- Urethral stricture
-
Urethral stricture Classification and external resources 
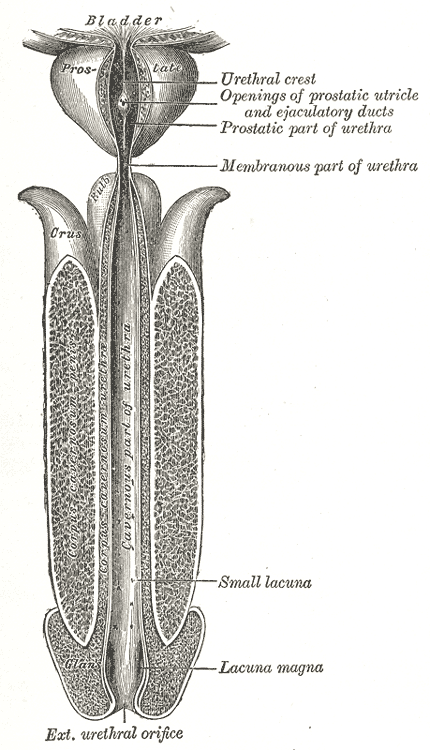
Urethra is tube at center.ICD-10 N35 ICD-9 598 DiseasesDB 13562 MedlinePlus 001271 eMedicine med/3075 MeSH C12.777.767.700.700 A urethral stricture is a narrowing of the urethra[1] caused by injury or disease such as urinary tract infections or other forms of urethritis.
Contents
Signs and symptoms
During the early stages of the condition, the subject may experience pain during urination and the inability to fully empty the bladder. It is not uncommon for the bladder's capacity to significantly increase due to this inability to completely void.
Urethral strictures may cause problems with urination, including in certain cases the complete inability to urinate, which is a medical emergency. Additionally, a urinary tract infection is often present at, or prior to initial diagnosis. Antibiotics, quinolone class anti-infective agents, or a combination of trimethoprim/sulfamethoxazole are often employed as the initial stage of treatment. Occasionally, some degree of relief from straining, or improvement of the urinary stream (depending on the severity of the stricture) occurs with antibiotic treatment due to the reduction of urethral inflammation.
- Obstructive voiding symptoms namely:
- Decreased force of urinary stream
- Incomplete emptying of the bladder
- Urinary terminal dribbling
- Urinary intermittency
- Deflected urinary stream
- Increased frequency of micturition
- Acute or chronic retention of urine
- Hydronephrotic signs due to back pressure
Complications
- Urinary retention
- Urethral diverticulum
- Periurethral abscess
- Urethral fistula
- Bilateral hydronephrosis
- Urinary infections
- Urinary calculus
- Hernia, haemorrhoids or Rectal prolapse from straining
Causes
Urethral strictures are generally caused by either injury-related trauma to the tract or by a viral or bacterial infection of the tract, often caused by certain sexually transmitted infections (STIs). The body's attempt to repair the damage caused by the injury or infection creates a buildup of scar tissue in the tract resulting in a significant narrowing or even closure of the passage. Instrumentation of the urethra, particularly before the advent of flexible uro-endoscopy, was (and remains) an important causative event.
Short strictures in the bulbar urethra, particularly between the proximal 1/3 and distal 2/3 of the bulb, may be congenital. They probably form as a membrane at the junction between the posterior and anterior urethral segments. It is not usually noticeable until later in life, as it fails to widen as the urethra does with growth, thus it only impedes urinary flow relative to the rest of the urethra after puberty. Moreover, the patient will often not "know any different", and so will not complain about poor flow.
The urethra runs between the legs very close to the skin, leaving it vulnerable to trauma. Simply falling off a bike and hitting between the legs may result in the formation of scar tissue within the urethra tract. This condition is often not found until the patient has problems urinating because these are painless growths of scar tissue.
Passage of kidney stones through the urethra can be painful and subsequently can lead to urethral strictures.
In infants and toddlers, can be as a result of inflammation following a circumcision and not noticeable until toilet training when a deflected stream is observed or when the child must strain to produce a urinary stream.
Diagnosis
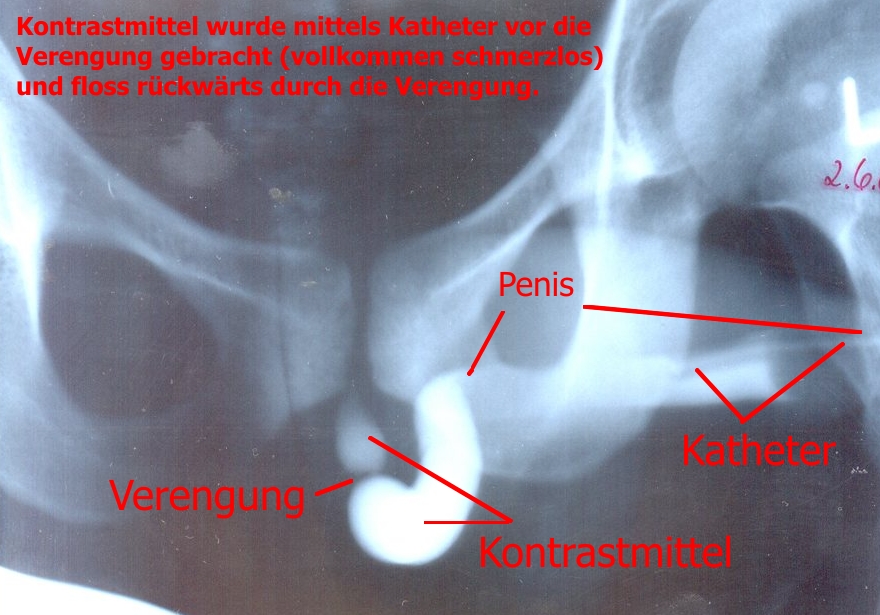
 Urethrography showing an urethra stricture in a man.
