- Management of prostate cancer
-
Treatment for prostate cancer may involve active surveillance, surgery, radiation therapy including brachytherapy (prostate brachytherapy) and external beam radiation therapy, High-intensity focused ultrasound (HIFU), chemotherapy, cryosurgery, hormonal therapy, or some combination. Which option is best depends on the stage of the disease, the Gleason score, and the PSA level. Other important factors are the man's age, his general health, and his feelings about potential treatments and their possible side effects. Because all treatments can have significant side effects, such as erectile dysfunction and urinary incontinence, treatment discussions often focus on balancing the goals of therapy with the risks of lifestyle alterations.
The selection of treatment options may be a complex decision involving many factors. For example, radical prostatectomy after primary radiation failure is a very technically challenging surgery and may not be an option.[1] This may enter into the treatment decision.
If the cancer has spread beyond the prostate, treatment options significantly change, so most doctors that treat prostate cancer use a variety of nomograms to predict the probability of spread. Treatment by watchful waiting/active surveillance, HIFU, external beam radiation therapy, brachytherapy, cryosurgery, and surgery are, in general, offered to men whose cancer remains within the prostate. Hormonal therapy and chemotherapy are often reserved for disease that has spread beyond the prostate. However, there are exceptions: Radiation therapy may be used for some advanced tumors, and hormonal therapy is used for some early stage tumors. Cryotherapy (the process of freezing the tumor), hormonal therapy, and chemotherapy may also be offered if initial treatment fails and the cancer progresses.[2]
Contents
Active surveillance
Active surveillance refers to observation and regular monitoring without invasive treatment. In the context of prostate disease this usually comprises regular PSA blood tests and prostate biopsies. Active surveillance is often used when an early stage, slow-growing prostate cancer is suspected. However, watchful waiting may also be suggested when the risks of surgery, radiation therapy, or hormonal therapy outweigh the possible benefits. Other treatments can be started if symptoms develop, or if there are signs that the cancer growth is accelerating (e.g., rapidly-rising PSA, increase in Gleason score on repeat biopsy, etc.).
Approximately one-third of men that choose active surveillance for early stage tumors eventually have signs of tumor progression, and they may need to begin treatment within three years.[3] Men that choose active surveillance avoid the risks of surgery, radiation, and other treatments. The risk of disease progression and metastasis (spread of the cancer) may be increased, but this increase risk appears to be small if the program of surveillance is followed closely, generally including serial PSA assessments and repeat prostate biopsies every 1–2 years depending on the PSA trends.
Study results in 2011 suggest active surveillance is the best choice for older 'low-risk' patients.[4]
For younger men, a trial of active surveillance may not mean avoiding treatment altogether, but may reasonably allow a delay of a few years or more, during which time the quality of life impact of active treatment can be avoided. Published data to date suggest that carefully selected men will not miss a window for cure with this approach.[citation needed] Additional health problems that develop with advancing age during the observation period can also make it harder to undergo surgery and radiation therapy.
Hormonal therapy
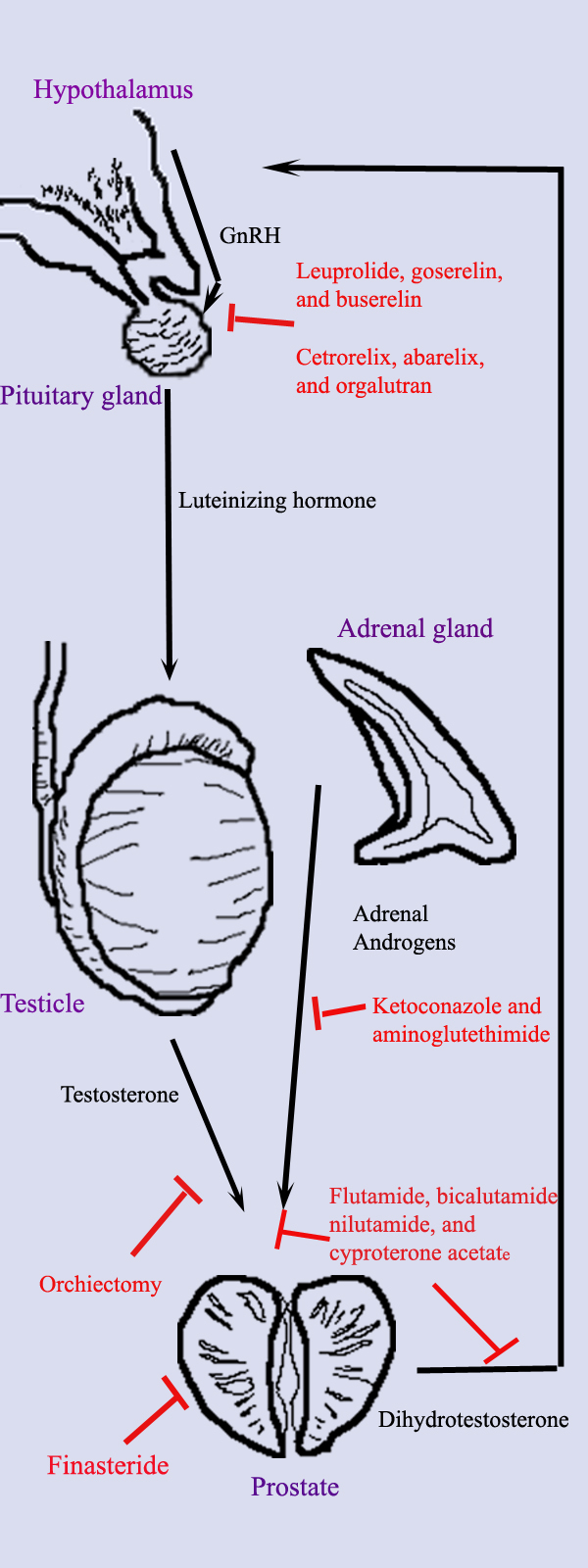
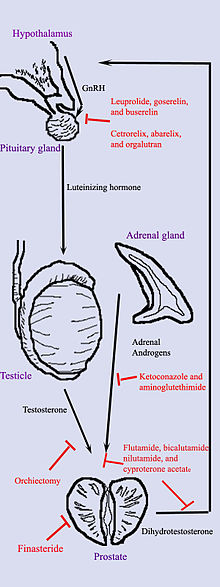 Hormonal therapy in prostate cancer. Diagram shows the different organs (purple text), hormones (black text and arrows), and treatments (red text and arrows) important in hormonal therapy.
