- Visceral leishmaniasis
-
Visceral leishmaniasis Classification and external resources 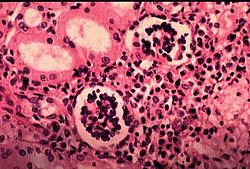
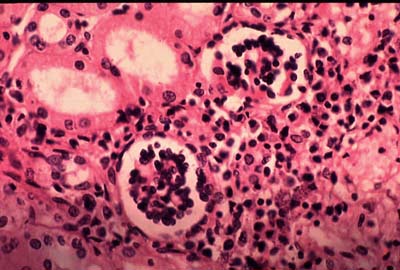
Amastigotes in a chorionic villusICD-10 B55.0 ICD-9 085.0 DiseasesDB 7070 eMedicine emerg/296 MeSH D007898 Visceral leishmaniasis (VL), also known as kala-azar, black fever, and Dumdum fever,[1]:426 is the most severe form of leishmaniasis. Leishmaniasis is a disease caused by protozoan parasites of the Leishmania genus. This disease is the second-largest parasitic killer in the world (after malaria), responsible for an estimated 500,000 cases each year worldwide.[2] The parasite migrates to the internal organs such as liver, spleen (hence 'visceral') and bone marrow, and, if left untreated, will almost always result in the death of the host. Signs and symptoms include fever, weight loss, mucosal ulcers, fatigue, anemia and substantial swelling of the liver and spleen. Of particular concern, according to the World Health Organization (WHO), is the emerging problem of HIV/VL co-infection.[3]
Contents
Species that give rise to VL
Several species of Leishmania are known to give rise to the visceral form of the disease. The "Old World" (Africa, Asia, Europe) species are L. donovani and L. infantum and the "New World" (South America) species is L. chagasi.
Life-cycle of the parasite
Visceral leishmaniasis (Kala-azar) is spread through an insect vector, the sandfly of the Phlebotomus genus in the Old World and the Lutzomyia genus in the New World. Sandflies are tiny creatures, 3-6 millimeters long by 1.5-3 millimeters in diameter, and found in tropical or temperate regions throughout the world. Sandfly larvae grow in warm, moist organic matter, such as old trees, house walls or waste — making them hard to eradicate.
The adult female sand fly is a bloodsucker, usually feeding at night on sleeping prey. When the fly bites an animal infected with L. donovani, the pathogen is ingested along with the prey’s blood. At this point the protozoan is in the smaller of its two forms, called an amastigote — round, non-motile, and only three to seven micrometers in diameter.
Taken into the stomach of the sandfly, the amastigotes quickly transform into a second L. donovani form, called the promastigote. This form is spindle-shaped, triple the size of the amastigote, and has a single flagellum that allows for motility. The promastigotes live extracellularly in the sandfly’s alimentary canal, reproducing asexually, then migrate to the proximal end of the gut where they become poised for a regurgitational transmission. This is their means of transmission back into a mammalian host, as the fly injects its saliva into prey when it bites. The promastigotes are introduced locally at the bite site along with the fly’s saliva.
Once inside the new host, promastigotes invade macrophages. Once inside, they transform back into the smaller amastigote form. As an amastigote, L. donovani can only reproduce intracellularly — and the amastigotes replicate in the most hostile part of the macrophage cell, inside the phagolysosome, whose normal defensive response they are able to prevent. After they have reproduced to a certain extent, the L. donovani lyse their host cell by sheer pressure of mass, but there is some recent speculation that they are able to leave the cell by triggering the exocytosis response of the macrophage. The daughter cell protozoans then migrate through the bloodstream to find new macrophage hosts. In time, L. donovani becomes a systemic infection, spreading to all the host’s organs, particularly the spleen and liver.