Urethrography showing an urethra stricture in a man.
- Cystoscopy
- Urethrography
Treatment
Instrumental treatment
- Urethral Dilatation with urethral sounds or filiform catheter (at prescribed intervals depending upon the severity and location of the stricture and the age/health of the patient) (office procedure - topical anesthetic)
- Bougies of increasing size (gum, elastic, continuous dilatation) (this is a seldom used method/treatment modality due to the increased possibility of infection, discomfort, and time involved)
- PRN Urethral Dilatation, usually every three to six months (office procedure - topical anesthetic)
Emergency treatment
- Dilatation with filiform and followers, and drainage of the urinary bladder through the follower catheter/lumen (Emergency Department or office-based procedure)
- Cystoscope guided insertion of filiform and followers, and drainage of the urinary bladder through the follower catheter/lumen (Emergency Department or office-based procedure)
- Visual Internal Urethrotomy with placement of Foley catheter and urinary drainage system for 7 days post-procedure (Operating Room based procedure under local or general anesthesia)
- Insertion of a suprapubic catheter with catheter drainage system (prior to surgical resolution) (Operating Room, Emergency Department or office-based procedure)
Surgery
- Visual internal urethrotomy
- Laser ablation urethrotomy
- Single-Stage urethroplasty (Penile flap or buccal mucosal graft)
- Multiple-Stage urethroplasty (Anastomotic urethroplasty)
- Johanson's urethroplasty (limited to the most severe cases, usually for traumatic stricture)
- Temporary urethral stent placement
- Permanent urethral stent placement [2]
Ongoing care
Because of the high rate of recurrence, Urethral Stricture Disease is often a lifetime-long diagnosis, even after successful surgical resolution of the stricture. Patients should be monitored (and treated) for urinary tract infection , including patient instruction/education on detection of the symptoms of UTI and undergo a non-invasive Uroflowmetric Study at annual intervals for at least five years (post surgery). Additionally, after age 40, it is recommended that the prostate be monitored (in males) at intervals as determined by the physician/practitioner overseeing the situation. Although no formal studies are available documenting this, there appears to be a slightly higher incidence of prostatitis in stricture patients versus the general population.[3] Patient education and counseling is an important aspect of the successful resolution, and continued care for the stricture patient.
References
- ^ "Urethral stricture: What causes it? - MayoClinic.com". Archived from the original on 2007-11-26. http://web.archive.org/web/20071126065424/http://www.mayoclinic.com/health/urethral-stricture/AN00805. Retrieved 2007-12-13.
- ^ Urolume Endoprosthesis
- ^ http://www.prostatitis.org/strictures.html
- MacDonald MF, Al-Qudah HS, Santucci RA (October 2005). "Minimal impact urethroplasty allows same-day surgery in most patients". Urology 66 (4): 850–3. doi:10.1016/j.urology.2005.04.057. PMID 16230151.
- Al-Qudah HS, Cavalcanti AG, Santucci RA (2005). "Early catheter removal after anterior anastomotic (3 days) and ventral buccal mucosal onlay (7 days) urethroplasty". International Braz J Urol 31 (5): 459–63; discussion 464. PMID 16255792. http://www.brazjurol.com.br/september_october_2005/AlQudah_ing_459_464.htm.
- Santucci RA, McAninch JW, Mario LA, et al. (July 2004). "Urethroplasty in patients older than 65 years: indications, results, outcomes and suggested treatment modifications". J Urol. 172 (1): 201–3. doi:10.1097/01.ju.0000128810.86535.be. PMID 15201773.
- Kizer WS, Armenakas NA, Brandes SB, Cavalcanti AG, Santucci RA, Morey AF (April 2007). "Simplified reconstruction of posterior urethral disruption defects: limited role of supracrural rerouting". J Urol. 177 (4): 1378–81; discussion 1381–2. doi:10.1016/j.juro.2006.11.036. PMID 17382736.
- Al-Qudah HS, Santucci RA (2005). "Extended complications of urethroplasty". Int Braz J Urol. 31 (4): 315–23; discussion 324–5. PMID 16137399. http://www.brazjurol.com.br/july_august_2005/Al-Qudah_ing_315_325.htm.
- Santucci RA, Mario LA, McAninch JW (April 2002). "Anastomotic urethroplasty for bulbar urethral stricture: analysis of 168 patients". J Urol. 167 (4): 1715–9. doi:10.1016/S0022-5347(05)65184-1. PMID 11912394.
Essentials of Surgery 4th Edition 2007 by Professor Muhammad Shamim
External links
Urinary system · Pathology · Urologic disease / Uropathy (N00–N39, 580–599) Abdominal Primarily
nephrotic.3 Mesangial proliferative · .4 Endocapillary proliferative .5/.6 Membranoproliferative/mesangiocapillaryBy conditionType III RPG/Pauci-immuneTubulopathy/
tubulitisAny/allAny/allGeneral syndromesOtherUreterPelvic UrethraUrethritis (Non-gonococcal urethritis) · Urethral syndrome · Urethral stricture/Meatal stenosis · Urethral caruncleAny/all Obstructive uropathy · Urinary tract infection · Retroperitoneal fibrosis · Urolithiasis (Bladder stone, Kidney stone, Renal colic) · Malacoplakia · Urinary incontinence (Stress, Urge, Overflow)Categories:- Urethra disorders
- Obstructive voiding symptoms namely:
Wikimedia Foundation. 2010.