Hormonal therapy in prostate cancer. Diagram shows the different organs (purple text), hormones (black text and arrows), and treatments (red text and arrows) important in hormonal therapy.
Hormonal therapy uses medications or surgery to block prostate cancer cells from getting dihydrotestosterone (DHT), a hormone produced in the prostate and required for the growth and spread of most prostate cancer cells. Blocking DHT often causes prostate cancer to stop growing and even shrink. However, hormonal therapy rarely cures prostate cancer because cancers that initially respond to hormonal therapy typically become resistant after one to two years. Hormonal therapy is, therefore, usually used when cancer has spread from the prostate. It may also be given to certain men undergoing radiation therapy or surgery to help prevent return of their cancer.[5]
Hormonal therapy for prostate cancer targets the pathways the body uses to produce DHT. A feedback loop involving the testicles, the hypothalamus, and the pituitary, adrenal, and prostate glands controls the blood levels of DHT. First, low blood levels of DHT stimulate the hypothalamus to produce gonadotropin-releasing hormone (GnRH). GnRH then stimulates the pituitary gland to produce luteinizing hormone (LH), and LH stimulates the testicles to produce testosterone. Finally, testosterone from the testicles and dehydroepiandrosterone from the adrenal glands stimulate the prostate to produce more DHT. Hormonal therapy can decrease levels of DHT by interrupting this pathway at any point. There are several forms of hormonal therapy:
- Orchiectomy, also called "castration," is surgery to remove the testicles. Because the testicles make most of the body's testosterone, after orchiectomy testosterone levels drop. Now the prostate not only lacks the testosterone stimulus to produce DHT but also does not have enough testosterone to transform into DHT. Orchiectomy is considered the gold standard of treatment.[6]
- Antiandrogens are medications such as flutamide, bicalutamide, nilutamide, and cyproterone acetate that directly block the actions of testosterone and DHT within prostate cancer cells.
- Medications that block the production of adrenal androgens such as DHEA include ketoconazole and aminoglutethimide. Because the adrenal glands make only about 5% of the body's androgens, these medications are, in general, used only in combination with other methods that can block the 95% of androgens made by the testicles. These combined methods are called total androgen blockade (TAB). TAB can also be achieved using antiandrogens.
- GnRH action can be interrupted in one of two ways. GnRH antagonists such as abarelix and degarelix suppress the production of LH directly by acting on the anterior pituitary. GnRH agonists such as leuprolide and goserelin acetate suppress LH through the process of downregulation after an initial stimulation effect which can cause initial tumor flare. Abarelix and degarelix are examples of GnRH antagonists, whereas the GnRH agonists include leuprolide, goserelin, triptorelin, and buserelin. Initially, GnRH agonists increase the production of LH. However, because the constant supply of the medication does not match the body's natural production rhythm, production of both LH and GnRH decreases after a few weeks.[7]
- Abiraterone acetate was FDA approved in April 2011 for treatment of castration-resistant prostate cancer for patients who have failed docetaxel therapy. Abiraterone inhibits an enzyme known as CYP17, which is used in the body to produce testosterone.[8][9]
The most successful hormonal treatments are orchiectomy and GnRH agonists. Despite their higher cost, GnRH agonists are often chosen over orchiectomy for cosmetic and emotional reasons. Eventually, total androgen blockade may prove to be better than orchiectomy or GnRH agonists used alone.
