' (centre left) number one concern was the creation of Medicare. In the summer of 1962, Saskatchewan became the centre of a hard-fought struggle between the provincial government, the North American medical establishment, and the province's physicians, who brought things to a halt with a doctors' strike.
Tommy Douglas' (centre left) number one concern was the creation of Medicare. In the summer of 1962, Saskatchewan became the centre of a hard-fought struggle between the provincial government, the North American medical establishment, and the province's physicians, who brought things to a halt with a doctors' strike.
Health care in Canada is delivered through a publicly-funded health care system, which is mostly free at the point of use and has most services provided by private entities.[2] It is guided by the provisions of the Canada Health Act.[3] The government assures the quality of care through federal standards. The government does not participate in day-to-day care or collect any information about an individual's health, which remains confidential between a person and his or her physician. Canada's provincially-based Medicare systems are cost-effective partly because of their administrative simplicity.[citation needed] In each province each doctor handles the insurance claim against the provincial insurer. There is no need for the person who accesses health care to be involved in billing and reclaim. Private insurance is only a minimal part of the overall health care system. Competitive practices such as advertising are kept to a minimum, thus maximizing the percentage of revenues that go directly towards care.[citation needed] In general, costs are paid through funding from income taxes, although British Columbia is the only province to impose a fixed monthly premium which is waived or reduced for those on low incomes.[4] There are no deductibles on basic health care and co-pays are extremely low or non-existent (supplemental insurance such as Fair Pharmacare may have deductibles, depending on income).
A health card is issued by the Provincial Ministry of Health to each individual who enrolls for the program and everyone receives the same level of care.[5] There is no need for a variety of plans because virtually all essential basic care is covered, including maternity and infertility problems. Depending on the province, dental and vision care may not be covered but are often insured by employers through private companies. In some provinces, private supplemental plans are available for those who desire private rooms if they are hospitalized. Cosmetic surgery and some forms of elective surgery are not considered essential care and are generally not covered. These can be paid out-of-pocket or through private insurers. Health coverage is not affected by loss or change of jobs, as long as premiums are up to date, and there are no lifetime limits or exclusions for pre-existing conditions.
Pharmaceutical medications are covered by public funds for the elderly or indigent,[6] or through employment-based private insurance. Drug prices are negotiated with suppliers by the federal government to control costs. Family physicians are chosen by individuals. If a patient wishes to see a specialist or is counseled to see a specialist, a referral can be made by a GP. Preventive care and early detection are considered important and yearly checkups are encouraged. Early detection not only extends life expectancy and quality of life, but cuts down overall costs.
Contents
Public opinion
Canadians strongly support the health system's public rather than for-profit private basis, and a 2009 poll by Nanos Research found 86.2% of Canadians surveyed supported or strongly supported "public solutions to make our public health care stronger."[7][8]
A 2009 Harris/Decima poll found 82% of Canadians preferred their healthcare system to the one in the United States, more than ten times as many as the 8% stating a preference for a US-style health care system for Canada[9] while a Strategic Counsel survey in 2008 found 91% of Canadians preferring their healthcare system to that of the U.S.[10][11] In the same poll, when asked "overall the Canadian health care system was performing very well, fairly well, not very well or not at all?" 70% of Canadians rated their system as working either "well" or "very well".[citation needed] A 2003 Gallup poll found only 25% of Americans are either "very" or "somewhat" satisfied with "the availability of affordable healthcare in the nation", versus 50% of those in the UK and 57% of Canadians. Those "very dissatisfied" made up 44% of Americans, 25% of respondents of Britons, and 17% of Canadians.[12]
Economics

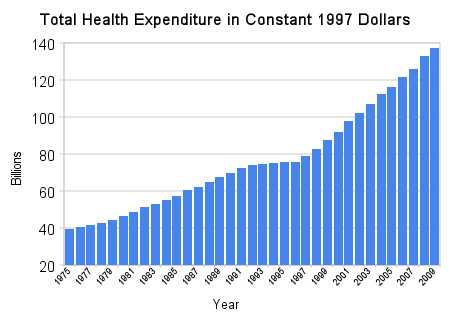
The amount Canadians spend on health care in 1997 dollars has increased every year between 1975 and 2009 from $39.7 billion to $137.3 billion or a more than doubling of per capita spending from $1,715 to $4089.[15] In 2009 dollars spending is expected to reach $183.1 billion ( a more than five percent increase over the previous year ) or $5,452 per person.[16] Most of this increase in health care costs has been covered by public funds.[17] The greatest proportion of this money goes to hospitals ($51B), followed by pharmaceuticals ($30B), and physicians ($26B).[16] Total spending in 2007 was equivalent to 10.1% of the gross domestic product which was slightly above the average for OECD countries, and below the 16.0% of GDP spent on health care in the United States.[18] The proportion spent on hospitals and physicians has declined between 1975 and 2009 while the amount spent on pharmaceuticals has increased.[19]
Of the three biggest health care expenses, the amount spent on pharmaceuticals has increased the most. In 1997 the total price of drugs surpassed that of doctors. In 1975 the three biggest health costs were hospitals ($5.5B/44.7%), physicians ($1.8B/15.1% ), and medications ($1.1B/8.8% ) while in 2007 the three biggest costs were hospitals ($45.4B/28.2% ), medications ($26.5B/16.5% ), and physicians ($21.5B/13.4% ).[20]
In 2009, the government funded about 70% of Canadians' health care costs.[21] This covered most hospital and physician cost while the dental and pharmaceutical costs were primarily paid for by individuals.[21] This is slightly below the OECD average. Under the terms of the Canada Health Act, public funding is required to pay for medically necessary care, but only if it is delivered in hospitals or by physicians. There is considerable variation across the provinces/territories as to the extent to which such costs as out of hospital prescription medications, physical therapy, long-term care, dental care and ambulance services are covered.[22]
Canada has a publicly funded medicare system, with most services provided by the private sector. Each province may opt out, though none currently do. Canada's system is known as a single payer system, where basic services are provided by private doctors (since 2002 they have been allowed to incorporate), with the entire fee paid for by the government at the same rate. Most government funding (94%) comes from the provincial level.[14] Most family doctors receive a fee per visit. These rates are negotiated between the provincial governments and the province's medical associations, usually on an annual basis. Pharmaceutical costs are set at a global median by government price controls.
