- Elbow
-
For other uses, see Elbow (disambiguation).
Elbow 
Latin articulatio cubiti Gray's subject #84 321 MeSH Elbow+joint The human elbow is the region surrounding the elbow-joint[1]—the ginglymus or hinge joint in the middle of the arm. Three bones form the elbow joint: the humerus of the upper arm, and the paired radius and ulna of the forearm.[2]
The bony prominence at the very tip of the elbow is the olecranon process of the ulna, and the inner aspect of the elbow is called the antecubital fossa.
Contents
Terminology
The now obsolete length unit ell relates closely to the elbow. This becomes especially visible when considering the Germanic origins of both words, Elle (ell, defined as the length of a male forearm from elbow to fingertips) and Ellbogen (elbow). It is unknown when or why the second "l" was dropped from English usage of the word.
Joint
The elbow-joint comprises three different portions. All these articular surfaces are enveloped by a common synovial membrane, and the movements of the whole joint should be studied together.
Joint From To Description humeroulnar joint trochlear notch of the ulna trochlea of humerus Is a simple hinge-joint, and allows of movements of flexion and extension only. humeroradial joint head of the radius capitulum of the humerus Is a hinge-joint. proximal radioulnar joint head of the radius radial notch of the ulna In any position of flexion or extension, the radius, carrying the hand with it, can be rotated in it. This movement includes pronation and supination. The combination of the movements of flexion and extension of the forearm with those of pronation and supination of the hand, which is ensured by the two being performed at the same joint, is essential to the accuracy of the various minute movements of the hand.
The hand is only directly articulated to the distal surface of the radius, and the ulnar notch on the lower end of the radius travels around the lower end of the ulna. The ulna is excluded from the wrist-joint by the articular disk.
Thus, rotation of the head of the radius around an axis passing through the center of the radial head of the humerus imparts circular movement to the hand through a very considerable arc.
Ligaments
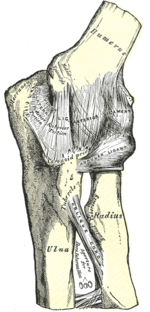
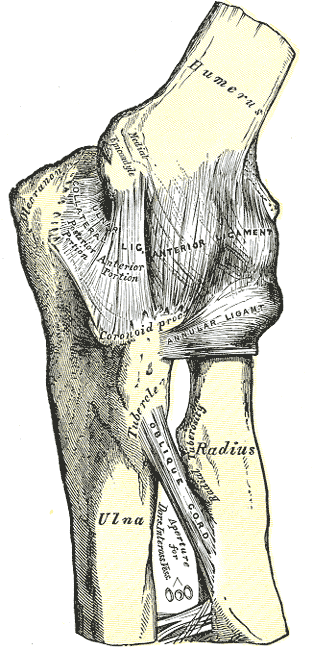
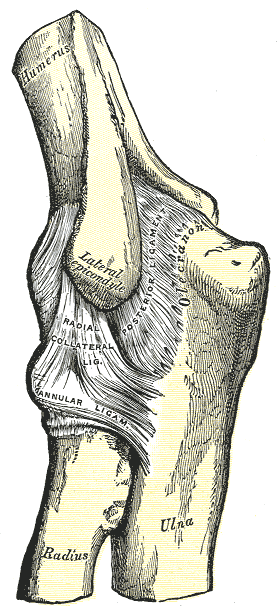
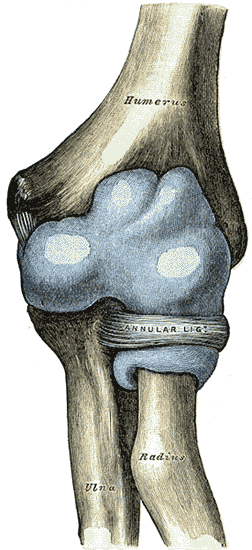
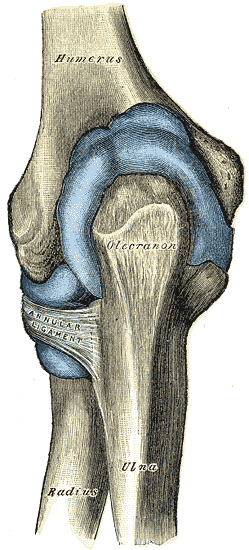
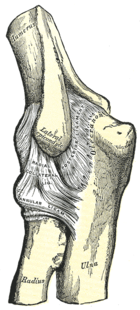 Left elbow-joint
Left elbow-joint
Left: anterior and ulnar collateral ligaments
Right: posterior and radial collateral ligamentsThe trochlea of the humerus is received into the semilunar notch of the ulna, and the capitulum of the humerus articulates with the fovea on the head of the radius. The articular surfaces are connected together by a capsule, which is thickened medially and laterally, and, to a less extent, in front and behind. These thickened portions are usually described as distinct ligaments.