Disease progression
In human hosts, response to infection by L. donovani varies a great deal, not only by the strength but also by the type of the patient’s immune reaction. People with a history of infection by strains of leishmania that cause visceral leishmaniasis show a continuum of immune responses from protective to non-protective. Those who acquired protective immunity (skin test positive) without ever having visceral leishmaniasis have a strong type 1 CD4+ response to leishmania antigens. Antigen specific interferon-gamma and proliferation, as well as the ability to kill intracellular leishmania, are hallmarks of protective immunity.[4,5] Because visceral leishmaniasis patients lack these responses to leishmania and other antigens, they usually die of secondary infections unless treated. In addition, increased interleukin-10 secretion is characteristic of the disease[6-8]. Addition of interleukin-12, anti-interleukin-10, or anti-interleukin-4 to peripheral blood mononuclear cells from acute patients sometimes increases interferon-gamma secretion and proliferation.[9-11] Acute patient peripheral blood mononuclear cells include CD8+ T regulatory cells that decrease interferon-gamma secretion and proliferation responses to leishmania and other antigens and increase interleukin-10 secretion when added to autologous peripheral blood mononuclear cells harvested after successful treatment.[8,12] Thus, the CD8+ T regulatory cells reproduce the immune response characteristic of visceral leishmaniasis. CD8+ T regulatory cells are also associated with post kala azar dermal leishmaniasis.[13] Addition of interleukin-12 or interferon-gamma does not prevent CD8+ T regulatory activity. The dominance of type 1 CD4+ T cells in skin test positive adults maybe explained by their secretion of factors that inhibit and kill CD8+ T regulatory cells.[11,12] Successfully treated patients rarely develop visceral leishmaniasis a second time. Their peripheral blood mononuclear cells show a mixed T1/T2 CD4+ and CD8+ T suppressor response but do have the ability to kill intracellular leishmania.[4,12,14]
When a human patient does develop visceral leishmaniasis, the most typical symptoms are fever and the enlargement of the spleen, or splenomegaly, with enlargement of the liver — hepatomegaly — sometimes being seen as well. The blackening of the skin that gave the disease its common name in India does not appear in most strains of the disease, and the other symptoms are very easy to mistake for those of malaria. Mis-diagnosis is dangerous, as without proper treatment the mortality rate for kala-azar is close to 100%. L. donovani itself is not usually the direct cause of death in kala-azar sufferers, however. Pneumonia, tuberculosis and dysentery are omnipresent in the depressed regions where leishmaniasis thrives, and, as with AIDS, it is these opportunistic infections that are more likely to kill, flaring up in a host whose immune system has been weakened by the L. donovani infection. Progress of the disease is extremely variable, taking anywhere from one to twenty weeks, but a typical duration for the Sudanese strain of the disease is narrower, between twelve and sixteen weeks.
Even with recovery, kala-azar does not always leave its hosts unmarked. Some time after successful treatment—generally a few months with African kala-azar, or as much as several years with the Indian strain—a secondary form of the disease may set in, called post kala-azar dermal leishmaniasis, or PKDL. This condition manifests first as small, measle-like skin lesions on the face, which gradually increase in size and spread over the body. Eventually the lesions may coalesce to form disfiguring, swollen structures resembling leprosy, and occasionally causing blindness if they spread to the eyes. (This disease is not the same as cutaneous leishmaniasis, a milder disease caused by another protozoan of the Leishmania genus which also causes skin lesions.)
Diagnosis
The gold standard for diagnosis is visualization of the amastigotes in splenic aspirate or bone marrow aspirate. This is a technically challenging procedure that is frequently unavailable in areas of the world where visceral leishmaniasis is endemic.
Serological testing is much more frequently used in areas where leishmaniasis is endemic. The K39 dipstick test is easy to perform, and village health workers can be easily trained to use it. The kit may be stored at ambient temperature and no additional equipment needs to be carried to remote areas. The DAT anti-leishmania antigen test is standard within MSF is much more cumbersome to use and appears not to have any advantages over the K39 test.[15]
There are a number of problems with serological testing: in highly endemic areas, not everyone who becomes infected will actually develop clinical disease or require treatment. Indeed, up to 32% of the healthy population may test positive, but not require treatment.[16][17] Conversely, because serological tests look for an immune response and not for the organism itself, the test does not become negative after the patient is cured, it cannot be used as a check for cure, or to check for re-infection or relapse.[18] Likewise, patients with abnormal immune systems (e.g., HIV infection) will have false-negative tests.[19]
Other tests being developed include a latex agglutination test (KAtex), which is currently being tested in Asia and Africa. Another potential test detects erythrosalicylic acid.[18]
Treatments
As with many diseases in developing nations, (including trypanosomiasis and malaria) effective and affordable chemotherapy is sorely lacking and parasites or insect vectors are becoming increasingly resistant to existing anti-parasite drugs. Presumably due to the lack of financial return, new drugs are slow to emerge and much of the basic research into potential drug targets takes place in universities, funded by charitable organisations. This may change as a result of infection of members of the armed forces from the developed nations that currently occupy nations such as Afghanistan and Iraq, where Leishmania is commonplace.