Hospital care is delivered by publicly funded hospitals in Canada. Most of the public hospitals, each of which are independent institutions incorporated under provincial Corporations Acts, are required by law to operate within their budget.[23] Amalgamation of hospitals in the 1990s has reduced competition between hospitals. As the cost of patient care has increased, hospitals have been forced to cut costs or reduce services. Applying perspective (pharmacoeconomic) to analyze cost reduction, it has been shown that savings made by individual hospitals result in actual cost increases to the Provinces.[24]
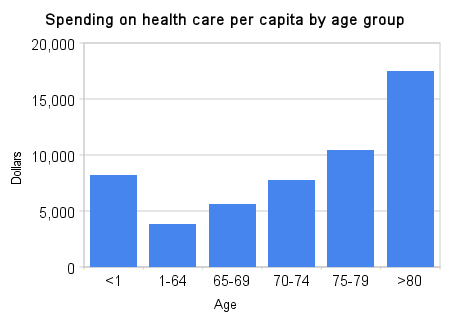
Health care costs per capita vary across Canada with Quebec ($4,891) and British Columbia ($5,254) at the lowest level and Alberta ($6,072) and Newfoundland ($5,970) at the highest.[14] It is also the greatest at the extremes of age at a cost of $17,469 per capita in those older than 80 and $8,239 for those less than 1 year old in comparison to $3,809 for those between 1 and 64 years old in 2007.[14]
History
18th century
Hospitals were initially places which cared for the poor; others were cared for at home. In Quebec (formerly known as New France and then as Lower Canada), a series of charitable institutions, many set up by Catholic religious orders, provided such care.[25] As the country grew, hospitals grew with them. They tended to be not-for-profit, and were run by municipal governments, charitable organizations, and religious denominations (both Catholic and Protestant).[26] These organizations tended to be at arm's length from government; they received subsidies from provincial governments to admit and treat all patients, regardless of their ability to pay. Dr. David Parker of the Maritimes was the first to operate using anesthetic. One of the first "modern" operations, the removal of a tumour, was performed by William Fraser Tolmie in British Columbia.
19th century
The first medical schools were established in Lower Canada in the 1820s. These included the Montreal Medical Institution, which is the faculty of medicine at McGill University today; in the mid-1870s, Sir William Osler changed the face of medical school instruction throughout the West with the introduction of the hands-on approach. The College of Physicians and Surgeons of Upper Canada was established in 1839 and in 1869 was permanently incorporated. In 1834, William Kelly, a surgeon with the Royal Navy, introduced the idea of preventing the spread of disease via sanitation measures following epidemics of cholera. In 1871, female physicians Emily Howard Stowe and Jennie Kidd Trout won the right for women to be admitted to medical schools and granted licenses from the College of Physicians and Surgeons of Ontario. In 1883, Emily Stowe led the creation of the Ontario Medical College for Women, affiliated with the University of Toronto. In 1892, Dr. William Osler wrote the landmark text The Principles and Practice of Medicine, which dominated medical instruction in the West for the next 40 years. Around this time, a movement began that called for the improved health care for the poor, focusing mainly on sanitation and hygiene. This period saw important advances including the provision of safe drinking water to most of the population, public baths and beaches, and municipal garbage services to remove waste from the city. During this period, medical care was severely lacking for the poor and minorities such as First Nations[27]
20th century
The twentieth century saw the discovery of insulin by Frederick Banting and his colleagues, Charles Best, J.J.R. Macleod, and J.B. Collip[28] in 1922. For this, Frederick Banting and J.J.R. Macleod of the University of Toronto won the 1923 Nobel Prize in Physiology and Medicine.[29] Dr. Wilder Penfield, who discovered a successful surgical treatment for epilepsy called the "Montreal procedure", founded the Montreal Neurological Institute in 1934.
The early 20th century saw the first widespread calls for increased government involvement and the idea of a national health insurance system had considerable popularity. During the Great Depression calls for a public health system were widespread. Doctors who had long feared such an idea reconsidered hoping a government system could provide some stability as the depression had badly affected the medical community. However, governments had little money to enact the idea. In 1935, the United Farmers of Alberta passed a bill creating a provincial insurance program, but they lost office later that year and the Social Credit Party scrapped the plan due to the financial situation in the province. The next year a health insurance bill passed in British Columbia, but its implementation was halted over objections from doctors. William Lyon Mackenzie King promised to introduce such a scheme, but while he created the Department of Health he failed to introduce a national program.
The beginning of coverage
 Canadian health care spending for 1970 to 2007 compared with other nations
Canadian health care spending for 1970 to 2007 compared with other nationsIt was not until 1946 that the first Canadian province introduced near universal health coverage. Saskatchewan had long suffered a shortage of doctors, leading to the creation of municipal doctor programs in the early twentieth century in which a town would subsidize a doctor to practice there. Soon after, groups of communities joined to open union hospitals under a similar model. There had thus been a long history of government involvement in Saskatchewan health care, and a significant section of it was already controlled and paid for by the government. In 1946, Tommy Douglas' Co-operative Commonwealth Federation government in Saskatchewan passed the Saskatchewan Hospitalization Act, which guaranteed free hospital care for much of the population. Douglas had hoped to provide universal health care, but the province did not have the money.
In 1950, Alberta created a program similar to Saskatchewan's. Alberta, however, created Medical Services (Alberta) Incorporated (MS(A)I) in 1948 to provide prepaid health services. This scheme eventually provided medical coverage to over 90% of the population.[30]
In 1957, the Diefenbaker federal government passed the Hospital Insurance and Diagnostic Services Act[31] to fund 50% of the cost of such programs for any provincial government that adopted them. The HIDS Act outlined five conditions: public administration, comprehensiveness, universality, portability, and accessibility. These remain the pillars of the Canada Health Act.
By 1961, all ten provinces had agreed to start HIDS Act programs. In Saskatchewan, the act meant that half of their current program would now be paid for by the federal government. Premier Woodrow Lloyd decided to use this freed money to extend the health coverage to also include physicians. Despite the sharp disagreement of the Saskatchewan College of Physicians and Surgeons, Lloyd introduced the law in 1962 after defeating the Saskatchewan Doctors' Strike in July.
Medical Care Act
The Saskatchewan program proved a success and the federal government of Lester B. Pearson introduced the Medical Care Act in 1966 that extended the HIDS Act cost-sharing to allow each province to establish a universal health care plan -an initiative that was supported by the New Democratic Party (NDP). It also set up the Medicare system. In 1984, the Canada Health Act was passed, which prohibited user fees and extra billing by doctors. In 1999, the prime minister and most premiers reaffirmed in the Social Union Framework Agreement that they are committed to health care that has "comprehensiveness, universality, portability, public administration and accessibility."[32]
Government involvement
The various levels of government pay for about 70% of Canadians' health care, although this number has decreased somewhat in recent years.[33] The Constitution Act, 1867 (formerly called the British North America Act, 1867, and still known informally as the BNA Act) did not give either the federal or provincial governments responsibility for health care, as it was then a minor concern. The Act did give the provinces responsibility for regulating hospitals, and the provinces claimed that their general responsibility for local and private matters encompassed health care. The federal government felt that the health of the population fell under the Peace, Order, and Good Government part of its responsibilities. This led to several decades of debate over jurisdiction that were not resolved until the 1930s. Eventually the Judicial Committee of the Privy Council JCPC decided that the administration and delivery of health care was a provincial concern, but that the federal government also had the responsibility of protecting the health and well-being of the population.
