- Flutamide
-
Flutamide 
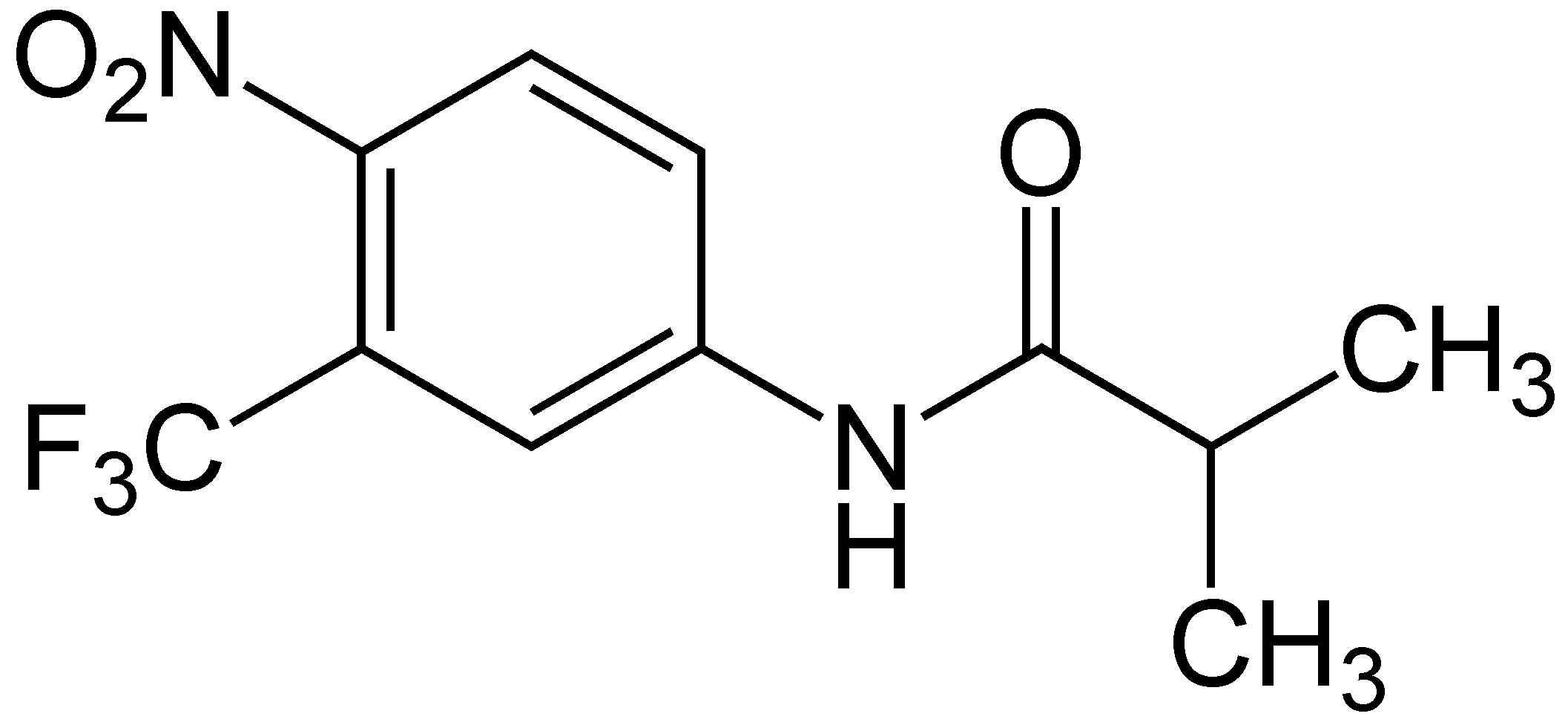
Systematic (IUPAC) name 2-methyl-N-[4-nitro-3-(trifluoromethyl)phenyl]-propanamide Clinical data AHFS/Drugs.com monograph MedlinePlus a697045 Pregnancy cat. D Legal status ℞ Prescription only Routes Oral Pharmacokinetic data Bioavailability >90% Protein binding 94 to 96% Excretion >90% via urine Identifiers CAS number 13311-84-7 ATC code L02BB01 PubChem CID 3397 DrugBank APRD00984 ChemSpider 3280 
UNII 76W6J0943E KEGG D00586 ChEBI CHEBI:5132 ChEMBL CHEMBL806 Chemical data Formula C11H11F3N2O3 Mol. mass 276.212 g/mol SMILES eMolecules & PubChem - InChI=1S/C11H11F3N2O3/c1-6(2)10(17)15-7-3-4-9(16(18)19)8(5-7)11(12,13)14/h3-6H,1-2H3,(H,15,17)
Key:MKXKFYHWDHIYRV-UHFFFAOYSA-N
 (what is this?) (verify)
(what is this?) (verify)Flutamide is an oral nonsteroidal antiandrogen drug primarily used to treat prostate cancer. It competes with testosterone and its powerful metabolite, dihydrotestosterone (DHT) for binding to androgen receptors in the prostate gland. By doing so, it prevents them from stimulating the prostate cancer cells to grow. Flutamide has been largely replaced by a newer member of this class, bicalutamide, due to a better side-effect profile. Flutamide may also be used to treat excess androgen levels in women - especially those with PolyCystic Ovarian Syndrom (PCOS)[1].[1] It is marketed by Schering-Plough under the brand name Eulexin. It is also known as Flutamin.