The traditional treatment is with pentavalent antimonials such as sodium stibogluconate and meglumine antimoniate. Resistance is now common in India, and rates of resistance have been shown to be as high as 60% in parts of Bihar, India.[20][21]
The Indian medical practitioner, Upendra Nath Brahmachari, was nominated for the Nobel Prize in Physiology or Medicine in 1929 for his discovery of ureastibamine (an antimonial compound for the treatment of kala-azar) and a new disease, post kala-azar dermal leishmaniasis.[22] Brahmachari's cure for visceral leishmaniasis was the urea salt of para-amino-phenyl stibnic acid which he called Urea Stibamine.[23]
The treatment of choice for visceral leishmaniasis acquired in India is now Amphotericin B[24] in its various liposomal preparations (AmBisome,[25] Abelcet, Amphocil[26])
- AmBisome dose: total dose 21 mg/kg (Mediterranean/Brazilian VL); total dose 7.5 mg/kg over 6 days (Indian VL)
- Amphocil dose: total dose 7.5 mg/kg over 6 days (Indian VL)
A low dose (0.5–1 mg/kg) is given on the first day, increasing to 1–2 mg/kg on the second day, followed by 1.5–3 mg/kg on the third and subsequent days.
Miltefosine Impavido is the first oral treatment for this disease. The cure rate of miltefosine in Phase III clinical trials is 95%; Studies in Ethiopia show that is also effective in Africa. In HIV immunosuppressed people which are coinfected with leishmaniasis it has shown that even in resistant cases 2/3 of the people responded to this new treatment. Miltefosine has received approval by the Indian regulatory authorities in 2002 and in Germany in 2004.It is now registered in many countries.
The drug is generally better tolerated than other drugs. Main side effects are gastrointetinal disturbance in the first or second day of treatment (a course of treatment is 28 days) which does not affect the efficiency. Because it is available as an oral formulation, the expense and inconvenience of hospitalization is avoided, and outpatient distribution of the drug becomes an option, making Miltefosine a drug of choice.
The nonprofit Institute for OneWorld Health has adopted the broad spectrum antibiotic paromomycin for use in treating VL; its antileishmanial properties were first identified in the 1980s. A treatment with paromomycin costs about $15 USD. The drug had originally been identified in the 1960s.[27] The Indian government approved paromomycin for sale and use in August 2006.[28]
In 2009, the Hebrew University of Jerusalem Kuvin Center for the Study of Infectious and Tropical Diseases, in a collaborative effort with Addis Ababa University, was awarded a grant by the Bill & Melinda Gates Foundation for research into visceral leishmaniasis in Ethiopia. The project will gather data to be analyzed to identify the weak links in the transmission cycle and devise methods for control of the disease.[29]
Combination drug therapies are currently under investigation, particularly by the Drugs for Neglected Diseases initiative (DNDi). Combination therapies allow for the use of existing drugs in combination, each in lower doses, which helps to decrease the incidence of severe side effects and drug toxicity, as well as the risk for development of resistance against the drugs; they have been shown to be cost-effective strategies strategies.[30]
The drug development pipeline is lacking significantly, and no novel drug targets are expected for approval in the next 5 years.[31] In the meantime, new combination therapies, and well as improvements to existing drugs targets, are under development. Single-dosage administrations of liposomal amphotericin B have been shown to be effective, and oral formulations are currently under development to increase access and facilitate distribution of the efficacious drug in the field.[32][33]
History and epidemiology
See also History of leishmaniasis
Kala-azar first came to the attention of Western doctors in 1824 in Jessore, India (now Bangladesh), where it was initially thought to be a form of malaria. Assam gave kala-azar one of its common names, Assam fever.[34] Another common name, kala-azar, is derived from kala which means black in Sanskrit, Assamese,[35] Hindi and Urdu[36] and the Persian azar for disease,[35] so called for the darkening of the skin on the extremities and abdomen that is a symptom of the Indian form of the disease. The agent of the disease was also first isolated in India by Scottish doctor William Leishman and Irish physician Charles Donovan, working independently of each other. As they published their discovery almost simultaneously, the species was named for both of them — Leishmania donovani.
Today, the name kala-azar is used interchangeably with the scientific name visceral leishmaniasis for the most acute form of the disease caused by L. donovani. The disease is endemic in West Bengal, where it was first discovered, but is seen at its most deadly in north and east Africa. It can also be found throughout the Arab world and southern Europe (where the causative organism is L. infantum), and a slightly different strain of the pathogen, L. chagasi, is responsible for leishmaniasis in the new world. Several species of canines serve as reservoir hosts of L. infantum (chagasi).
