- Bedsore
-
Bedsore Classification and external resources 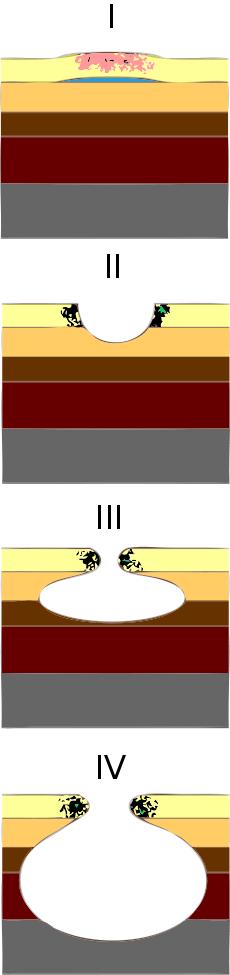
Progression of ulcersICD-10 L89 ICD-9 707.0 DiseasesDB 10606 eMedicine med/2709 MeSH D003668 Bedsores, more properly known as pressure ulcers or decubitus ulcers, are lesions caused by many factors—such as unrelieved pressure, friction, humidity, shearing forces, temperature, age, continence, and medication—to any part of the body, especially portions over bony or cartilaginous areas such as sacrum, elbows, knees, and ankles. Although often prevented and treatable if found early, they can be very difficult to prevent in frail elderly patients, wheelchair users (especially where spinal injury is involved) and terminally ill patients. Bedsores are often fatal—even under the auspices of medical care—and are one of the leading iatrogenic causes of death reported in developed countries, second only to adverse drug reactions. The primary cure and treatment is to remove the pressure by turning the patient regularly (every two hours is often quoted, though the evidence for this figure is not strong and four hourly turns may be as effective in some patients). However the relief of pressure to avoid further sores is well documented since at least the 19th century; regular turning was advised to prevent sores by Galloway [1] (though some of her other recommendations are not current practice, for example massage of the pressure area is probably contra-indicated) and virtually all authors since.
Contents
Classification
The definitions of the four pressure ulcer stages are revised periodically by the National Pressure Ulcer Advisory Panel (NPUAP) in the United States. Briefly, however, they are as follows:
- Stage I is the most superficial, indicated by non blanchable redness that does not subside after pressure is relieved. This stage is visually similar to reactive hyperemia seen in skin after prolonged application of pressure. Stage I pressure ulcers can be distinguished from reactive hyperemia in two ways: a) reactive hyperemia resolves itself within 3/4 of the time pressure was applied, and b) reactive hyperemia blanches when pressure is applied, whereas a Stage I pressure ulcer does not. The skin may be hotter or cooler than normal, have an odd texture, or perhaps be painful to the patient. Although easy to identify on a light-skinned patient, ulcers on darker-skinned individuals may show up as shades of purple or blue in comparison to lighter skin tones.
- Stage II is damage to the epidermis extending into, but no deeper than, the dermis. In this stage, the ulcer may be referred to as a blister or abrasion.
- Stage III involves the full thickness of the skin and may extend into the subcutaneous tissue layer. This layer has a relatively poor blood supply and can be difficult to heal. At this stage, there may be undermining damage that makes the wound much larger than it may seem on the surface
- Stage IV is the deepest, extending into the muscle, tendon or even bone. A graphic presentation of severe stage IV ulcers is visible here.
- Unstageable pressure ulcers are covered with dead cells, or eschar and wound exudate, so the depth cannot be determined.
Suspected Deep tissue injury: Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.
Further description: Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment.
With higher stages, healing time is prolonged. While about 75% of Stage II ulcers heal within eight weeks, only 62% of Stage IV pressure ulcers ever heal, and only 52% heal within one year.[2] It is important to note that pressure ulcers do not regress in stage as they heal. A pressure ulcer that is becoming shallower with healing is described in terms of its original deepest depth (e.g., healing Stage II pressure ulcer).
Etiology
Bedsores are accepted to be caused by three different tissue forces:
- Pressure, or the compression of tissues. In most cases, this compression is caused by the force of bone against a surface, as when a patient remains in a single decubitus position for a lengthy period. After an extended amount of time with decreased tissue perfusion, ischemia occurs and can lead to tissue necrosis if left untreated.