Each treatment has disadvantages that limit its use in certain circumstances. Although orchiectomy is a low-risk surgery, the psychological impact of removing the testicles can be significant, and sterility is certain. The loss of testosterone can cause hot flashes, weight gain, loss of libido, enlargement of the breasts (gynecomastia), impotence, penile atrophy, and osteoporosis. GnRH agonists eventually cause the same side effects as orchiectomy but may cause worse symptoms at the beginning of treatment. When GnRH agonists are first used, testosterone surges can lead to increased bone pain from metastatic cancer, so antiandrogens or abarelix is often added to blunt these side effects. Estrogens are not commonly used because they increase the risk for cardiovascular disease and blood clots. In general, the antiandrogens do not cause impotence, and usually cause less loss of bone and muscle mass. Ketoconazole can cause liver damage with prolonged use, and aminoglutethimide can cause skin rashes.
Surgery
Main article: ProstatectomySurgical removal of the prostate, or prostatectomy, is a common treatment either for early stage prostate cancer or for cancer that has failed to respond to radiation therapy. The most common type is radical retropubic prostatectomy, when the surgeon removes the prostate through an abdominal incision. Another type is radical perineal prostatectomy, when the surgeon removes the prostate through an incision in the perineum, the skin between the scrotum and anus. Radical prostatectomy can also be performed laparoscopically, through a series of small (1 cm) incisions in the abdomen, with or without the assistance of a surgical robot.
Radical prostatectomy
Radical prostatectomy is effective for tumors that have not spread beyond the prostate;[10] cure rates depend on risk factors such as PSA level and Gleason grade. However, it may cause nerve damage that may significantly alter the quality of life of the prostate cancer survivor.
Radical prostatectomy has traditionally been used alone when the cancer is localized to the prostate. In the event of positive margins or locally advanced disease found on pathology, adjuvant radiation therapy may offer improved survival. Surgery may also be offered when a cancer is not responding to radiation therapy. However, because radiation therapy causes tissue changes, prostatectomy after radiation has higher risks of complications.
Laparoscopic radical prostatectomy, LRP, is a new way to approach the prostate surgically with intent to cure. Contrasted with the open surgical form of prostate cancer surgery, laparoscopic radical prostatectomy requires a smaller incision. Relying on modern technology, such as miniaturization, fiber optics, and the like, laparoscopic radical prostatectomy is a minimally invasive prostate cancer treatment but is technically demanding and seldom done in the USA.
Some believe that in the hands of an experienced surgeon, robotic-assisted laparoscopic prostatectomy (RALP) may reduce positive surgical margins when compared to radical retropubic prostatectomy (RRP) among patients with prostate cancer according to a retrospective study.[11] The relative risk reduction was 57.7%. For patients at similar risk to those in this study (35.5% of patients had positive surgical margins following RRP), this leads to an absolute risk reduction of 20.5%. 4.9 patients must be treated for one to benefit (number needed to treat = 4.9). Other recent studies have shown RALP to result in a significantly higher rate of positive margins.[12] Other studies showed no difference of robotic to open surgery.[13] A recent French study comparing standard laparoscopic to robotic to open prostatectomy showed no difference in margin status or biochemical recurrence at 5 years.[14] The relative merits of RALP and potential benefit versus open radical prostatectomy is currently an area of intense research and debate in urology. The only proven and accepted advantage to RALP is less intraoperative blood loss. Other suggested advantages beyond this lack definitive data and have not been widely accepted by the broader urological community.
Transurethral resection of the prostate
Transurethral resection of the prostate, commonly called a "TURP," is a surgical procedure performed when the tube from the bladder to the penis (urethra) is blocked by prostate enlargement. In general, TURP is for benign disease and is not meant as definitive treatment for prostate cancer. During a TURP, a small instrument (cystoscope) is placed into the penis and the blocking prostate is cut away.
Orchiectomy
In metastatic disease, where cancer has spread beyond the prostate, removal of the testicles (called orchiectomy) may be done to decrease testosterone levels and control cancer growth. (See hormonal therapy, below).
Cryosurgery
Cryosurgery is another method of treating prostate cancer in which the prostate gland is exposed to freezing temperatures.[15] It is less invasive than radical prostatectomy, and general anesthesia is less commonly used. Under ultrasound guidance, a method invented by Dr. Gary Onik,[16] metal rods are inserted through the skin of the perineum into the prostate. Highly-purified argon gas is used to cool the rods, freezing the surrounding tissue at −186 °C (−302 °F). As the water within the prostate cells freezes, the cells die. The urethra is protected from freezing by a catheter filled with warm liquid. In general, cryosurgery causes fewer problems with urinary control than other treatments, but impotence occurs up to ninety percent of the time. When used as the initial treatment for prostate cancer and in the hands of an experienced cryosurgeon, cryosurgery has a 10-year biochemical disease-free rate superior to all other treatments including radical prostatectomy and any form of radiation.[17] Cryosurgery has also been demonstrated to be superior to radical prostatectomy for recurrent cancer following radiation therapy.