The major ligaments are the ulnar collateral ligament, radial collateral ligament, and annular ligament.
Synovial membrane
The synovial membrane is very extensive. It extends from the margin of the articular surface of the humerus, and lines the coronoid, radial and olecranon fossæ on that bone; it is reflected over the deep surface of the capsule and forms a pouch between the radial notch, the deep surface of the annular ligament, and the circumference of the head of the radius. Projecting between the radius and ulna into the cavity is a crescentic fold of synovial membrane, suggesting the division of the joint into two; one the humeroradial, the other the humeroulnar.
Between the capsule and the synovial membrane are three masses of fat:
- the largest, over the olecranon fossa, is pressed into the fossa by the Triceps brachii during the flexion;
- the second, over the coronoid fossa,
- and the third, over the radial fossa, are pressed by the Brachialis into their respective fossæ during extension.
Muscles
The muscles in relation with the joint are:
- in front, the Brachialis, the Brachioradialis
- behind, the Triceps brachii and Anconæus
- laterally, the Supinator, and the common tendon of origin of the Extensor muscles
- medially, the common tendon of origin of the Flexor muscles, and the Flexor carpi ulnaris
Movements
Two main movements are possible at the elbow:
- The hinge-like bending and straightening (flexion and extension) between the humerus and the ulna.
- The complex action of turning the forearm over (pronation or supination) happens at the articulation between the radius and the ulna (this movement also occurs at the wrist joint).
- The hinge moves in only one plane.
In the anatomical position (with the forearm supine), the radius and ulna lie parallel to each other. During pronation, the ulna remains fixed, and the radius rolls around it at both the wrist and the elbow joints. In the prone position, the radius and ulna appear crossed.
Most of the force through the elbow joint is transferred between the humerus and the ulna. Very little force is transmitted between the humerus and the radius. (By contrast, at the wrist joint, most of the force is transferred between the radius and the carpus, with the ulna taking very little part in the wrist joint).
Carrying angle
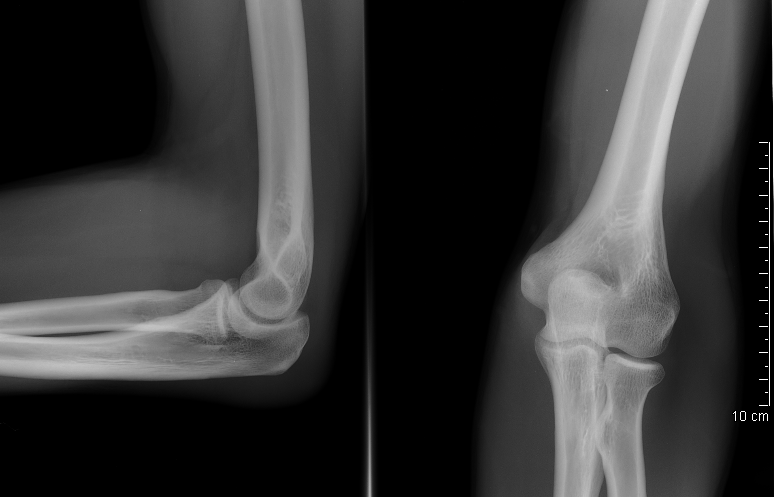
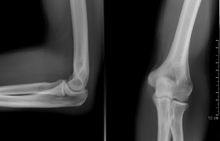 Normal radiograph; right picture of the straightened arm shows the carrying angle of the elbow
Normal radiograph; right picture of the straightened arm shows the carrying angle of the elbow
When the arm is extended, with the palm facing forward or up, the bones of the humerus and forearm are not perfectly aligned. The deviation from a straight line occurs in the direction of the thumb, and is referred to as the “carrying angle” (visible in the right half of the picture, right).