- Shear force, or a force created when the skin of a patient stays in one place as the deep fascia and skeletal muscle slide down with gravity. This can also cause the pinching off of blood vessels which may lead to ischemia and tissue necrosis.
- Friction, or a force resisting the shearing of skin. This may cause excess shedding through layers of epidermis.
Aggravating the situation may be other conditions such as excess moisture from incontinence, perspiration or exudate. Over time, this excess moisture may cause the bonds between epithelial cells to weaken thus resulting in the maceration of the epidermis. Temperature is also a very important factor. The cutaneous metabolic demand rises by 13% for every 1°C rise in cutaneous temperature. When supply can't meet demand, necrosis therefore occurs. Other factors in the development of bedsores include age, nutrition, vascular disease, diabetes mellitus, and smoking, amongst others.
There are currently two major theories about the development of pressure ulcers. The first and most accepted is the deep tissue injury theory which claims that the ulcers begin at the deepest level, around the bone, and move outward until they reach the epidermis. The second, less popular theory is the top-to-bottom model which says that skin first begins to deteriorate at the surface and then proceeds inward.[3]
 Stage 4 decubitus displaying the tuberosity of the ischium protruding through the tissue and possible onset of osteomyelitis
Stage 4 decubitus displaying the tuberosity of the ischium protruding through the tissue and possible onset of osteomyelitis
Pathophysiology
Pressure ulcers may be caused by inadequate blood supply and resulting reperfusion injury when blood re-enters tissue. A simple example of a mild pressure sore may be experienced by healthy individuals while sitting in the same position for extended periods of time: the dull ache experienced is indicative of impeded blood flow to affected areas. Within 2 hours, this shortage of blood supply, called ischemia, may lead to tissue damage and cell death. The sore will initially start as a red, painful area, which eventually turns purple. Left untreated, the skin may break open and become infected. Moist skin is more sensitive to tissue ischemia and necrosis and is also more likely to get infected. They are a sign of malnutrition.[citation needed]
Epidemiology
Within acute care in the United States, the incidence of bedsores is 0.4% to 38%; within long-term care, 2.2% to 23.9%; and in home care, 0% to 17%. There is the same wide variation in prevalence: 10% to 18% in acute care, 2.3% to 28% in long-term care, and 0% to 29% in home care. There is a much higher rate of bedsores in intensive care units because of immunocompromised individuals, with 8% to 40% of ICU patients developing bedsores.[4] However pressure ulcer prevalence is highly dependent on the methodology used to collect the data. Using the European Pressure Ulcer Advisory Panel (EPUAP) methodology there is are similar figures for pressure ulcers in acute hospital patients. There are differences across countries, but in Europe (for example) using this methodology pressure ulcer prevalence was consistently high, from 8.3% (Italy) to 22.9% (Sweden).[5] A recent study in Jordan also showed a figure in this range.[6]
The risk of developing bedsores can be determined by using the Braden Scale for Predicting Pressure Ulcer Risk.
Treatment
The best treatment outcomes will result from using a multidisciplinary team of specialists, this will ensure all problems are addressed.
There are seven major contributors to healing.
Preventative care
The most important care for a patient with bedsores is the relief of pressure. Once a bedsore is found, pressure should immediately be lifted from the area and the patient turned at least every two hours to avoid aggravating the wound. Nursing homes and hospitals usually set programs to avoid the development of bedsores in bedridden patients such as using a standing frame to reduce pressure and ensuring dry sheets by using catheters or impermeable dressings. For individuals with paralysis, pressure shifting on a regular basis and using a cushion featuring pressure relief components can help prevent pressure wounds.
Pressure-distributive mattresses are used to reduce high values of pressure on prominent or bony areas of the body.[7] Antidecubitus mattresses and cushions can contain multiple air chambers that are alternately pumped.[8] However, methods to evaluate the efficacy of these products have only been developed in recent years.[9]
Debridement
The removal of necrotic tissue is an absolute must in the treatment of pressure sores. Because dead tissue is an ideal area for bacterial growth, it has the ability to greatly compromise wound healing. There are at least seven ways to excise necrotic tissue.[3]
- Autolytic debridement is the use of moist dressings to promote autolysis with the body's own enzymes. It is a slow process, but mostly painless.