By far the largest government health program is Medicare, which is actually ten provincial programs, such as OHIP in Ontario, that are required to meet the general guidelines laid out in the federal Canada Health Act. Almost all government health spending goes through Medicare, but there are several smaller programs. The federal government directly administers health to groups such as the military, and inmates of federal prisons. They also provide some care to the Royal Canadian Mounted Police and veterans, but these groups mostly use the public system. Prior to 1966, Veterans Affairs Canada had a large health care network, but this was merged into the general system with the creation of Medicare. The largest group the federal government is directly responsible for is First Nations. Native peoples are a federal responsibility and the federal government guarantees complete coverage of their health needs. For the last 20 years and despite health care being a guaranteed right for First Nations due to the many treaties the government of Canada signed for access to First Nations lands and resources, the amount of coverage provided by the Federal government has diminished drastically for optometry, dentistry, and medicines. Status First Nations individuals only qualify for a set amount of visits to the optometrist and dentist, with a limited amount of coverage for glasses, eye exams, fillings, root canals, etc. For the most part First Nations people use the normal hospitals and the federal government then fully compensates the provincial government for the expense. The federal government also covers any user fees the province charges. The federal government maintains a network of clinics and health centres on Native Reserves. At the provincial level, there are also several much smaller health programs alongside Medicare. The largest of these is the health care costs paid by the worker's compensation system. Regardless of federal efforts, healthcare for First Nations has generally not been considered effective.[34][35][36]
Despite being a provincial responsibility, the large health costs have long been partially funded by the federal government. The cost sharing agreement created by the HIDS Act and extended by the Medical Care Act was discontinued in 1977 and replaced by Established Programs Financing. This gave a bloc transfer to the provinces, giving them more flexibility but also reducing federal influence on the health system. In 1996, when faced with a large budget shortfall, the Liberal federal government merged the health transfers with the transfers for other social programs into the Canada Health and Social Transfer, and overall funding levels were cut. This placed considerable pressure on the provinces, and combined with population aging and the generally high rate of inflation in health costs, has caused problems with the system.
Private sector
About 27.6% of Canadians' health care is paid for through the private sector. This mostly goes towards services not covered or only partially covered by Medicare, such as prescription drugs, dentistry and optometry. Some 75% of Canadians have some form of supplementary private health insurance; many of them receive it through their employers.[37] There are also large private entities that can buy priority access to medical services in Canada, such as WCB in BC.
The Canadian system is for the most part publicly funded, yet most of the services are provided by private enterprises. Most doctors do not receive an annual salary, but receive a fee per visit or service.[2] According to Dr. Albert Schumacher, former president of the Canadian Medical Association, an estimated 75 percent of Canadian health care services are delivered privately, but funded publicly.
"Frontline practitioners whether they're GPs or specialists by and large are not salaried. They're small hardware stores. Same thing with labs and radiology clinics ...The situation we are seeing now are more services around not being funded publicly but people having to pay for them, or their insurance companies. We have sort of a passive privatization."[2]
"Although there are laws prohibiting or curtailing private health care in some provinces, they can be changed", according to a report in the New England Journal of Medicine.[38][39] In June 2005, the Supreme Court of Canada ruled in Chaoulli v. Quebec (Attorney General) that Quebec's prohibition against private health insurance for medically necessary services laws violated the Quebec Charter of Human Rights and Freedoms, potentially opening the door to much more private sector participation in the health system. Justices Beverley McLachlin, Jack Major, Michel Bastarache and Marie Deschamps found for the majority. "Access to a waiting list is not access to health care", wrote Chief Justice Beverly McLachlin.
The Quebec and federal governments asked the high court to suspend its ruling for 18 months. Less than two months after its initial ruling, the court agreed to suspend its decision for 12 months, retroactive to June 9, 2005.[40]
Physicians and medical organization
Canada, like its North American neighbour the United States, has a ratio of practising physicians to population that is below the OECD average [41] but a level of practising nurses that is higher than either the U.S. or the OECD average.[42]
Family physicians in Canada make an average of $202,000 a year (2006, before expenses).[43] Alberta has the highest average salary of around $230,000, while Quebec has the lowest average annual salary at $165,000, arguably creating interprovincial competition for doctors and contributing to local shortages.[43] In fact, the cost of living in Alberta is considerably higher than the cost of living in Quebec, so absolute income differentials can be massively misleading.
In 1991, the Ontario Medical Association agreed to become a province-wide closed shop, making the OMA union a monopoly. Critics argue that this measure has restricted the supply of doctors to guarantee its members' incomes.[44]
In September 2008, the Ontario Medical Association and the Ontarian government agreed to a new four-year contract that will see doctors receive a 12.25% pay raise. The new agreement is expected to cost Ontarians an extra $1 billion. Referring to the agreement, Ontario premier Dalton McGuinty said,"One of the things that we've got to do, of course, is ensure that we're competitive ... to attract and keep doctors here in Ontario...".[45]
In December 2008, the Society of Obstetricians and Gynaecologists of Canada reported a critical shortage of obstetricians and gynaecologists. The report stated that only 1,370 obstetricians were practicing in Canada and that number is expected to fall by at least one-third within five years. The society is asking the government to increase the number of medical school spots for obstetrics and gynecologists by 30 per cent a year for three years and also recommended rotating placements of doctors into smaller communities to encourage them to take up residence there.[46]
Each province regulates its medical profession through a self-governing College of Physicians and Surgeons, which is responsible for licensing physicians, setting practice standards, and investigating and disciplining its members.
The national doctors association is called the Canadian Medical Association;[47] it describes its mission as "To serve and unite the physicians of Canada and be the national advocate, in partnership with the people of Canada, for the highest standards of health and health care. "[48] Because health care is deemed to be under provincial/territorial jurisdiction, negotiations on behalf of physicians are conducted by provincial associations such as the Ontario Medical Association. The views of Canadian doctors have been mixed, particularly in their support for allowing parallel private financing. The history of Canadian physicians in the development of Medicare has been described by C. David Naylor.[49] Since the passage of the 1984 Canada Health Act, the CMA itself has been a strong advocate of maintaining a strong publicly-funded system, including lobbying the federal government to increase funding, and being a founding member of (and active participant in) the Health Action Lobby (HEAL).[50]
However, there are internal disputes. In particular, some provincial medical associations have argued for permitting a larger private role. To some extent, this has been a reaction to strong cost control; CIHI estimates that 99% of physician expenditures in Canada come from public sector sources, and physicians—particularly those providing elective procedures who have been squeezed for operating room time—have accordingly looked for alternative revenue sources.
One indication of this internal dispute came when Dr. Brian Day of B.C. was elected CMA president in August 2007. Day is the owner of the largest private hospital in Canada and a vocal supporter of increasing private health care in Canada. The CMA presidency rotates among the provinces, with the provincial association electing a candidate who is customarily ratified by the CMA general meeting. Day's selection was sufficiently controversial that he was challenged—albeit unsuccessfully—by another physician. The newspaper story went on to note that "Day said he has never supported the privatization of health care in Canada, and accused his detractors of deliberately distorting his position." [51]
Criticisms
Wait times
Health Canada, a federal department, publishes a series of surveys of the health care system in Canada based on Canadians first-hand experience of the health care system.[52]
Although life-threatening cases are dealt with immediately, some services needed are non-urgent and patients are seen at the next-available appointment in their local chosen facility.