Brachytherapy
Main article: Prostate brachytherapyBrachytherapy for prostate cancer involves the surgical placement of radioactive 'seeds' or implants directly into the cancerous portions of the prostate, where the radiation kills the surrounding cancerous cells. It is therefore usually classified as a radiation treatment, rather than as a surgical treatment, because the actual treatment of the disease is by radiation, not surgery. See: Brachytherapy, below
Complications of surgery
The most common serious complications of surgery are loss of urinary control and impotence. Reported rates of both complications vary widely depending on how they are assessed, by whom, and how long after surgery, as well as the setting (e.g., academic series vs. community-based or population-based data). Although penile sensation and the ability to achieve orgasm usually remain intact, erection and ejaculation are often impaired. Medications such as sildenafil (Viagra), tadalafil (Cialis), or vardenafil (Levitra) may restore some degree of potency. For most men with organ-confined disease, a more limited "nerve-sparing" technique may help reduce urinary incontinence and impotence.[18]
According to an online news story article in AOL Healthy Living, posted from Chicago, Illinois on Tuesday, September 20, 2011, by news writer Carla K. Johnson:
"A new study addresses one of the most worrying questions faced by men with prostate cancer: What are my chances of losing sexual function after treatment?
The answers vary greatly by age, sexual potency before treatment, PSA levels and whether a man has surgery, standard radiation or radioactive seeds, the study found.
Using the findings, men can get a rough idea of their personal odds by answering questions that also include weight and race, experts said.
Unsurprisingly, older men whose sexual function is already low have the worst chances of good sexual function after treatment.
"This will make it possible for patients to have a more realistic view of what to expect for themselves, rather than trying to guess where they fit in overall compared to the average guy with prostate cancer," said study co-author Dr. Martin Sanda of Beth Israel Deaconess Medical Center in Boston.
The federally funded study, appearing in Wednesday's Journal of the American Medical Association, included only men with early-stage cancers, and it didn't address cure rates for different treatments. In the real world, some patients have limited treatment choices. For instance, only men with early-stage, slow-growing cancers can choose radioactive pellets.
That means the findings may be most useful in giving a realistic picture of the sexual side effects of a treatment that's already chosen, rather than helping men pick a treatment.
Researchers studied factors affecting potency in men and developed a questionnaire to help measure it. They evaluated its usefulness among 1,027 prostate cancer patients ages 38 to 84 and validated its accuracy in a separate group of more than 1,900 men. It correctly predicted the chances of post-treatment potency in 77 percent of the men who had surgery to 90 percent of the men who had radiation.
The study found great variation in men's odds of having firm erections after treatment.
For surgery, the prospects for maintaining top sexual function for a 50-year-old man could range from 21 percent to 70 percent, depending on his PSA level and whether a nerve-sparing technique was used.
For standard radiation, the study found, the odds for a man keeping top sexual function ranged from 53 percent to 92 percent depending on PSA level and whether hormones were used along with radiation. The researchers couldn't find an age-related difference for standard radiation.
For radiation pellets, a 60-year-old man's chances of keeping top sexual function ranged from 58 percent to 98 percent depending on race and body mass index. African-Americans and trimmer men had better chances.
The study has some deficiencies, experts said.
It didn't include men who chose what's called "active surveillance," where a doctor keeps track of a tumor through regular tests and treats it only if the cancer markedly worsens. Many prostate cancer patients with slow-growing tumors can live their whole lives without symptoms or treatment, said Dr. Durado Brooks, prostate cancer director for the American Cancer Society. They die of something else before the cancer kills them.
"There are a lot of prostate cancers that are not likely to benefit from treatment," Brooks said. Including an active surveillance group would have shown how much sexual function changes because of factors other than treatment, such as age and general health, he said.
Most patients treated for early-stage prostate cancer survive, so the common side effects of treatment – incontinence and sexual problems – have become more important for patients making choices."[19]
Radiation therapy
Overview
 Brachytherapy for prostate cancer is administered using "seeds," small radioactive pellets or ribbons implanted directly into the tumor.
Brachytherapy for prostate cancer is administered using "seeds," small radioactive pellets or ribbons implanted directly into the tumor.Radiation therapy, also known as radiotherapy, is often used to treat all stages of prostate cancer. It is also often used after surgery if the surgery was not successful at curing the cancer. Radiotherapy uses ionizing radiation to kill prostate cancer cells. When absorbed in tissue, Ionizing radiation such as gamma and x-rays damage the DNA in cancer cells, which increases the probability of apoptosis (cell death). Normal cells are able to repair radiation damage, while cancer cells are not. Radiation therapy exploits this fact to treat cancer. Two different kinds of radiation therapy are used in prostate cancer treatment: external beam radiation therapy and brachytherapy (specifically prostate brachytherapy).
External beam radiation therapy
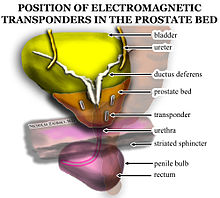 Electromagnetic fiducial transponder beacons are placed in the prostate bed after prostatectomy to improve radiation oncology accuracy. Transponders are placed in a triangular separation pattern, at least one centimeter apart from one another. There is one beacon on either lateral aspect of the vesicoureteral anastomosis and one in the retrovesical tissue approximately at the level where the seminal vesicles had been.
