- Burn
-
Burn Classification and external resources 
Second-degree burn of the handICD-10 T20-T31 ICD-9 940-949 MeSH D002056 A burn is a type of injury to flesh caused by heat, electricity, chemicals, light, radiation or friction.[1][2][3] Most burns affect only the skin (epidermal tissue and dermis). Rarely, deeper tissues, such as muscle, bone, and blood vessels can also be injured. Burns may be treated with first aid, in an out-of-hospital setting, or may require more specialised treatment such as those available at specialised burn centers.
Managing burn injuries properly is important because they are common, painful and can result in disfiguring and disabling scarring, amputation of affected parts or death in severe cases. Complications such as shock, infection, multiple organ dysfunction syndrome, electrolyte imbalance and respiratory distress may occur. The treatment of burns may include the removal of dead tissue (debridement), applying dressings to the wound, fluid resuscitation, administering antibiotics and skin grafting.
While large burns can be fatal, modern treatments developed in the last 60 years have significantly improved the prognosis of such burns, especially in children and young adults.[4][5] In the United States, approximately 4 out of every 100 people with injuries from burns will succumb to their injuries. The majority of these fatalities occur either at the scene or enroute to hospital.[6]
Contents
Classification
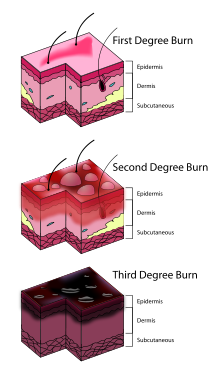 Three degrees of burns
Three degrees of burns
Burns can be classified by mechanism of injury, depth, extent and associated injuries and comorbidities.
By depth
Currently, burns are described according to the depth of injury to the dermis and are loosely classified into first, second, third and fourth degrees. This system was devised by the French barber-surgeon Ambroise Pare and remains in use today.[7]
It is often difficult to accurately determine the depth of a burn. This is especially so in the case of second degree burns, which can continue to evolve over time. As such, a second-degree partial-thickness burn can progress to a third-degree burn over time even after initial treatment. Distinguishing between the superficial-thickness burn and the partial-thickness burn is important, as the former may heal spontaneously, whereas the latter often requires surgical excision and skin grafting.
The following tables describe degrees of burn injury under this system as well as provide pictorial examples.
Nomenclature Layer involved Appearance Texture Sensation Time to healing Complications Example First degree Epidermis Redness (erythema) Dry Painful 1wk or less None 
Second degree (superficial partial thickness) Extends into superficial (papillary) dermis Red with clear blister. Blanches with pressure Moist Painful 2-3wks Local infection/cellulitis 
Second degree (deep partial thickness) Extends into deep (reticular) dermis Red-and-white with bloody blisters. Less blanching. Moist Painful Weeks - may progress to third degree Scarring, contractures (may require excision and skin grafting) 
Third degree (full thickness) Extends through entire dermis Stiff and white/brown Dry, leathery Painless Requires excision Scarring, contractures, amputation 
Fourth degree Extends through skin, subcutaneous tissue and into underlying muscle and bone Black; charred with eschar Dry Painless Requires excision Amputation, significant functional impairment By severity
In order to determine the need for referral to a specialised burn unit, the American Burn Association devised a classification system to aid in the decision-making process. Under this system, burns can be classified as major, moderate and minor. This is assessed based on a number of factors, including total body surface area (TBSA) burnt, the involvement of specific anatomical zones, age of the person and associated injuries.[6]
Major
Major burns are defined as:
- Age 10-50yrs: partial thickness burns >25% of total body surface area
- Age <10 or >50: partial thickness burns >20% of total body surface area
- Full thickness burns >10%
- Burns involving the hands, face, feet or perineum[8]
- Burns that cross major joints
- Circumferential burns to any extremity
- Any burn associated with inhalational injury
- Electrical burns
- Burns associated with fractures or other trauma
- Burns in infants and the elderly
- Burns in persons at high-risk of developing complications
These burns typically require referral to a specialised burn treatment center.
Moderate
Moderate burns are defined as:
- Age 10-50yrs: partial thickness burns involving 15-25% of total body surface area
- Age <10 or >50: partial thickness burns involving 10-20% of total body surface area
- Full thickness burns involving 2-10% of total body surface area
Persons suffering these burns often need to be hospitalised for burn care.
Minor
Minor burns are:
- Age 10-50yrs: partial thickness burns <15% of total body surface area
- Age <10 or >50: partial thickness burns involving <10% of total body surface area
- Full thickness burns <2% of total body surface area, without associated injuries
These burns usually do not require hospitalization.