The median wait time in Canada to see a special physician is a little over four weeks with 89.5% waiting less than 90 days.[52]
The median wait time for diagnostic services such as MRI and CAT scans [53] is two weeks with 86.4% waiting less than 90 days.[52]
The median wait time for surgery is four weeks with 82.2% waiting less than 90 days.[52]
Another study by the Commonwealth Fund found that 57% of Canadians reported waiting 30 days (4 weeks) or more to see a specialist, broadly in line with the current official statistics. A quarter (24%) of all Canadians waited 4 hours or more in the emergency room.[54]
Dr. Brian Day was once quoted as saying "This is a country in which dogs can get a hip replacement in under a week and in which humans can wait two to three years."[55] Day gave no source for his two to three years claim. The Canadian Health Coalition has responded succinctly to Day's claims, pointing out that "access to veterinary care for animals is based on ability to pay. Dogs are put down if their owners can’t pay. Access to care should not be based on ability to pay." [56] Regional administrations of Medicare across Canada publish their own wait time data on the internet. For instance in British Columbia the wait time for a hip replacement is currently a little under ten weeks.[57] The CHC is one of many groups across Canada calling for increased provincial and federal funding for medicare and an end to provincial funding cuts as solutions to unacceptable wait times.[58] In a 2007 episode of ABC News's 20/20 titled "Sick in America", host John Stossel cited numerous examples of Canadians who did not get the health care that they needed.[59] The Fraser Institute, a conservative think tank, claims to do its own research and found that treatment time from initial referral by a GP through consultation with a specialist to final treatment, across all specialties and all procedures (emergency, non-urgent, and elective), averaged 17.7 weeks in 2005.[60] However, the report of the Fraser Institute is greatly at odds with the Canadian government's own 2007 report.[61]
Criticisms have been laid during the administration of H1N1 shots in 2009, in parts of Canada, including Hamilton and Toronto. "Wait times for flu shots continued to be hours long yesterday [October 29] as Hamiltonians lined up for the only protection from H1N1 that public health can offer. Waits were about five hours at the clinic on the West Mountain, with 1,000 people in line. The Dundas clinic wasn't much better, with 700 waiting for a shot."[62] "Hundreds of people who lined up in Toronto today were given slips of paper with a time on it so they could return for their vaccination without standing around for hours on end." [63]
Since 2002, the Canadian government has invested $5.5 billion to decrease wait times.[64] In April 2007, Canadian Prime Minister Stephen Harper announced that all ten provinces and three territories would establish patient wait times guarantees by 2010. Canadians will be guaranteed timely access to health care in at least one of the following priority areas, prioritized by each province: cancer care, hip and knee replacement, cardiac care, diagnostic imaging, cataract surgeries or primary care.[65]
Counter-criticism: some longer wait times can benefit patients
It has been observed and found in data that the complete elimination of all waiting times is not ideal. When waiting lists arise through a prioritization process based on physician-determined medical urgency and the procedure's risk, (in contrast to patient's ability to pay or profitability for the physician), waiting lists can possibly help patients. It's been postulated that a system of immediate care can be detrimental for optimal patient outcomes due to avoidance of unnecessary or unproven surgery. An example is the Canadian province of British Columbia, where, according to surgeon Dr. Lawrence Burr, 15 heart patients died in 1990 while on a waiting list for heart surgery. According to Robin Hutchinson, senior medical consultant to the Health Ministry's heart program, had the waiting list not existed and all patients given instant access to the surgery, the expected number of fatalities would have been 22 due to the operation mortality rate at that time. Hutchison noted that the BC Medical Association's media campaign did not make reference to these comparative statistics and only focused on deaths during waiting for surgery.[66]
Since, ideally, waiting lists prioritize higher-risk patients to receive surgery ahead of those with lower risks, this helps reduce overall patient mortality. Consequently, a wealthy or highly-insured patient in a system based on profit or ability to pay (as in the U.S.) may be pushed into surgery or other procedures more quickly, with a result in higher morbidity or mortality risk. This is in addition to the better-understood phenomenon in which lower-income, uninsured, or under-insured patients have their care denied or delayed, also resulting in worse health care.[67]
Restrictions on privately funded health care
The Canada Health Act, which sets the conditions with which provincial/territorial health insurance plans must comply if they wish to receive their full transfer payments from the federal government, does not allow charges to insured persons for insured services (defined as medically necessary care provided in hospitals or by physicians). Most provinces have responded through various prohibitions on such payments. This does not constitute a ban on privately funded care; indeed, about 30% of Canadian health expenditures come from private sources, both insurance and out-of-pocket payments.[68] The Canada Health Act does not address delivery. Private clinics are therefore permitted, albeit subject to provincial/territorial regulations, but they cannot charge above the agreed-upon fee schedule unless they are treating non-insured persons (which may include those eligible under automobile insurance or worker's compensation, in addition to those who are not Canadian residents), or providing non-insured services. This provision has been controversial among those seeking a greater role for private funding.
In 2006, the Government of British Columbia threatened to shut down one private clinic because it was planning to start accepting private payments from patients.[69]
Governments have responded through wait time strategies, discussed above, which attempt to ensure that patients will receive high-quality, necessary services in a timely manner. Nonetheless, the debate continues.
Cross-border health care
The border between Canada and the United States represents a boundary line for medical tourism, in which a country's residents travel elsewhere to seek health care that is more available or affordable.
Canadians visiting the US to receive health care
Some residents of Canada travel to the United States because it provides the nearest facility for their needs. Some do so on quality grounds or because of easier access. A study by Barer, et al., indicates that the majority of Canadians who seek health care in the U.S. are already there for other reasons, including business travel or vacations. A smaller proportion seek care in the U.S. for reasons of confidentiality, including abortions, mental illness, substance abuse, and other problems that they may not wish to divulge to their local physician, family, or employer.