Electromagnetic fiducial transponder beacons are placed in the prostate bed after prostatectomy to improve radiation oncology accuracy. Transponders are placed in a triangular separation pattern, at least one centimeter apart from one another. There is one beacon on either lateral aspect of the vesicoureteral anastomosis and one in the retrovesical tissue approximately at the level where the seminal vesicles had been.External beam radiation therapy uses a linear accelerator to produce high-energy x-rays that are directed in a beam towards the prostate. A technique called Intensity Modulated Radiation Therapy (IMRT) may be used to adjust the radiation beam to conform with the shape of the tumor, allowing higher doses to be given to the prostate and seminal vesicles with less damage to the bladder and rectum. External beam radiation therapy is generally given over several weeks, with daily visits to a radiation therapy center. New types of radiation therapy such as IMRT have fewer side effects than traditional treatment. Doctors are also studying proton therapy for prostate cancer, which uses protons rather than X-rays to kill the cancer cells. They are also studying types of stereotactic body radiotherapy (SBRT) to treat prostate cancer.[20]
 External beam radiation therapyfor prostate cancer is delivered by a linear accelerator, such as this one.
External beam radiation therapyfor prostate cancer is delivered by a linear accelerator, such as this one.Brachytherapy
Main article: Prostate brachytherapyPermanent implant brachytherapy is a popular treatment choice for patients with low to intermediate risk features, can be performed on an outpatient basis, and is associated with good 10-year outcomes with relatively low morbidity[21] It involves the placement of about 100 small "seeds" containing radioactive material (such as iodine-125 or palladium-103) with a needle through the skin of the perineum directly into the tumor while under spinal or general anesthetic. These seeds emit lower-energy X-rays which are only able to travel a short distance. Although the seeds eventually become inert, they remain in the prostate permanently. The risk of exposure to others from men with implanted seeds is generally accepted to be insignificant.[22] However, men are encouraged to talk to their doctors about any special temporary precautions around small children and pregnant women.[23]
Uses
Radiation therapy is commonly used in prostate cancer treatment. It may be used instead of surgery or after surgery in early stage prostate cancer (adjuvant radiotherapy). Radiation treatments also can be combined with hormonal therapy for intermediate risk disease, when surgery or radiation therapy alone is less likely to cure the cancer. Some radiation oncologists combine external beam radiation and brachytherapy for intermediate to high-risk situations. Radiation therapy is often used in conjunction with hormone therapy for high-risk patients.[24] Others use a "triple modality" combination of external beam radiation therapy, brachytherapy, and hormonal therapy. In advanced stages of prostate cancer, radiation is used to treat painful bone metastases or reduce spinal cord compression.
Radiation therapy is also used after radical prostatectomy either for cancer recurrence or if multiple risk factors are found during surgery. Radiation therapy delivered immediately after surgery when risk factors are present (positive surgical margin, extracapsular extension, seminal vessicle involvement) has been demonstrated to reduce cancer recurrence, decrease distant metastasis, and increase overall survival in two separate randomized trials.[25]
Side effects
Side effects of radiation therapy might occur after a few weeks into treatment. Both types of radiation therapy may cause diarrhea and mild rectal bleeding due to radiation proctitis, as well as potential urinary incontinence and impotence. Symptoms tend to improve over time except erections which typically worsen as time progresses.
Comparison to surgery
Multiple retrospective analyses have demonstrated that overall survival and disease-free survival outcomes are similar between radical prostatectomy, external beam radiation therapy, and brachytherapy.[26] Rates for impotence when comparing radiation to nerve-sparing surgery are similar. Radiation has lower rates of incontinence compared with surgery, but has higher rates of occasional mild rectal bleeding.[27] Men who have undergone external beam radiation therapy may have a slightly higher risk of later developing colon cancer and bladder cancer.[28]
High intensity focused ultrasound (HIFU)
HIFU for prostate cancer utilizes high-intensity focused ultrasound to ablate/destroy the tissue of the prostate. During the HIFU procedure, sound waves are used to heat the prostate tissue, thus destroying the cancerous cells. In essence, ultrasonic waves are precisely focused on specific areas of the prostate to eliminate the prostate cancer, with minimal risks of affecting other tissue or organs. Temperatures at the focal point of the sound waves can exceed 100 °C (212 °F).[29] The ability to focus the ultrasonic waves leads to a relatively low occurrence of both incontinence and impotence. (0.6% and 0-20%, respectively)[30] According to preliminary international studies, HIFU has a high success rate with a reduced risk of side effects. Studies using HIFU machine have shown that 94% of patients with a pretreatment PSA (Prostate Specific Antigen) of less than 10 ng/mL were cancer-free after three years.[30] However, many studies of HIFU were performed by manufacturers of HIFU devices, or members of manufacturers' advisory panels.[31]
HIFU was first used in the 1940s and 1950s in efforts to destroy tumors in the central nervous system. Since then, HIFU has been shown to be effective at destroying malignant tissue in the brain, prostate, spleen, liver, kidney, breast, and bone.[29] Today, the HIFU procedure for prostate cancer is performed using a transrectal probe. This procedure has been performed for over ten years and is currently approved for use in Japan, Europe, Canada, and parts of Central and South America.
HIFU is currently not approved for medical use in the United States. Current NCCN guidelines for the treatment of prostate cancer do not include HIFU as part of standard of care, though many promising clinical trials exist. Many patients have received the HIFU procedure at facilities in Canada, and Central, and South America.