The carrying angle permits the arm to be swung without contacting the hips. Women on average have smaller shoulders and wider hips than men, which may necessitate a more acute carrying angle (i.e., less angle than that in male when measured from outside). There is, however, extensive overlap in the carrying angle between individual men and women, and a sex-bias has not been consistently observed in scientific studies.[3][4][5]
The angle is greater in the dominant limb than the non-dominant limb of both sexes,[6][7] suggesting that natural forces acting on the elbow modify the carrying angle. Developmental,[8] ageing and possibly racial influences add further to the variability of this parameter.
The carrying angle can influence how objects are held by individuals — those with a more extreme carrying angle may be more likely to pronate the forearm when holding objects in the hand to keep the elbow closer to the body.
The lateral elbow radiograph positioned to the right is a poor example of a lateral elbow joint. although, the radius and ulna are at true lateral position at the distal radio ulnar joint the humerus is not parallel to the image receptor resulting in a closing of the joint at the trochlear olecranon articulation, thus making the image non diagnostic.
Arteries and nerves
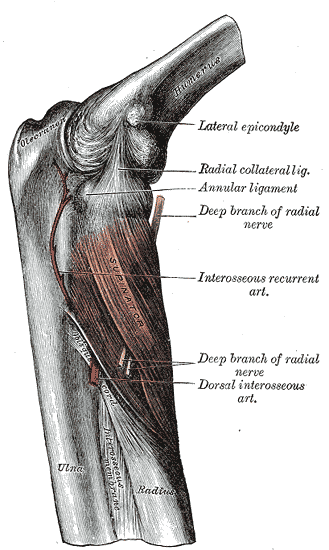
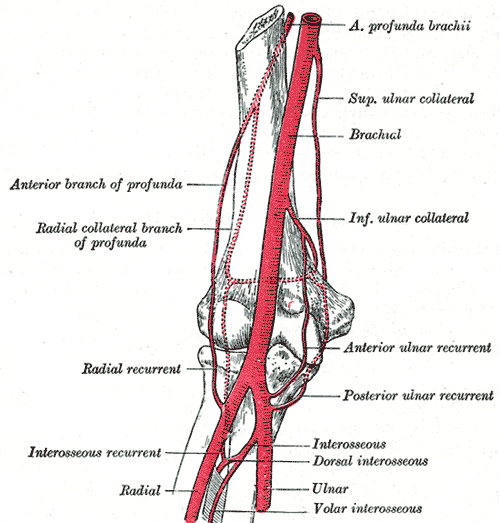
The arteries supplying the joint are derived from the anastomosis between the profunda and the superior and inferior ulnar collateral branches of the brachial, with the anterior, posterior, and interosseous recurrent branches of the ulnar, and the recurrent branch of the radial. These vessels form a complete anastomotic network around the joint.
The nerves of the joint are a twig from the ulnar, as it passes between the medial condyle and the olecranon; a filament from the musculocutaneous, and two from the median.