- Canadians offered free care in the US paid by the Canadian government have sometimes declined it. In 1990 the British Columbia Medical Association ran radio ads asking, "What's the longest you'd wait in line at a bank before getting really annoyed? Five minutes? Ten minutes? What if you needed a heart operation?" Following this, the government responded, as summarized by Robin Hutchinson, senior medical consultant for the health ministry's heart program. Despite the medically questionable nature of heart bypass for milder cases of chest pain and follow-up studies showing heart bypass recipients were only 25-40% more likely to be relieved of chest pain than people who stay on heart medicine, the "public outcry" following the ads led the government to take action:
"'We did a deal with the University of Washington at Seattle' said Hutchinton.. to take 50 bypass cases at $18,000 per head, almost $3,000 higher than the cost in Vancouver, with all the money [paid by] the province..In theory, the Seattle operations promised to take the heat off the Ministry of Health until a fourth heart surgery unit opened in the Vancouver suburb of New Westminster. If the first batch of Seattle bypasses went smoothly..then the government planned to buy three or four more 50-head blocks. But four weeks after announcing the plan, health administrators had to admit they were stumped. 'As of now..we've have nine people sign up. The opposition party, the press, everybody's making a big stink about our waiting lists. And we've got [only] nine people signed up! The surgeons ask their patients and they say, "I'd rather wait", We thought we could get maybe two hundred and fifty done down in Seattle..but if nobody wants to go to Seattle, we're stuck,'".[67]
- In a Canadian National Population Health Survey of 17,276 Canadian residents, it was reported that only 0.5% sought medical care in the US in the previous year. Of these, less than a quarter had traveled to the U.S. expressly to get that care.[70]
- A 2002 study by Katz, Cardiff, et al., reported the number of Canadians using U.S. services to be "barely detectible relative to the use of care by Canadians at home" and that the results "do not support the widespread perception that Canadian residents seek care extensively in the United States."[71]
- According to a September 14, 2007, article from CTV News, Canadian Liberal MP Belinda Stronach went to the United States for breast cancer surgery in June 2007. Stronach's spokesperson Greg MacEachern was quoted in the article saying that the US was the best place to have this type of surgery done. Stronach paid for the surgery out of her own pocket.[72] Prior to this incident, Stronach had stated in an interview that she was against two-tier health care.[73]
- When Robert Bourassa, the premier of Quebec, needed cancer treatment, he went to the US to get it.[74]
- In 2007, it was reported that Canada sent scores of pregnant women to the US to give birth.[75] In 2007 a woman from Calgary who was pregnant with quadruplets was sent to Great Falls, Montana to give birth. An article on this incident states there were no Canadian hospitals with enough neo-natal intensive beds to accommodate the extremely rare quadruple birth.[76]
- A January 19, 2008, article in The Globe and Mail states, "More than 150 critically ill Canadians – many with life-threatening cerebral hemorrhages – have been rushed to the United States since the spring of 2006 because they could not obtain intensive-care beds here. Before patients with bleeding in or outside the brain have been whisked through U.S. operating-room doors, some have languished for as long as eight hours in Canadian emergency wards while health-care workers scrambled to locate care." [77]
- In 2010, Newfoundland and Labrador Premier Danny Williams traveled to the US for heart surgery.[78]
In 2005 Shona Holmes of Waterdown, Ontario, traveled to the Mayo Clinic after deciding she couldn't afford to wait for appointments with specialists through the Ontario health care system.[79][80] She has characterized her condition as an emergency, said she was losing her sight, and portrayed her condition as life-threatening brain cancer. OHIP did not reimburse her for her medical expenses. In 2007 she joined a lawsuit to force the Ontario government to reimburse patients who feel they had to travel outside of Canada for timely, life-saving medical treatment. In July 2009 Holmes agreed to appear in television ads broadcast in the United States warning Americans of the dangers of adopting a Canadian style health care system. After her ad appeared critics pointed out discrepancies in her story, including that Rathke's cleft cyst, the condition she was treated for, was not a form of cancer, and was not life-threatening.[81][82] In fact, the mortality rate for patients with a Rathke's cleft cyst is zero percent. [83]
US citizens visiting Canada to receive health care
On the other hand, some US citizens travel to Canada for health-care related reasons:
- Many US citizens purchase prescription drugs from Canada, either over the Internet or by traveling there to buy them in person, because prescription drug prices in Canada are substantially lower than prescription drug prices in the United States; this cross-border purchasing has been estimated at $1 billion annually.[84]
- Because medical marijuana is legal in Canada but illegal in most of the US, many US citizens suffering from cancer, AIDS, multiple sclerosis, and glaucoma have traveled to Canada for medical treatment. One of those is Steve Kubby, the Libertarian Party's 1998 candidate for governor of California, who is suffering from adrenal cancer.[85] Recent legal changes such as Proposition 215 may decrease this type of medical tourism from California only.
- Sarah Palin, in an appearance in Calgary, told her audience that her family once used the Canadian health-care system,[86] before the Canada Health Act although she says it was in the 60s, when the Canadian healthcare system was beginning to reform.
Comparison to other countries
Main article: Comparison of Canadian and American health care systemsThe Canadian health care system is often compared to the US system. The US system spends the most in the world per capita, and was ranked 37th in the world by the World Health Organization in 2000, while Canada's health system was ranked 30th. The relatively low Canadian WHO ranking has been criticized by some[who?] for its choice of ranking criteria and statistical methods, and the WHO is currently revising its methodology and withholding new rankings until the issues are addressed.[87][88]
Canada spent approximately 10.0% of GDP on health care in 2006, more than one percentage point higher than the average of 8.9% in OECD countries.[89] According to the Canadian Institute for Health Information, spending is expected to reach $160 billion, or 10.6% of GDP, in 2007.[90] This translates to $4,867 per person.
Most health statistics in Canada are at or above the G8 average.[91] Direct comparisons of health statistics across nations is complex. The OECD collects comparative statistics, and has published brief country profiles.[92][93][94]
Country Life expectancy Infant mortality rate Physicians per 1000 people Nurses per 1000 people Per capita expenditure on health (USD) Healthcare costs as a percent of GDP % of government revenue spent on health % of health costs paid by government Australia 81.4 4.2 2.8 9.7 3,137 8.7 17.7 67.7 Canada 81.3 4.5 2.2 9.0 3,895 10.1 16.7 69.8 France 81.0 4.0 3.4 7.7 3,601 11.0 14.2 79.0 Germany 79.8 3.8 3.5 9.9 3,588 10.4 17.6 76.9 Japan 82.6 2.6 2.1 9.4 2,581 8.1 16.8 81.3 Sweden 81.0 2.5 3.6 10.8 3,323 9.1 13.6 81.7 UK 79.1 4.8 2.5 10.0 2,992 8.4 15.8 81.7 US 78.1 6.9 2.4 10.6 7,290 16.0 18.5 45.4 See also
- Health care compared - tabular comparisons of the US, Canada, and other countries not shown above.
- Canada Health Act
- Canada Health Transfer
- Canada Health and Social Transfer
- Indian Health Transfer Policy (Canada)
- Canada's Health Care providers, 2007
- Royal Commission on the Future of Health Care in Canada
- Canadian and American health care systems compared
- Medicare (Canada)
- Health Evidence Network of Canada
- Suicide in Canada
References
- ^ http://www.civilization.ca/cmc/exhibitions/hist/medicare/medic-5h23e.shtml
- ^ a b c Public vs. private health care CBC, December 1, 2006.
- ^ "Overview of the Canada Health Act". http://www.hc-sc.gc.ca/hcs-sss/medi-assur/cha-lcs/overview-apercu-eng.php.
- ^ http://www.health.gov.bc.ca/msp/infoben/premium.html#monthly
- ^ "Provincial/Territorial Role in Health". http://www.hc-sc.gc.ca/hcs-sss/delivery-prestation/ptrole/index-eng.php.
- ^ CIHI p.91
- ^ "Public health care scores big in poll as MDs study privatization". Healthzone.ca. 2009-08-12. http://www.healthzone.ca/health/article/679824. Retrieved 2011-02-10.
- ^ "Canada overwhelmingly supports public health care". Nupge.ca. 2009-08-13. http://www.nupge.ca/node/2486. Retrieved 2011-02-10.
- ^ "Never mind the anecdotes: Do Canadians like their health-care system?". Chicago Tribune. 2009-08-06. http://blogs.chicagotribune.com/news_columnists_ezorn/2009/08/never-mind-the-anecdotes-do-canadians-like-their-health-care-system.html. Retrieved 2011-02-10.