But, while the disease's geographical range is broad, it is not continuous. The disease clusters around areas of drought, famine, and high population density. In Africa, this has meant a knot of infection centers mostly in Sudan, Kenya, and Somalia. Living conditions here have changed very little in the past century, and the people are not normally very mobile. Parts of the Sudan, in particular the Upper Nile region, are almost totally cut off from the rest of the country, and the people are as tied to the place of their birth as any peasant of Europe’s Dark Ages.[37]
Contemporary life has made itself felt even here, however—not as "progress" but in the form of the many small wars of Africa's post-colonial era. In the Sudan, where civil war has been continuous since 1983, the violence has been concentrated in the more populated south, and kala-azar was concentrated there too. But the wars have driven a steady stream of refugees out of the region, and these traveled either across the southern border or into the remoter western part of the country called the Upper Nile, where both war and the disease that went with it had not yet penetrated.[37]
These refugees, moving at foot-speed, carried the disease with them, and when it arrived it hit the Upper Nile with a force comparable to smallpox hitting the American Indians. The isolated people of the Upper Nile had no access to medicine or education about the new disease among them. Worse, their immune systems were defenseless against this new pathogen, foreign to them though it came only from another part of their own country. One village at the center of the epidemic, Duar, was left with four survivors out of a population of a thousand, and from the late eighties to the mid-nineties a total of 100,000 succumbed to the sickness in that region alone. In the words of Jill Seaman, the doctor who led relief efforts in the Upper Nile for the French organization Médecins Sans Frontières, “Where else in the world could 50% of a population die without anyone knowing?”[38]
North Bihar, India (including Araria, Purnea and Kishanganj) is the endemic zone of this disease.
See also
References
- ^ James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 0-7216-2921-0.
- ^ Desjeux P. (2001). "The increase of risk factors for leishmaniasis worldwide". Transactions of the Royal Society of Tropical Medicine and Hygiene 95 (3): 239–43. doi:10.1016/S0035-9203(01)90223-8. PMID 11490989.
- ^ "Leishmaniasis and HIV co-infection". WHO. http://www.who.int/leishmaniasis/burden/hiv_coinfection/burden_hiv_coinfection/en/index.html.
- ^ Carvalho E, Badaro R, Reed S, Jones T, Johnson W (1985) “Absence of Gamma Interferon and Interleukin 2 Production During Active Visceral Leishmaniasis”. J Clin Invest 76(6): 2066-2069. PMID: 3935667
- ^ Holaday B, Pompeu M, Evans T, de Melo Braga D, Texeira M, Sousa A, Sadick M, Vasconcelos A, Abrams J, Pearson R, Locksley R (1993) “Correlates of Leishmania-Specifc Immunity in the Clinical Spectrum of Infection with Leishmania chagasi" J infect Dis 167(2): 411-417. PMID: 8421174
- ^ Karp C, El-Safi S, Wynn T, Satti M, Kordofani A, Hashim F, Hag-Ali M, Neva F, Nutman T, Sacks D (1993) “In Vivo Cytokine Profiles in Patients with Kala-azar: Marked Elevation of Both Interleukin-10 and Interferon-gamma”. J Clin Invest 91(4): 1644-1648. PMID: 8097208
- ^ Ghalib H, Piuvezam M, Skeiky Y (1993) “Interleukin 10 production correlates with pathology in human Leishmania donovani infections”. J Clin Invest 92(1): 324-329. PMID: 8326000
- ^ Holaday B, Pompeu M, Jeronimo S, Texeira M, Sousa A, Vasconcelos W, Pearson R, Abrams J, Locksley R (1993). “Potential Role for Interleukin-10 in Immunosuppression Associated with Kala Azar”. J of Clin Invest 92(2): 2626-2632. PMID 8254019