- Biological debridement, or maggot debridement therapy, is the use of medical maggots to feed on necrotic tissue and therefore clean the wound of excess bacteria. Although this fell out of favour for many years, in January 2004, the FDA approved maggots as a live medical device.[10]
- Chemical debridement, or enzymatic debridement, is the use of prescribed enzymes that promote the removal of necrotic tissue.
- Mechanical debridement is the use of outside force to remove dead tissue. A quite painful method, this involves the packing of a wound with wet dressings that are allowed to dry and then are removed. This is also unpopular because it has the ability to remove healthy tissue in addition to dead tissue. Lastly, with Stage IV ulcers, there is the chance that overdrying of the dressings can lead to bone fractures and ligament snaps.[citation needed]
- Sharp debridement is the removal of necrotic tissue with a scalpel or similar instrument.
- Surgical debridement is the most popular method, as it allows a surgeon to quickly remove dead tissue with little pain to the patient.
- Ultrasound-assisted wound therapy is the use of ultrasound waves to separate necrotic and healthy tissue.[citation needed]
Infection control
Infection has one of the greatest effects on the healing of a wound. Symptoms of systemic infection include fever, pain, redness, swelling, warmth of the area, and purulent discharge. Additionally, infected wounds may have a gangrenous smell, be discoloured, and may eventually exude even more pus.
In order to eliminate this problem, it is imperative to apply antiseptics at once. Hydrogen peroxide is not recommended for this task as it is difficult to balance the toxicity of the wound with this. New dressings have been developed that have cadexomer iodine and silver in them, and they are used to treat bad infections. Duoderm can be used on smaller wounds to both provide comfort and protect them from infection.
Systemic antibiotics are not recommended in treating infection of a bedsore, as it can lead to bacterial resistance.[citation needed]
Nutritional support
Upon admission the patient should have a consultation with a dietitian to determine the best diet to support healing, as a malnourished person does not have the ability to synthesize enough protein to repair tissue. The dietitian should conduct a nutritional assessment that includes a battery of questions and a physical examination. If malnourishment is suspected, lab tests should be run to check serum albumin and lymphocyte counts. Additionally, a bioelectrical impedance analysis should be considered.
If the patient is found to be at risk for malnutrition, it is imperative to begin nutritional intervention with dietary supplements and nutrients including, but not limited to, arginine, glutamine, vitamin A, vitamin B complex, vitamin E, vitamin C, magnesium, manganese, selenium and zinc. It is very important that intake of these vitamins and minerals be overseen by a physician, as many of them can be detrimental in incorrect dosages.
There is anecdotal evidence that high protein diet helps healing of sores. High protein diet seems to be especially helpful in sores that do not heal in eight weeks.
Educating the caregiver
In the case that the patient will be returning to home care, it is very important to educate the family about how to treat their loved one's pressure ulcers. The cross-specialization wound team should train the caregiver in the proper way to turn the patient, how to properly dress the wound, how to properly nourish the patient, and how to deal with crisis, among other things.
As this is a very difficult undertaking, the caregiver may feel overburdened and depressed, so it may be best to bring in a psychological consult.
Wound intervention
Once the patient has reached the point that intervention is possible, there are many different options. For patients with Stages I and II ulcers, the wound care team should use guidelines established by the American Medical Directors Association (AMDA) for the treatment of these low-grade sores.
For those with Stage III or IV ulcers, most interventions will likely include surgery such as a tissue flap, free flap or other closure methods. A more recent intervention is Negative Pressure Wound Therapy, which is the application of topical negative pressure to the wound. This technique, developed by scientists at Wake Forest University, uses foam placed into the wound cavity which is then covered in a film which creates an airtight seal. Once this seal is established, the technician is able to remove exudate and other infectious materials in addition to aiding the body produce granulation tissue, the best bed for the creation of new skin.
There are, unfortunately, contraindications to the use of negative pressure therapy. Most deal with the unprepared patient, one who has not gone through the previous steps toward recovery, but there are also wound characteristics that bar a patient from participating: a wound with inadequate circulation, a raw debrided wound, a wound with necrotised tissue and eschar, and a fibrotic wound.