- ^ "Canadians prefer Obama over own leaders: poll - CTV News". CTV.ca. 2008-06-29. http://www.ctv.ca/servlet/ArticleNews/story/CTVNews/20080629/poll_us_canada_080629/20080629?hub=Politics. Retrieved 2011-02-10.
- ^ "Never mind the anecdotes: Do Canadians like their health-care system?". Chicago Tribune. 2009-08-06. http://blogs.chicagotribune.com/news_columnists_ezorn/2009/08/never-mind-the-anecdotes-do-canadians-like-their-health-care-system.html.
- ^ "Healthcare System Ratings: U.S., Great Britain, Canada". Gallup.com. http://www.gallup.com/poll/8056/healthcare-system-ratings-us-great-britain-canada.aspx. Retrieved 2011-02-10.
- ^ CIHI p.119
- ^ a b c d CIHI p.xiv
- ^ CIHI pg. 119
- ^ a b "www.cbc.ca". CBC News. 2009-11-19. http://www.cbc.ca/health/story/2009/11/19/health-care-spending-canada.html.
- ^ CIHI p.24
- ^ CIHI p.55
- ^ CIHI p.20
- ^ CIHI p.112-113
- ^ a b CIHI p.xiii
- ^ "Ontario Ministry of Health and Long-Term Care - Public Information - Ontario Health Insurance Plan - Ohip Facts - Ambulance Services Billing". http://www.health.gov.on.ca/english/public/pub/ohip/amb.html.
- ^ Ministry of Health and Long-term Care, Ontario website available at
- ^ MacInnes JK, McAlister VC. Myopia of healthcare reform using business models. Ann R Coll Physicians Surg Can 2001; 34: 20-2. Available at [1]
- ^ Shah, Chandrakant P (2003). Public health and preventive medicine in Canada (5th ed.). Toronto: Elsevier Canada.
- ^ [Marchildon GP. Health Systems in Transition: Canada. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies. Downloaded from http://www.euro.who.int/Document/E87954.pdf].
- ^ Warren, P. (2008). "Physician advocacy essential for Canada's First Nations". Canadian Medical Association Journal 179 (7): 728. doi:10.1503/cmaj.081290. PMC 2535741. PMID 18809906. http://www.cmaj.ca/cgi/content/full/179/7/728. Retrieved 2011-02-10.
- ^ The Discovery of Insulin, 25th Anniversary Edition, by Michael Bliss, Chicago, ISBN 978-0-226-05899-3
- ^ "The Nobel Prize in Physiology or Medicine 1923". Nobelprize.org. http://nobelprize.org/nobel_prizes/medicine/laureates/1923/. Retrieved 2011-02-10.
- ^ "History". Alberta Medical Association. http://www.albertadoctors.org/bcm/ama/ama-website.nsf/0/72D6C5EEBCA2CA9787256E1C0056E7A8?OpenDocument. Retrieved 2011-02-10.
- ^ Turner, JG (1958). "The Hospital Insurance and Diagnostic Services Act: Its Impact on Hospital Administration". Canadian Medical Association journal 78 (10): 768–70. PMC 1829926. PMID 13523526. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1829926.
- ^ Government of Canada, Social Union, News Release, "A Framework to Improve the Social Union for Canadians: An Agreement between the Government of Canada and the Governments of the Provinces and Territories, February 4, 1999." Retrieved 20 December 2006.
- ^ CIHI
- ^ Silversides, Ann (October 23, 2007). "The North "like Darfur"". Canadian Medical Association Journal 9 (177): 1013–4. doi:10.1503/cmaj.071359. PMC 2025628. PMID 17954876. http://www.cmaj.ca/cgi/content/full/177/9/1013.
- ^ Gao, Song; et al. (November 4, 2008). "Access to health care among status Aboriginal people with chronic kidney disease". Canadian Medical Association Journal 10 (179): 1007–12. doi:10.1503/cmaj.080063. PMC 2572655. PMID 18981441. http://www.cmaj.ca/cgi/content/full/179/10/1007.
- ^ Peiris, David; Alex Brown, BMed MPH and Alan Cass, MBBS PhD (November 4, 2008). "Addressing inequities in access to quality health care for indigenous people". Canadian Medical Association Journal 10 (179): 985–6. doi:10.1503/cmaj.081445. PMC 2572646. PMID 18981431. http://www.cmaj.ca/cgi/content/full/179/10/985.
- ^ Private Health Insurance in OECD Countries OECD Health Project, 2004. Retrieved January 21, 2008.
- ^ "Private Health Care in Canada, Robert Steinbrook, N Engl J Med, 354:1661-1664, April 20, 2006". Content.nejm.org. 1970-01-01. http://content.nejm.org/cgi/content/full/354/16/1661. Retrieved 2011-02-10.
- ^ Kraus, Clifford (2006-02-26). "As Canada's Slow-Motion Public Health System Falters, Private Medical Care Is Surging". New York Times. http://www.nytimes.com/2006/02/26/international/americas/26canada.html?ex=1184644800&en=44cca772dc339429&ei=5070. Retrieved 2007-07-16.
- ^ "CBC News Indepth: Health Care". CBC News. http://www.cbc.ca/news/background/healthcare/2005scc035decision.html.
- ^ "OECD data. Number of practising physicians". Titania.sourceoecd.org. http://titania.sourceoecd.org/vl=4012838/cl=17/nw=1/rpsv/health2007/g4-2-01.htm. Retrieved 2011-02-10.
- ^ "SourceOECD: OECD Health 2007". Titania.sourceoecd.org. http://titania.sourceoecd.org/vl=4012838/cl=17/nw=1/rpsv/health2007/g4-3-01.htm. Retrieved 2011-02-10.
- ^ a b "Que. doctors lagging in fee-for-service payments". Ctv.ca. 2006-12-21. http://www.ctv.ca/servlet/ArticleNews/story/CTVNews/20061221/quebec_doctors_061221?s_name=&no_ads=. Retrieved 2011-02-10.
- ^ Terence Corcoran (November 6). "ONTARIO DOCTORS SOLD OUT AGAIN". National Post. http://64.233.169.104/search?q=cache:_UP9BMpiPOIJ:www.cofp.com/documents/2004Nov9NPCorcoranArticleDoctorsSoldOutAgain.pdf+doctor+shortage+in+Canada+created+by+doctors+union&hl=en&ct=clnk&cd=9. Retrieved 2011-02-10.
- ^ "Ont. doctors get 12.25 per cent wage hike". http://www.ctv.ca/servlet/ArticleNews/story/CTVNews/20080915/doctors_wage_080915/20080915?hub=Health. Retrieved 2008-09-15.
- ^ "Obstetrician shortage endangers moms, babies: report says". CTV.ca. 2008-12-05. http://www.ctv.ca/servlet/ArticleNews/story/CTVNews/20081205/ob_shortage_081205/20081205?hub=Health.
- ^ "Canadian Medical Association". Cma.ca. http://www.cma.ca/index.cfm/ci_id/121/la_id/1.htm. Retrieved 2011-02-10.
- ^ "About CMA". Cma.ca. 2010-03-24. http://www.cma.ca/index.cfm/ci_id/44413/la_id/1.htm. Retrieved 2011-02-10.