Contraindications to HIFU for prostate cancer include a prostate volume larger than 40 grams, which can prevent targeted HIFU waves from reaching the anterior and anterobasal regions of the prostate, anatomic or pathologic conditions that may interfere with the introduction or displacement of the HIFU probe into the rectum, and high-volume calcification within the prostate, which can lead to HIFU scattering and transmission impairment.[32]
Palliative care
Palliative care for advanced stage prostate cancer focuses on extending life and relieving the symptoms of metastatic disease. As noted above, Abiraterone Acetate is showing some promise in treating advance-stage prostate cancer. It causes a dramatic reduction in PSA levels and Tumor sizes in aggressive advanced-stage prostate cancer for 70% of patients. Chemotherapy may be offered to slow disease progression and postpone symptoms. The most commonly-used regimen combines the chemotherapeutic drug docetaxel with a corticosteroid such as prednisone. One study showed that treatment with docetaxel with prednisone prolonged life from 16.5 months for those taking mitoxantrone and prednisone to 18.9 months for those taking docetaxel + prednisone.[33] Bisphosphonates such as zoledronic acid have been shown to delay skeletal complications such as fractures or the need for radiation therapy in patients with hormone-refractory metastatic prostate cancer.[34] Alpharadin is a new alpha emitting pharmaceutical targeting bone metastasis. The phase II testing shows prolonged patient survival times, reduced pain, and improved quality of life.
Bone pain due to metastatic disease is treated with opioid pain relievers such as morphine and oxycodone. External beam radiation therapy directed at bone metastases may provide pain relief. Injections of certain radioisotopes, such as strontium-89, phosphorus-32, or samarium-153, also target bone metastases and may help relieve pain.
Alternative therapies
As an alternative to active surveillance or definitive treatments, other therapies are also under investigation for the management of prostate cancer. PSA has been shown to be lowered in men with apparent localized prostate cancer using a vegan diet (fish allowed), regular exercise, and stress reduction.[35] These results have so far proven durable after two-years' treatment. However, this study did not compare the vegan diet to either active surveillance or definitive treatment, and thus cannot comment on the comparative efficacy of the vegan diet in treating prostate cancer.[36]
Many other single agents have been shown to reduce PSA, slow PSA doubling times, or have similar effects on secondary markers in men with localized cancer in short term trials, such as pomegranate juice or genistein, an isoflavone found in various legumes.[37][38]
The potential of using multiple such agents in concert, let alone combining them with lifestyle changes, has not yet been studied. A more thorough review of natural approaches to prostate cancer has been published.[39]
Neutrons have been shown to be superior to X-rays in a the treatment of prostatic cancer. The rationale is that tumours containing hypoxic cells (cells with enough oxygen concentration to be viable, yet not enough to be X-ray-radiosensitive) and cells deficient in oxygen are resistant to killing by X-rays. Thus, the lower Oxygen Enhancement Ratio (OER) of neutrons confers an advantage. Also, neutrons have a higher relative biological effectiveness (RBE) for slow-growing tumours than X-rays, allowing for an advantage in tumour cell killing.[40]
Prevention
Neither selenium nor vitamin E have been found to be effective in preventing prostate cancer.[41]
References
- ^ Mouraviev V, Evans B, Polascik TJ (2006). "Salvage prostate cryoablation after primary interstitial brachytherapy failure: a feasible approach". Prostate Cancer Prostatic Dis. 9 (1): 99–101. doi:10.1038/sj.pcan.4500853. PMID 16314889.
- ^ "Prostate Cancer At A Glance". ShaveMagazine.com. http://www.shavemagazine.com/body/health/090401/2.
- ^ Wu, H; Sun L, Moul JW, Wu HY, McLeod DG, Amling C, Lance R, Kusuda L, Donahue T, Foley J, Chung A, Sexton W, Soderdahl D (March 2004). "Watchful waiting and factors predictive of secondary treatment of localized prostate cancer". J Urol 171 (3): 1111–6. doi:10.1097/01.ju.0000113300.74132.8b. PMID 14767282.
- ^ http://www.cancer.gov/ncicancerbulletin/041911/page2 Active Surveillance May Be Preferred Option in Some Men with Prostate Cancer
- ^ Robson, M; Dawson N (June 1996). "How is androgen-dependent metastatic prostate cancer best treated?". Hematol Oncol Clin North Am 10 (3): 727–47. doi:10.1016/S0889-8588(05)70364-6. PMID 8773508. Review.
- ^ Immediate versus deferred treatment for advanced prostatic cancer: initial results of the Medical Research Council Trial. The Medical Research Council Prostate Cancer Working Party Investigators Group. Br J Urol. 1997 Feb;79(2):235-46.
- ^ Loblaw, DA; Mendelson DS, Talcott JA, Virgo KS, Somerfield MR, Ben-Josef E, Middleton R, Porterfield H, Sharp SA, Smith TJ, Taplin ME, Vogelzang NJ, Wade JL Jr, Bennett CL, Scher HI; American Society of Clinical Oncology (July 15 2004). "American Society of Clinical Oncology recommendations for the initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer". J Clin Oncol 22 (14): 2927–41. doi:10.1200/JCO.2004.04.579. PMID 15184404. Erratum in: J Clin Oncol. 2004 November 1;22(21):4435.