After Negative Pressure Wound Therapy, the patient should be reevaluated every two weeks to determine future therapy.
Prevention
It is common sense that prevention is better than cure - this applies particularly to pressure sores, which are painful and slow to heal, and most of which are definitely preventable if good clinical practice is followed. In the UK the Royal College of Nursing has published guidelines in 'Pressure ulcer risk assessment and prevention'.[11] It is important to identify those who are at risk and to intervene early with strategies for prevention, in the bed, wheelchair or chair, in the bath and on the commode - indeed, it is a requirement within the National Standards for Care Homes (UK) to do so:
"Standard 8.3 Service users are assessed, by a person trained to do so, to identify those service users who have developed, or are at risk of developing, pressure sores and appropriate intervention is recorded in the plan of care. 8.4 The incidence of pressure sores, their treatment and outcome, are recorded in the service user’s individual plan of care and reviewed on a continuing basis. 8.5 Equipment necessary for the promotion of tissue viability and prevention or treatment of pressure sores is provided."[12]
A wide variety of techniques are used to mitigate the risk of pressure ulcers in at risk groups including: nutritional supplements, topical skin protection and mechanical devices to mimic the effect of movement, such as alternating pressure mattresses. The most commonly used method of reducing the risk of pressure ulcers is regular nursing intervention and a 'turning schedule' to ensure the weight of the immobile patient is redistributed, reducing sustained pressure on a vulnerable area.
Complications
Pressure sores can trigger other ailments, cause patients considerable suffering, and be expensive to treat.[13] Some complications include autonomic dysreflexia, bladder distension, osteomyelitis, pyarthroses, sepsis, amyloidosis, anemia, urethral fistula, gangrene and very rarely malignant transformation (Marjolin's ulcer - secondary carcinomas in chronic wounds). Sores often recur because patients do not follow recommended treatment or develop seromas, hematomas, infections, or dehiscence. Paralytic patients are the most likely people to have pressure sores recur. In some cases, complications from pressure sores can be life-threatening. The most common causes of fatality stem from renal failure and amyloidosis.
See also
References
- ^ Galloway I (1899). "Conditions terminating in necrosis of the skin". A System of Medicine (Allbut C ed), Macmillan, London: 135.
- ^ Thomas DR, Diebold MR, Eggemeyer LM (2005). "A controlled, randomized, comparative study of a radiant heat bandage on the healing of stage 3-4 pressure ulcers: a pilot study". J Am Med Dir Assoc 6 (1): 46–9. doi:10.1016/j.jamda.2004.12.007. PMID 15871870.
- ^ a b Niezgoda JA, Mendez-Eastman S (2006). "The effective management of pressure ulcers". Adv Skin Wound Care 19 Suppl 1: 3–15. doi:10.1097/00129334-200601001-00001. PMID 16565615. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?an=00129334-200601001-00001.
- ^ "Pressure ulcers in America: prevalence, incidence, and implications for the future. An executive summary of the National Pressure Ulcer Advisory Panel monograph". Adv Skin Wound Care 14 (4): 208–15. 2001. PMID 11902346. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=1527-7941&volume=14&issue=4&spage=208.
- ^ Vanderwee K, Clark M, Dealey C, Gunningberg L & Defloor T (2007). "Pressure ulcer prevalence in Europe: a pilot study". Journal of Evaluation in Clinical Practice 13 (2): 227–235. doi:10.1111/j.1365-2753.2006.00684.x. PMID 17378869.
- ^ Tubaishat A, Anthony DM, Saleh M (2010). "Pressure ulcers in Jordan: A point prevalence study". Journal of Tissue Viability 19 (4): 132–136. doi:10.1016/j.jtv.2009.11.006. PMID 20036124.
- ^ Guy H (2004). "Preventing pressure ulcers: choosing a mattress". Professional Nurse 20 (4): 43–46. PMID 15624622.
- ^ "Antidecubitus Why?" (PDF). Antidecubitus Systems Matfresses Cushions. COMETE s.a.s.. http://www.cometemedicali.it/images/Brochure%20antidecubito%202005%20INGLESE.pdf. Retrieved 2009-10-02.