- ^ Ghalib H, Whittle J, Kubin M, Hashim F, El-Hassan A, Grabstein K, Trinchieri G, Reed S (1995). “IL-12 Enhances Th1-Type Responses in Human Leishmania donovani Infections”. J Immunol 154(9): 4623-4629. PMID: 7722314
- ^ Bacellar O, Brodskyn C, Guerreiro J, Barral-Netto M, Costa C, Coffman R, Johnson W, Carvalho E (1996). “Interleukin-12 Restores Interferon-gamma Production and Cytotoxic Responses in Visceral Leishmaniasis” J Infect Dis 173(6):1515-1518. PMID: 8648233
- ^ Holaday B (1999). “Immunotherapy for Visceral Leishmaniasis: Ability of Factors Produced during Anti-leishmania Responses of Skin Test Positive Adults to Inhibit Peripheral Blood Mononuclear Cell Activities Associated with Visceral Leishmaniasis”. Mem Inst Oswaldo Cruz 94(1): 55-66. PMID: 10029912
- ^ Holaday B (2000) “Role of CD8+ T Cells in Endogenous Interleukin-10 Secretion Associated with Visceral Leishmaniasis” Mem Inst Oswaldo Cruz 95(2): 217-220. PMID: 10733741
- ^ Ganguly S, Mukhopadhyay D, Das N, Chaduvula M,Sadhu S, Chatterjee U, Rahman M, Goswami R, Guha S, Modak D, Mallik S, Gonju D, Pramanik N, Barbhuiya J, Saha B, Chatterjee M (2010) “Enhanced Lesional Foxp3 Expression and Peripheral Anergic Lymphocytes Indicate a Role for Regulatory T Cells in Indian Post-Kala-Azar Dermal Leishmaniasis”. J Invest Dermatol 130(4): 1013-1022. PMID: 20032994
- ^ Kemp M, Kurtzhals J, Bendtzen K, Poulsen L, Hansen M, Koech D, Kharazmi A, Theander T (1993) “Leishmania donovani-Reactive Thl- and Th2-Like T-Cell Clones from Individuals Who Have Recovered from Visceral Leishmaniasis” Infect Immun 61(3): 1069-1073. PMID: 8432588
- ^ Chappuis F, Rijal S, Soto A, Menten J, Boelaert M (2006). "A meta-analysis of the diagnostic performance of the direct agglutination test and rK39 dipstick for visceral leishmaniasis". Brit Med J 333 (7571): 723–6. doi:10.1136/bmj.38917.503056.7C. PMC 1592383. PMID 16882683. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1592383.
- ^ Sundar S, Singh RK, Maurya R, et al. (June 2006). "Serological diagnosis of Indian visceral leishmaniasis: direct agglutination test versus rK39 strip test". Trans. R. Soc. Trop. Med. Hyg. 100 (6): 533–7. doi:10.1016/j.trstmh.2005.08.018. PMID 16325874. http://linkinghub.elsevier.com/retrieve/pii/S0035-9203(05)00330-5.
- ^ Sundar S, Maurya R, Singh RK, et al. (January 2006). "Rapid, noninvasive diagnosis of visceral leishmaniasis in India: comparison of two immunochromatographic strip tests for detection of anti-K39 antibody". J. Clin. Microbiol. 44 (1): 251–3. doi:10.1128/JCM.44.1.251-253.2006. PMC 1351954. PMID 16390983. http://jcm.asm.org/cgi/pmidlookup?view=long&pmid=16390983.
- ^ a b Lockwood DN, Sundar S (October 2006). "Serological tests for visceral leishmaniasis". BMJ 333 (7571): 711–2. doi:10.1136/bmj.38989.567083.BE. PMC 1592372. PMID 17023436. http://bmj.com/cgi/pmidlookup?view=long&pmid=17023436.
- ^ Pasquau F, Ena J, Sanchez R, et al. (June 2005). "Leishmaniasis as an opportunistic infection in HIV-infected patients: determinants of relapse and mortality in a collaborative study of 228 episodes in a Mediterreanean region". Eur. J. Clin. Microbiol. Infect. Dis. 24 (6): 411–8. doi:10.1007/s10096-005-1342-6. PMID 15928908.
- ^ Sundar S, More DK, Singh MK, et al. (October 2000). "Failure of pentavalent antimony in visceral leishmaniasis in India: report from the center of the Indian epidemic". Clin. Infect. Dis. 31 (4): 1104–7. doi:10.1086/318121. PMID 11049798. http://www.journals.uchicago.edu/cgi-bin/resolve?CID000236.
- ^ Thakur CP, Narayan S, Ranjan A (September 2004). "Epidemiological, clinical & pharmacological study of antimony-resistant visceral leishmaniasis in Bihar, India" (PDF). Indian J. Med. Res. 120 (3): 166–72. PMID 15489554. http://www.icmr.nic.in/ijmr/2004/0904.pdf.