- ^ Naylor, C David (1986). Private Practice, Public Payment: Canadian Medicine and the Politics of Health Insurance 1911-1966. Kingston, Ontario: McGill-Queen's University Press.
- ^ "HEAL home page". Physiotherapy.ca. http://www.physiotherapy.ca/HEAL/english/index.htm. Retrieved 2011-02-10.
- ^ "CBC Private health-care advocate wins CMA presidency". CBC.ca. 2006-08-22. http://www.cbc.ca/canada/prince-edward-island/story/2006/08/22/day-cma-president.html. Retrieved 2011-02-10.
- ^ a b c d "Healthy Canadians: Canadian government report on comparable health care indicators". http://www.healthcoalition.ca/index-eng.pdf.
- ^ Diagnostic tests defined as the following: non-emergency magnetic resonance imaging (MRI) devices; computed tomography (CT or CAT) scans; and angiographies that use X-rays to examine the inner opening of blood-filled structures such as veins and arteries.
- ^ Commonwealth Fund, "Mirror, Mirror on the Wall: An International update on the comparative performance of American health care", Karen Davis et al., May 15, 2007.
- ^ Krauss, Clifford (2006-02-28). "Canada's Private Clinics Surge as Public System Falters". The New York Times. http://www.nytimes.com/2006/02/28/international/americas/28canada.html?ei=5090&en=ad12dcee61e8b584&ex=1298782800&partner=rssuserland&emc=rss&pagewanted=print. Retrieved 2010-05-04.
- ^ [2][dead link]
- ^ Provincial Median Wait Times in British Columbia - mostly 6 weeks or less[dead link]
- ^ "Ontario Health Coalition - Home". Web.net. http://www.web.net/ohc/index.html. Retrieved 2011-02-10.
- ^ 20/20, "Sick in America", ABC News, 2007
- ^ "Hidden costs of Canada's Health Care System". Independent.org. 2004-04-23. http://www.independent.org/newsroom/article.asp?id=1292. Retrieved 2011-02-10.
- ^ "Wait Times Tables A Comparison by Province 2007" (PDF). http://www.cihi.ca/cihiweb/en/downloads/aib_provincial_wait_times_e.pdf. Retrieved 2011-02-10.
- ^ http://www.thespec.com/News/Local/article/663360
- ^ http://www.thespec.com/News/BreakingNews/article/663640
- ^ Waiting for access, CBC News: In Depth: Health Care, November 29, 2006. Retrieved November 19, 2007.
- ^ Media release Canada’s New Government announces Patient Wait Times Guarantees, Office of the Prime Minister, April 4, 2007. Retrieved November 19, 2007.
- ^ Schmitz, Anthony (January/February 1991). "Health Assurance". In Health 5 (1): pp. 39–47. http://www.healthadvocates.info/HealthAssurance.pdf.
- ^ a b Schmitz, Anthony (January/February 1991). "Health Assurance". In Health 5 (1): pp. 39–47. http://www.healthadvocates.info/HealthAssurance.pdf.
- ^ Canadian Institute for Health Information (September 27, 2005). CIHI exploring the 70-30 split. Ottawa, Ont.: Canadian Institute for Health Information. ISBN 1-55392-655-2. http://www.cihi.ca/cihiweb/dispPage.jsp?cw_page=AR_1282_E. Retrieved 2007-12-21.
- ^ Cernetig, Miro (2006-12-01). "B.C. gov't gets tough with private clinic". Vancouver Sun (CanWest News Service). http://www.canada.com/topics/news/story.html?id=16141a15-58d5-4e05-a1d2-78eaaeae207a&k=29315. Retrieved 2008-01-09.[3]
- ^ [4] Canadian National Population Health Survey study
- ^ Katz, S. J.; Cardiff, K.; Pascali, M.; Barer, M. L.; Evans, R. G. (2002). "Phantoms in the Snow: Canadians' Use of Health Care Services in the United States". Health Affairs 21 (3): 19–31. doi:10.1377/hlthaff.21.3.19. PMID 12025983. http://content.healthaffairs.org/cgi/content/full/21/3/19.
- ^ "Stronach went to U.S. for cancer treatment: report". CTV.ca. 2007-09-14. http://www.ctv.ca/servlet/ArticleNews/story/CTVNews/20070914/belinda_Stronach_070914/20070914?hub=TopStories. Retrieved 2011-02-10.
- ^ "CBC News: Sunday - Belinda Stronach Interview". http://www.cbc.ca/sunday/coverstory_stronach.html.[dead link]
- ^ Rationing Health Care: Price Controls Are Hazardous to Our Health The Independent Institute, February 1, 1994
- ^ "Some Canadian mothers forced to give birth in U.S. | KOMO-TV - Seattle, Washington | News". Komo-Tv. 2010-04-01. http://www.komotv.com/news/10216201.html. Retrieved 2011-02-10.
- ^ Calgary, The (2007-08-17). "Calgary's quads: Born in the U.S.A". Canada.com. http://www.canada.com/calgaryherald/story.html?id=41ccae74-8325-449a-b89f-e68957ca25ae&k=79546. Retrieved 2011-02-10.
- ^ Canada (2008-01-19). "Health". Toronto: Globe and Mail. http://www.theglobeandmail.com/servlet/story/RTGAM.20080119.neuro191/BNStory/specialScienceandHealth/home. Retrieved 2011-02-10.
- ^ Heart surgery to sideline N.L. premier for weeks, CBC News, February 2, 2010
- ^ Tanya Talaga (2007-09-06). "Patients suing province over wait times: Man, woman who couldn't get quick treatment travelled to U.S. to get brain tumours removed". Toronto Star. Archived from the original on 2009-08-07. http://www.webcitation.org/query?url=http%3A%2F%2Fwww.thestar.com%2FNews%2Farticle%2F253664&date=2009-08-07. Retrieved 2009-07-27. "Lindsay McCreith, 66, of Newmarket and Shona Holmes, 43, of Waterdown filed a joint statement of claim yesterday against the province of Ontario. Both say their health suffered because they are denied the right to access care outside of Ontario's "government-run monopolistic" health-care system. They want to be able to buy private health insurance."
- ^ Sam Solomon (2007-09-30). "New lawsuit threatens Ontario private care ban: "Ontario Chaoulli" case seeks to catalyze healthcare reform". National Review of Medicine 4 (16). Archived from the original on 2009-08-07. http://www.webcitation.org/query?url=http%3A%2F%2Fwww.nationalreviewofmedicine.com%2Fissue%2F2007%2F09_30%2F4_policy_politics02_16.html&date=2009-08-07. Retrieved 2009-07-27.
- ^ "Anti-medicare ad an exaggeration: experts". CBC News. 2009-07-31. Archived from the original on 2009-08-07. http://www.webcitation.org/query?url=http%3A%2F%2Fwww.cbc.ca%2Fhealth%2Fstory%2F2009%2F07%2F31%2Fmedicare-ad-exaggeration523.html&date=2009-08-07. Retrieved 2009-08-07.