Diseases

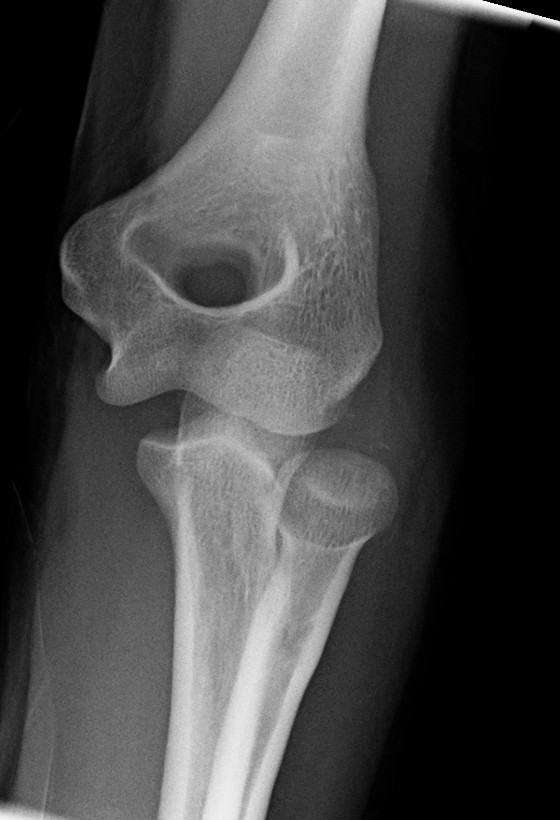
 Left: Lateral X ray of a dislocated right elbow
Left: Lateral X ray of a dislocated right elbow
Right: AP X ray of a dislocated right elbowThe types of disease most commonly seen at the elbow are due to injury.
Tendonitis
Two of the most common injuries at the elbow are overuse injuries: tennis elbow and golfer's elbow. Golfer's elbow involves the tendon of the common flexor origin which originates at the medial epicondyle of the humerus (the "inside" of the elbow). Tennis elbow is the equivalent injury, but at the common extensor origin (the lateral epicondyle of the humerus).
Fractures
There are three bones at the elbow joint, and any combination of these bones may be involved in a fracture of the elbow. Patients who are able to fully extend their arm at the elbow are unlikely to have a fracture (98% certainty) and an X-ray is not required as long as an olecranon fracture is ruled out.[9] Acute fractures may not be easily visible on X-ray.
Dislocation
Elbow dislocations constitute 10% to 25% of all injuries to the elbow. The elbow is one of the most commonly dislocated joints in the body, with an average annual incidence of acute dislocation of 6 per 100,000 persons.[10] Among injuries to the upper extremity, dislocation of the elbow is second only to a dislocated shoulder. A full dislocation of the elbow will require expert medical attention to re-align, and recovery can take approximately 8-14weeks. A small amount of people (10% or less) report near full recovery and very minimal permanent restriction, but most often a permanent restriction of 5-15% movement is common.
Infection
Infection of the elbow joint (septic arthritis) is uncommon. It may occur spontaneously, but may also occur in relation to surgery or infection elsewhere in the body (for example, endocarditis).
Arthritis
Elbow arthritis is usually seen in individuals with rheumatoid arthritis or after fractures that involve the joint itself. When the damage to the joint is severe, fascial arthroplasty or elbow joint replacement may be considered.[11]
Additional images
 Medial Humerus Radius Ulna Articulated
Medial Humerus Radius Ulna Articulated Left Human Posterior Distal Humerus Extended
Left Human Posterior Distal Humerus Extended Left Human Posterior Distal Humerus Flexed
Left Human Posterior Distal Humerus Flexed Capsule of elbow-joint (distended). Anterior aspect.
Capsule of elbow-joint (distended). Anterior aspect. Capsule of elbow-joint (distended). Posterior aspect.
Capsule of elbow-joint (distended). Posterior aspect. The Supinator. Posterior view.