- ^ de Bono, Johann; Gerhardt Attard, Alison H.M. Reid, Timothy A. Yap, Florence Raynaud, Mitch Dowsett, Sarah Settatree, Mary Barrett, Christopher Parker, Vanessa Martins, Elizabeth Folkerd, Jeremy Clark, Colin S. Cooper, Stan B. Kaye, David Dearnaley, Gloria Lee (July 21 2004). "Phase I Clinical Trial of a Selective Inhibitor of CYP17, Abiraterone Acetate, Confirms That Castration-Resistant Prostate Cancer Commonly Remains Hormone Driven". J Clin Oncol 26 (14): online. doi:10.1200/JCO.2007.15.9749. PMID 18645193. http://jco.ascopubs.org/cgi/content/abstract/JCO.2007.15.9749v1. Erratum in: J Clin Oncol. Early Release, published ahead of print July 21, 2008
- ^ Richard Warry (July 22, 2008). "Drug for deadly prostate cancer". BBC. http://news.bbc.co.uk/2/hi/health/7517414.stm. Retrieved 2008-07-23.
- ^ Bill-Axelson A, Holmberg L, Ruutu M, et al. (2005). "Radical prostatectomy versus watchful waiting in early prostate cancer". N. Engl. J. Med. 352 (19): 1977–84. doi:10.1056/NEJMoa043739. PMID 15888698.
- ^ Smith JA, Chan RC, Chang SS, et al. (December 2007). "A comparison of the incidence and location of positive surgical margins in robotic assisted laparoscopic radical prostatectomy and open retropubic radical prostatectomy". J. Urol. 178 (6): 2385–9; discussion 2389–90. doi:10.1016/j.juro.2007.08.008. PMID 17936849.
- ^ Ou, YC; Yang CR, Wang J, Cheng CL, Patel VR (May 2009). "Comparison of Robotic-assisted versus Retropubic Radical Prostatectomy Performed by a Single Surgeon". Anticancer Res 29 (5): 1637–42. doi:10.1016/S0889-8588(05)70364-6. PMID 8773508.
- ^ Ham, WS; Park SY, Rha KH, Kim WT, Choi YD (June, 2009). "Robotic radical prostatectomy for patients with locally advanced prostate cancer is feasible: results of a single-institution study". J of laparoscopic and advanced surgical techniques 19 (3): 329–32.
- ^ Drouin, SJ; Vaessen C, Hupertan V, Comperat E, Misraï V, Haertig A, Bitker MO, Chartier-Kastler E, Richard F, Rouprêt M (May, 2009). "Comparison of mid-term carcinologic control obtained after open, laparoscopic, and robot-assisted radical prostatectomy for localized prostate cancer". World Journal of Urology.
- ^ PreventProstateCancer.info: A Brief Overview of Prostate Cancer
- ^ "Cryosurgical system for destroying tumors by freezing". 1994-08-02. http://www.patentstorm.us/patents/5334181.html.
- ^ Bahn, DK; Lee F, Badalament R, Kumar A, Greski J, Chernick M (August 2002). "Targeted cryoablation of the prostate: 7-year outcomes in the primary treatment of prostate cancer". Urology 60 (2 Suppl 1): 3–11. doi:10.1016/S0090-4295(02)01678-3. PMID 12206842.
- ^ Gerber, GS; Thisted RA, Scardino PT, Frohmuller HG, Schroeder FH, Paulson DF, Middleton AW Jr, Rukstalis DB, Smith JA Jr, Schellhammer PF, Ohori M, Chodak GW (August 28 1996). "Results of radical prostatectomy in men with clinically localized prostate cancer". JAMA 276 (8): 615–9. doi:10.1001/jama.276.8.615. PMID 8773633.
- ^ http://www.huffingtonpost.com/2011/09/20/sexual-potency-prostate-cancer_n_972482.html
- ^ http://www.rtanswers.com/treatment/disease/prostate_cancer.htm
- ^ Nag S, Beyer D, Friedland J, Grimm P, Nath R (July 1999). "American Brachytherapy Society (ABS) recommendations for transperineal permanent brachytherapy of prostate cancer". Int. J. Radiat. Oncol. Biol. Phys. 44 (4): 789–99. doi:10.1016/S0360-3016(99)00069-3. PMID 10386635.
- ^ Perez, CA; Hanks GE, Leibel SA, Zietman AL, Fuks Z, Lee WR (December 1 1993). "Localized carcinoma of the prostate (stages T1B, T1C, T2, and T3). Review of management with external beam radiation therapy". Cancer 72 (11): 3156–73. doi:10.1002/1097-0142(19931201)72:11<3156::AID-CNCR2820721106>3.0.CO;2-G. PMID 7694785. Review.