- ^ Nobel Foundation (2008). The Nomination Database for the Nobel Prize in Physiology or Medicine, 1901-1951
- ^ Upendra Nath Brahmachari: A Pioneer of Modern Medicine in India. Vigyan Prasar: Government of India
- ^ Thakur CP, Singh RK, Hassan SM, Kumar R, Narain S, Kumar A (1999). "Amphotericin B deoxycholate treatment of visceral leishmaniasis with newer modes of administration and precautions: a study of 938 cases". Trans. R. Soc. Trop. Med. Hyg. 93 (3): 319–23. doi:10.1016/S0035-9203(99)90037-8. PMID 10492770.
- ^ Thakur CP, Pandey AK, Sinha GP, Roy S, Behbehani K, Olliaro P (1996). "Comparison of three treatment regimens with liposomal amphotericin B (AmBisome) for visceral leishmaniasis in India: a randomized dose-finding study". Trans. R. Soc. Trop. Med. Hyg. 90 (3): 319–22. doi:10.1016/S0035-9203(96)90271-0. PMID 8758093.
- ^ Sundar S, Mehta H, Chhabra A, et al. (March 2006). "Amphotericin B colloidal dispersion for the treatment of Indian visceral leishmaniasis". Clin. Infect. Dis. 42 (5): 608–13. doi:10.1086/500138?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dncbi.nlm.nih.gov. PMID 16447104.
- ^ A Small Charity Takes the Reins in Fighting a Neglected Disease, New York Times, July 31, 2006.
- ^ NEW CURE FOR DEADLY VISCERAL LEISHMANIASIS (KALA-AZAR) APPROVED BY GOVERNMENT OF INDIA, Institute for OneWorld Health Press Release, Sept 8, 2006.
- ^ $5m for disease control in Ethiopia in Israel 21c Innovation News Service Retrieved 2009-12-30
- ^ Olliaro, P., Darley, S., Laxminarayan, R., et al. (2009). "Cost-effectiveness projections of single and combination therapies for visceral leishmaniasis in Bihar, India". Trop Med Int Health 14 (8): 918–925. doi:10.1111/j.1365-3156.2009.02306.x. PMID 19563434.
- ^ den Boer, M.L., Alvar, J., Davidson, R.N., et al. (2009). "Developments in the treatment of visceral leishmaniasis". Expert Opin. Emerging Drugs 14 (3): 395–410. doi:10.1517/14728210903153862. PMID 19708817.
- ^ Sundar, S., Chakravarty, J., Agarwal, D., et al. (2010). "Single-dose liposomal amphotericin B for visceral leishmaniasis in India". N Engl J Med 362 (6): 504–512. doi:10.1056/NEJMoa0903627. PMID 20147716.
- ^ Wasan, K. M., Wasan, E. K., Gershkovich, P., et al. (2009). "Highly effective oral amphotericin B formulation against murine visceral leishmaniasis". J Infect Dis 200 (3): 557–360. doi:10.1086/600105. PMID 19545212.
- ^ "Mosby's Medical Dictionary, 8th edition. © 2009, Elsevier.". "kala-azar". http://www.medical-dictionary.thefreedictionary.com/kala-azar. Retrieved 2010-01-21.
- ^ a b "HarperCollins Publishers, 1991, 1994, 1998, 2000, 2003.". "kala-azar". http://www.thefreedictionary.com/kala-azar. Retrieved 2010-01-21.
- ^ Merriam-Webster's online dictionary. "kala-azar". http://www.merriam-webster.com/dictionary/kala-azar. Retrieved 2010-01-21.
- ^ a b Jean, Francois (1995). "Sudan: Speak no Evil, Do no Good". Life, Death and Aid: the Médecins Sans Frontières Report on World Crisis Intervention.
- ^ Dowell, William (1997). "Rescue in Sudan". Time.
Infectious diseases – Parasitic disease: protozoan infection: Excavata (A06–A07, B55–B57, 007, 085–086) Discicristata TrypanosomatidaLeishmania major/L. mexicana/L. aethiopica/L. tropica (Cutaneous leishmaniasis) · L. braziliensis (Mucocutaneous leishmaniasis) · L. donovani/infantum (Visceral leishmaniasis)SchizopyrenidaTrichozoa TrichomonadidaDiseases of poverty Diseases of poverty Neglected diseases Cholera · Chagas disease · African Sleeping Sickness · Schistosomiasis · Guinea worm · River blindness · LeishmaniasisMiscellaneous Categories:- Protozoal diseases
- Neglected diseases
- Parasitic infestations, stings, and bites of the skin
Wikimedia Foundation. 2010.