The Supinator. Posterior view.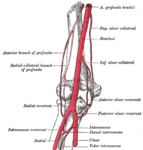 Diagram of the anastomosis around the elbow-joint.
Diagram of the anastomosis around the elbow-joint. Back of right upper extremity.
Back of right upper extremity. Close-up radiograph, right elbow-joint
Close-up radiograph, right elbow-joint Pathological fusion of three bones at elbow.
Pathological fusion of three bones at elbow.References
- ^ eMedicine/Stedman Medical Dictionary Lookup![dead link]
- ^ eMedicine/Stedman Medical Dictionary Lookup![dead link]
- ^ Steel, F; Tomlinson J (1958). "The 'carrying angle' in man". Journal of Anatomy 92 (2): 315–7. PMC 1249704. PMID 13525245. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1249704.
- ^ Van Roy, P, et al.; Baeyens, JP; Fauvart, D; Lanssiers, R; Clarijs, JP (2005). "Arthro-kinematics of the elbow: study of the carrying angle". Ergonomics 48 (11–14): 1645–56. doi:10.1080/00140130500101361. PMID 16338730.
- ^ Zampagni, M, et al.; Casino, D; Zaffagnini, S; Visani, AA; Marcacci, M (2008). "Estimating the elbow carrying angle with an electrogoniometer: acquisition of data and reliability of measurements". Orthopedics 31 (4): 370. PMID 19292279.
- ^ Paraskevas, G, et al.; Papadopoulos, A; Papaziogas, B; Spanidou, S; Argiriadou, H; Gigis, J (2004). "Study of the carrying angle of the human elbow joint in full extension: a morphometric analysis". Surgical and Radiologic Anatomy 26 (1): 19–23. doi:10.1007/s00276-003-0185-z. PMID 14648036.
- ^ Yilmaz, E, et al.; Karakurt, L; Belhan, O; Bulut, M; Serin, E; Avci, M (2005). "Variation of carrying angle with age, sex, and special reference to side". Orthopedics 28 (11): 1360–3. PMID 16295195.
- ^ Tukenmez, M, et al.; Demirel, H; Perçin, S; Tezeren, G (2004). "Measurement of the carrying angle of the elbow in 2,000 children at ages six and fourteen years". Acta Orthopaedica et Traumatologica Turcica 38 (4): 274–6. PMID 15618770.
- ^ Appelboam A, et al. (2008). "Elbow extension test to rule out elbow fracture: multicentre, prospective validation and observational study of diagnostic accuracy in adults and children". BMJ 337: a2428. doi:10.1136/bmj.a2428. PMC 2600962. PMID 19066257. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2600962.
- ^ Blakeney WG. Life in the Fast Lane: Elbow Dislocation
- ^ Summary - Total elbow joint replacement for elbow arthritis: Surgery with a dependable, time-tested prosthesis can lessen pain and improve function in elbows, especially those with rheumatoid arthritis
This article was originally based on an entry from a public domain edition of Gray's Anatomy. As such, some of the information contained within it may be outdated.
Human regional anatomy (TA A01.1) Head 
Neck Trunk Limbs Lower limb/
(see also leg)General anatomy: systems and organs, regional anatomy, planes and lines, superficial axial anatomy, superficial anatomy of limbsJoints and ligaments of upper limbs (TA A03.5, GA 3.313) Shoulder Elbow Radial collateralUlnar collateralAnular · Oblique cordForearm Joints of hand Dorsal radiocarpal/Palmar radiocarpal · Dorsal ulnocarpal/Palmar ulnocarpal · Ulnar collateral/Radial collateralRadiate carpal · Dorsal intercarpal · Palmar intercarpal · Interosseous intercarpal · Scapholunate · Pisiform joint (Pisohamate, Pisometacarpal)Collateral · PalmarCollateral · PalmarOtherM: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Categories:- Joints
- Upper limb anatomy
- Elbow








Wikimedia Foundation. 2010.