- ^ http://www.rtanswers.com/treatmentinformation/cancertypes/prostate/prostatebrach.aspx
- ^ D'Amico AV, Manola J, Loffredo M, Renshaw AA, DellaCroce A, Kantoff PW (2004). "6-month androgen suppression plus radiation therapy vs radiation therapy alone for patients with clinically localized prostate cancer: a randomized controlled trial". JAMA 292 (7): 821–7. doi:10.1001/jama.292.7.821. PMID 15315996.
- ^ Thompson IM, Tangen CM, Paradelo J (2009). "Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: long-term followup of a randomized clinical trial.". J Urol 181 (3): 956–62. doi:10.1016/j.juro.2008.11.032. PMID 19167731.
- ^ Kupelian PA, Elshaikh M, Reddy CA, Zippe C, Klein EA (August 2002). "Comparison of the efficacy of local therapies for localized prostate cancer in the prostate-specific antigen era: a large single-institution experience with radical prostatectomy and external-beam radiotherapy". J. Clin. Oncol. 20 (16): 3376–85. doi:10.1200/JCO.2002.01.150. PMID 12177097.
- ^ Lawton, CA; Won M, Pilepich MV, Asbell SO, Shipley WU, Hanks GE, Cox JD, Perez CA, Sause WT, Doggett SR, et al. (September 1991). "Long-term treatment sequelae following external beam irradiation for adenocarcinoma of the prostate: analysis of RTOG studies 7506 and 7706". Int J Radiat Oncol Biol Phys 21 (4): 935–9. doi:10.1016/0360-3016(91)90732-J. PMID 1917622.
- ^ Brenner, DJ; Curtis RE, Hall EJ, Ron E (January 15 2000). "Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery". Cancer 88 (2): 398–406. doi:10.1002/(SICI)1097-0142(20000115)88:2<398::AID-CNCR22>3.0.CO;2-V. PMID 10640974.
- ^ a b Gardner TA, Koch MO (December 2005). "Prostate cancer therapy with high-intensity focused ultrasound". Clin Genitourin Cancer 4 (3): 187–92. doi:10.3816/CGC.2005.n.031. PMID 16425987.
- ^ a b Uchida T, Ohkusa H, Yamashita H, et al. (March 2006). "Five years experience of transrectal high-intensity focused ultrasound using the Sonablate device in the treatment of localized prostate cancer". Int. J. Urol. 13 (3): 228–33. doi:10.1111/j.1442-2042.2006.01272.x. PMID 16643614.
- ^ Tom Pickles, Larry Goldenberg, Gary Steinhoff. High-Intensity Focused Ultrasound for Prostate Cancer. British Columbia Cancer Agencyhttp://www.bccancer.bc.ca/NR/rdonlyres/08EA1C8E-4345-4C7E-A83A-1F84853A1C27/8101/HIFUreport2005Feb10revised1.pdf
- ^ Barqawi AB, Crawford ED (2008). "Emerging Role of HIFU as a Noninvasive Ablative Method to Treat Localized Prostate Cancer". Oncology 22 (2). PMID 18409659. http://www.cancernetwork.com/display/article/10165/1146531.
- ^ Tannock, IF; de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA; TAX 327 Investigators (October 7 2004). "Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer". N Engl J Med 351 (15): 1502–12. doi:10.1056/NEJMoa040720. PMID 15470213.
- ^ Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, Chin JL, Vinholes JJ, Goas JA, Chen B (2002). "A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma". J Natl Cancer Inst 94 (19): 1458–68. PMID 12359855.
- ^ Ornish, D; Weidner G, Fair WR, et al. (2005). "Intensive lifestyle changes may affect the progression of prostate cancer". J Urol 174 (3): 1065–70. doi:10.1097/01.ju.0000169487.49018.73. PMID 16094059. http://www.pnas.org/content/105/24/8369.full.
- ^ Frattaroli J, Weidner G, Dnistrian AM, et al. (December 2008). "Clinical events in prostate cancer lifestyle trial: results from two years of follow-up". Urology 72 (6): 1319–23. doi:10.1016/j.urology.2008.04.050. PMID 18602144.
- ^ Pantuck, AJ; Leppert JT, Zomorodian N, et al. (2006). "Phase II study of pomegranate juice for men with rising prostate-specific antigen following surgery or radiation for prostate cancer". Clin Cancer Res 12 (13): 4018–26. doi:10.1158/1078-0432.CCR-05-2290. PMID 16818701.
- ^ Kumar, NB; Cantor A, Allen K, et al. (2004). "The specific role of isoflavones in reducing prostate cancer risk". Prostate 59 (2): 141–7. doi:10.1002/pros.10362. PMID 15042614.
- ^ Yarnell, E (1999). "A naturopathic approach to prostate cancer. Part 2: Guidelines for treatment and prevention". Altern Complemen Ther 5 (6): 360–8.
- ^ Hall, Eric J. (2000). Radiobiology for the Radiologist. Philadelphia, PA: Lippincott Williams & Williams. pp. 432–3. ISBN 0061410772.
- ^ Lippman SM, Klein EA, Goodman PJ, et al. (January 2009). "Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT)". JAMA 301 (1): 39–51. doi:10.1001/jama.2008.864. PMID 19066370.
Categories:- Cancer treatments


Wikimedia Foundation. 2010.