- ^ Ian Welsh (2009-07-21). "Americans Lives vs. Insurance Company Profits: The Real Battle in Health Care Reform". Huffington Post. Archived from the original on 2009-08-07. http://www.webcitation.org/query?url=http%3A%2F%2Fwww.huffingtonpost.com%2Fian-welsh%2Famericans-lives-vs-insura_b_241703.html&date=2009-08-07. Retrieved 2009-07-21.
- ^ Omar Islam, MD, FRCP(C) (2008-03-27). Rathke Cleft Cyst. Medscape. http://emedicine.medscape.com/article/343629-overview. Retrieved 2009-11-22
- ^ Morgan, S.; Morgan, Steven and Hurley, Jeremiah (2004-03-16). "Internet pharmacy: prices on the up-and-up". CMAJ 170 (6): 945–946. doi:10.1503/cmaj.104001. PMC 359422. PMID 15023915. http://www.cmaj.ca/cgi/content/full/170/6/945?etoc. Retrieved 2007-07-11.
- ^ US cannabis refugees cross border The Guardian July 20, 2002
- ^ "Palin Crossed Border For Canadian Health Care". The Huffington Post. http://www.huffingtonpost.com/2010/03/08/palin-crossed-border-for_n_490080.html. Retrieved 2011-02-10.
- ^ Phyllida Brown (2002-01-26). "WHO to revise its method for ranking health systems". BMJ 324 (7331): 190b. doi:10.1136/bmj.324.7331.190b. http://www.bmj.com/cgi/content/full/324/7331/190/b. Retrieved 2011-02-10.
- ^ Deber, Raisa (2004-03-15). "Why Did the World Health Organization Rate Canada's Health System as 30th? Some Thoughts on League Tables". Longwoods Review 2 (1). http://www.longwoods.com/product.php?productid=17238. Retrieved 2008-01-09. "The measure of "overall health system performance" derives from adjusting "goal attainment" for educational attainment. Although goal attainment is in theory based on five measures (level and distribution of health, level and distribution of "responsiveness" and "fairness of financial contribution"), the actual values assigned to most countries, including Canada, were never directly measured. The scores do not incorporate any information about the actual workings of the system, other than as reflected in life expectancy. The primary reason for Canada's low standing rests on the high educational level of its population, particularly as compared to France, rather than on any features of its health system."
- ^ OECD Health Data 2007: How Does Canada Compare, OECD, July 2007. Retrieved February 2, 2009.
- ^ Media release, Health care spending to reach $160 billion this year, Canadian Institute for Health Information, November 13, 2007. Retrieved November 19, 2007.
- ^ ""Health Care: The Romanow Report - By the Numbers" (Saturday, Feb. 4, 2006) globeandmail.com - Canada's best source for news continuously updated from The Globe and Mail". Toronto: The Globe and Mail. 2006-02-04. http://v1.theglobeandmail.com/special/romanow/stories/numbers.html. Retrieved 2011-02-10.
- ^ Organisation for Economic Co-operation and Development. "OECD Health Data 2008: How Does Canada Compare" (PDF). http://www.oecd.org/dataoecd/46/33/38979719.pdf. Retrieved 2009-01-09.
- ^ "Updated statistics from a 2009 report". Organization for Economic Co-Operation and Development. 2010-09-28. http://www.oecd.org/document/46/0,3343,en_2649_34631_34971438_1_1_1_1,00.html. Retrieved 2011-02-10.
- ^ "OECD Health Data 2009 - Frequently Requested Data". Organization for Economic Co-Operation and Development. 2010-09-28. http://www.oecd.org/document/16/0,3343,en_2649_34631_2085200_1_1_1_1,00.html. Retrieved 2011-02-10.
- Bibliography
- Caulfield, Timothy A; Von Tigerstrom, Barbara (2002). Health care reform & the law in Canada: meeting the challenge. University of Alberta Press. ISBN 0888643667. http://books.google.ca/books?id=_q0O2RjAO84C&lpg=PA37&dq=Canada%20Health%20Act&pg=PP1#v=onepage&q&f=true.
- Fierlbeck, Katherine (2011). Health Care in Canada: A Citizen's Guide to Policy and Politics. University of Toronto Press. ISBN 978-1-4426-0983-9. http://books.google.com/books?id=K-cvzH07VCUC&pg=PP1.
- Jacobs, Philip; Jonsson, Egon; Rapoport, John (2008). Cost Containment and Efficiency in National Health Systems : A Global Comparison. Wiley-VCH. ISBN 9783527321100. http://books.google.ca/books?id=gk6PhLacH3wC&lpg=PA19&dq=Health%20care%20in%20Canada&pg=PP1#v=onepage&q&f=true.
- Institute, John Deutsch (2006). Study of Economic Policy Health Services Restructuring in Canada Conference. Economic Policy, Queen's University. ISBN 9781553390756. http://books.google.ca/books?id=8KvGkTvjH1oC&lpg=PR1&dq=Health%20care%20in%20Canada&pg=PR1#v=onepage&q&f=true.
- Marchildon, Gregory P (2006). Health systems in transition : Canada. University of Toronto Press. ISBN 9780802094001. http://books.google.ca/books?id=mGGcyOSrESEC&lpg=PP1&dq=Health%20care%20in%20Canada&pg=PP1#v=onepage&q&f=true.
- Raphael, Dennis (2007). Poverty and Policy in Canada: Implications for Health and Quality of Life. Canadian Scholars' Press. ISBN 9781551303239. http://books.google.ca/books?id=P15Ye7AcS34C&lpg=PA288&dq=Gun%20policies%20in%20Canada&pg=PP1#v=onepage&q&f=true
- Mullner, Ross M (2009). Encyclopedia of health services research. SAGE. pp. 559–562. ISBN 9781412971942. http://books.google.ca/books?id=MUItoTour5oC&pg=PA559&dq=Canada+Health+Act#v=onepage&q&f=true.
- "secure.cihi.ca" (PDF). Canadian Institute for Health Information. http://secure.cihi.ca/cihiweb/products/National_health_expenditure_trends_1975_to_2009_en.pdf.
External links
- Canadian Federalism and Public Health Care: The Evolution of Federal-Provincial Relations | Mapleleafweb.com
- CBC Digital Archives — The Birth of Medicare
- Canadian Health Services Research Foundation
- Data from the Canadian Institute for Health Information
Health care in North America Sovereign states - Antigua and Barbuda
- Bahamas
- Barbados
- Belize
- Canada
- Costa Rica
- Cuba
- Dominica
- Dominican Republic
- El Salvador
- Grenada
- Guatemala
- Haiti
- Honduras
- Jamaica
- Mexico
- Nicaragua
- Panama
- Saint Kitts and Nevis
- Saint Lucia
- Saint Vincent and the Grenadines
- Trinidad and Tobago
- United States
Dependencies and
other territories- Anguilla
- Aruba
- Bermuda
- Bonaire
- British Virgin Islands
- Cayman Islands
- Curaçao
- Greenland
- Guadeloupe
- Martinique
- Montserrat
- Puerto Rico
- Saint Barthélemy
- Saint Martin
- Saint Pierre and Miquelon
- Saba
- Sint Eustatius
- Sint Maarten
- Turks and Caicos Islands
- United States Virgin Islands
Categories:- Healthcare in Canada


Wikimedia Foundation. 2010.