Contents
Structure
Unlike the hormones with which it competes, flutamide is not a steroid; rather, it is a substituted anilide. After absorption, the molecule is quickly α-hydroxylated to its primary active form, hydroxyflutamide. Flutamide is excreted in various forms in the urine, the primary form being 2-amino-5-nitro-4-(trifluoromethyl) phenol.
Use in prostate cancer
Gonadotropin-releasing hormone (GnRH) is released by the hypothalamus in a pulsatile fashion; this causes the anterior pituitary gland to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH stimulates the testes to produce testosterone, which is metabolized to DHT by the enzyme 5α-reductase. DHT, and to a much smaller extent, testosterone, stimulate prostate cancer cells to grow. Therefore, blocking these androgens can provide powerful treatment for prostate cancer, especially metastatic disease. Normally administered are analogues of GnRH, such as leuprolide or goserelin. Although they stimulate the same receptors that GnRH does, since they are present continuously and not in a pulsatile manner, they serve to inhibit the pituitary and therefore block the whole chain. However, they initially cause a surge in activity; this is not solely a theoretical risk but may cause the cancer to flare. Flutamide was initially used at the beginning of GnRH-analogue therapy to block this surge, and it and other nonsteroidal anti-androgens continue in this use.
There have been studies to investigate the benefit of adding an anti-androgen to surgical orchiectomy or its continued use with a GnRH analogue (combined androgen blockade, CAB). Adding anti-androgens to orchiectomy showed no benefit, while a small benefit was shown with adding anti-androgens to GnRH analogues
Unfortunately, therapies which lower testosterone levels, such as orchiectomy or GnRH-analogue administration, also have significant side effects. Compared to these therapies, treatment with antiandrogens exhibits "fewer hot flashes, less of an effect on libido, less muscle wasting, fewer personality changes, and less bone loss." However, antiandrogen therapy alone is less effective than surgery. Nevertheless, given the advanced age of many with prostate cancer, as well as other features, many men may choose antiandrogen therapy alone for a better quality of life.[2]
Side effects
In addition to the effects previously mentioned, flutamide may also induce gynecomastia. Tamoxifen can partially counteract this effect. Some patients experience mild liver injury, which resolves when the drug is discontinued. It may also cause gastrointestinal side effects; one reason bicalutamide is replacing flutamide is that it appears to exhibit these to a lesser degree.
Notes
- ^ http://www.nhs.uk/Conditions/Polycystic-ovarian-syndrome/Pages/Treatment.aspx
- ^ Scher, Howard I. (2005). "Hyperplastic and Malignant Diseases of the Prostate". In Dennis L. Kasper, Anthony S. Fauci, Dan L. Longo, Eugene Braunwald, Stephen L. Hauser, & J. Larry Jameson (Eds.), Harrison's Principles of Internal Medicine (16th edition), pp. 548–9. New York: McGraw-Hill.
References
- Chrousos, George P; Zoumakis, Emmanouil; & Gravanis, Achille. (2001). In Bertram G. Katzung (Ed.), Basic and Clinical Pharmacology (8th edition), pp 704–7. New York: Lange Medical Books/McGraw-Hill.
- http://pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=3397. PubChem. Accessed on December 3, 2005.
- http://www.rxlist.com/cgi/generic2/flutam_cp.htm. RxList. Accessed on December 3, 2005.
External links
- Schering-Plough (manufacturer's website)
Androgens (G03B) Agonist Testosterone# • Androstanolone • Fluoxymesterone • Mesterolone • Methyltestosterone • see also Anabolic steroidsSARM AC-262,356§ • Andarine (S-4)§ • BMS-564,929§ • LGD-2226§ • LGD-3303§ • Ostarine (MK-2866)§ • S-23§ • S-40503§Antiandrogen Bicalutamide • Cyproterone • Dienogest • Flutamide • Galeterone§ • MDV3100† • Nilutamide • SpironolactoneEnzyme inhibitors Alfatradiol • Bexlosteride • Dutasteride • Epristeride • Finasteride • Izonsteride • Lapisteride • TurosterideCYP17A1 inhibitorsAbiraterone • Galeterone§ • KetoconazoleCategories:- Antiandrogens
- Nitrobenzenes
- Organofluorides
- Anilides
- Propionamides
- InChI=1S/C11H11F3N2O3/c1-6(2)10(17)15-7-3-4-9(16(18)19)8(5-7)11(12,13)14/h3-6H,1-2H3,(H,15,17)
Wikimedia Foundation. 2010.