- ^ Bain DS, Ferguson-Pell M (2002). "Remote monitoring of sitting behavior of people with spinal cord injury". J Rehabil Res Dev 39 (4): 513–20. PMID 17638148.
- ^ "510(k)s Final Decisions Rendered for January 2004: DEVICE: MEDICAL MAGGOTS". FDA. http://www.fda.gov/cdrh/510k/sumjan04.html.
- ^ http://www.rcn.org.uk/__data/assets/pdf_file/0003/78501/001252.pdf
- ^ Pressure Relief and Wound Care Independent Living (UK)
- ^ Brem H, Kirsner RS, Falanga V (2004). "Protocol for the successful treatment of venous ulcers". Am. J. Surg. 188 (1A Suppl): 1–8. doi:10.1016/S0002-9610(03)00284-8. PMID 15223495.
External links
- Decubitus Ulcers Project at MSU
- Bed Sores and Pressure Ulcers
- CNN article
- USA today article
- Website of the European Wound Management Association (EWMA)
Cutaneous keratosis, ulcer, atrophy, and necrobiosis (L82–L94, 700–701.5) Epidermal thickening keratoderma: Keratoderma climactericum • Paraneoplastic keratoderma (Acrokeratosis paraneoplastica of Bazex ) • Aquagenic keratoderma · Drug-induced keratoderma · Paraneoplastic keratoderma • psoriasis (Keratoderma blennorrhagica)
keratosis: Seborrheic keratosis (Clonal seborrheic keratosis · Common seborrheic keratosis · Irritated seborrheic keratosis · Seborrheic keratosis with squamous atypia · Reticulated seborrheic keratosis · Dermatosis papulosa nigra) • Keratosis punctata of the palmar creases
other hyperkeratosis: Acanthosis nigricans (Confluent and reticulated papillomatosis) · Callus • Ichthyosis acquisita · Arsenical keratosis · Chronic scar keratosis · Hyperkeratosis lenticularis perstans · Hydrocarbon keratosis · Hyperkeratosis of the nipple and areola · Inverted follicular keratosis · Lichenoid keratosis · Multiple minute digitate hyperkeratosis · PUVA keratosis · Reactional keratosis · Stucco keratosis · Thermal keratosis · Viral keratosis · Warty dyskeratoma · Waxy keratosis of childhood
other hypertrophy: Keloid · Hypertrophic scar • Cutis verticis gyrata ·Necrobiosis/granuloma Granuloma annulare (Perforating, Generalized, Subcutaneous, Granuloma annulare in HIV disease, Localized granuloma annulare, Patch-type granuloma annulare) · Necrobiosis lipoidica · Annular elastolytic giant cell granuloma · Granuloma multiforme · Necrobiotic xanthogranuloma · Palisaded neutrophilic and granulomatous dermatitis · Rheumatoid nodulosis · Interstitial granulomatous dermatitis/Interstitial granulomatous drug reactionForeign body granulomaBeryllium granuloma • Mercury granuloma • Silica granuloma • Silicone granuloma • Zirconium granuloma • Soot tattoo • Tattoo • Carbon stainOther/ungroupedeosinophilic dermatosis (Granuloma faciale)Dermis/
localized CTDCutaneous lupus
erythematosusLocalized scleroderma (Localized morphea, Morphea–lichen sclerosus et atrophicus overlap, Generalized morphea, Atrophoderma of Pasini and Pierini, Pansclerotic morphea, Morphea profunda, Linear scleroderma)Atrophic/
atrophodermaLichen sclerosus · Anetoderma (Schweninger–Buzzi anetoderma, Jadassohn–Pellizzari anetoderma) · Atrophoderma of Pasini and Pierini · Acrodermatitis chronica atrophicans · Semicircular lipoatrophy · Follicular atrophoderma · Linear atrophoderma of MoulinKyrle disease · Reactive perforating collagenosis · Elastosis perforans serpiginosa · Perforating folliculitis · Acquired perforating dermatosisOtherCategories:- Skin conditions resulting from physical factors
- Traumatology


Wikimedia Foundation. 2010.