By surface area
Burns can also be assessed in terms of total body surface area (TBSA), which is the percentage affected by partial thickness or full thickness burns. First degree (erythema only, no blisters) burns are not included in this estimation. The rule of nines is used as a quick and useful way to estimate the affected TBSA. More accurate estimation can be made using Lund & Browder charts which take into account the different proportions of body parts in adults and children.[9] The size of a person's hand print (palm and fingers) is approximately 1% of their TBSA. The actual mean surface area is 0.8% so using 1% will slightly overestimate the size.[10]
Burns of 10% in children or 15% in adults (or greater) are potentially life threatening injuries (because of the risk of hypovolaemic shock) and should have formal fluid resuscitation and monitoring in a burns unit. Burns units will use surface area to predict severity and mortality, using a methodology such as the Baux score.
Cause
Burns are caused by a wide variety of substances and external sources such as exposure to chemicals, friction, electricity, radiation, and heat.
Chemical
Most chemicals that cause chemical burns are strong acids or bases.[11] Chemical burns can be caused by caustic chemical compounds such as sodium hydroxide or silver nitrate, and acids such as sulfuric acid.[12] Hydrofluoric acid can cause damage down to the bone and its burns are sometimes not immediately evident.[13]
Electrical
Main article: Electrical burnElectrical burns are caused by either an electric shock or an uncontrolled short circuit (A burn from a hot, electrified heating element is not considered an electrical burn). Common occurrences of electrical burns include workplace injuries, or being defibrillated or cardioverted without a conductive gel. Lightning is also a rare cause of electrical burns.
Since normal physiology involves a vast number of applications of electrical forces, ranging from neuromuscular signaling to coordination of wound healing, biological systems are very vulnerable to application of supraphysiologic electric fields. Some electrocutions produce no external burns at all, as very little current is required to cause fibrillation of the heart muscle. Therefore, even when the injury does not involve any visible tissue damage, electrical shock survivors may experience significant internal injury.[14] The internal injuries sustained may be disproportionate to the size of the burns seen (if any), and the extent of the damage is not always obvious. Such injuries may lead to cardiac arrhythmias, cardiac arrest, and unexpected falls with resultant fractures or dislocations.[15]
The true incidence of electrical burn injury is unknown. In one study of 220 deaths due to electrical injury, 40% of those associated with low-voltage (<500 AC volts) injury demonstrated no skin burns or marks whatsoever. Most household electrical burns occur at 110 AC volts. This is sufficient to cause cardiac arrest and ventricular fibrillation but generates relatively low heat energy deposit into skin, thus producing few or no burn marks at all.[16]
Radiation
Radiation burns are caused by protracted exposure to UV light (as from the sun), tanning booths, radiation therapy (in people undergoing cancer therapy), sunlamps, radioactive fallout, and X-rays. By far the most common burn associated with radiation is sun exposure, specifically two wavelengths of light UVA, and UVB, the latter being more dangerous. Tanning booths also emit these wavelengths and may cause similar damage to the skin such as irritation, redness, swelling, and inflammation. More severe cases of sun burn result in what is known as sun poisoning or "heatstroke". Microwave burns are caused by the thermal effects of microwave radiation.
Scalding

Scalding (from the Latin word calidus, meaning hot[17]) is caused by hot liquids (water or oil) or gases (steam), most commonly occurring from exposure to high temperature tap water in baths or showers or spilled hot drinks.[18] A so called immersion scald is created when an extremity is held under the surface of hot water, and is a common form of burn seen in child abuse.[19] A blister is a "bubble" in the skin filled with serous fluid as part of the body's reaction to the heat and the subsequent inflammatory reaction. The blister "roof" is dead and the blister fluid contains toxic inflammatory mediators. Scald burns are more common in children, especially "spill scalds" from hot drinks and bath water scalds.
Pathophysiology
Following a major burn injury, heart rate and peripheral vascular resistance increase. This is due to the release of catecholamines from injured tissues, and the relative hypovolemia that occurs from fluid volume shifts. Initially cardiac output decreases. At approximately 24 hours after burn injuries, cardiac output returns to normal if adequate fluid resuscitation has been given. Following this, cardiac output increases to meet the hypermetabolic needs of the body.
The effects of high temperature on tissue include speeding chemical reactions and unfolding (denaturing) proteins. [20]
Management
The resuscitation and stabilization phase begins with the reassessment of the injured person's airway, breathing and circulatory state. Appropriate interventions should be initiated to stabilize these. This may involve aggressive fluid resuscitation and, if inhalation injury is suspected, intubation. Once the injured person is stabilized, attention is turned to the care of the burn wound itself. Until then, it is advisable to cover the burn wound with a clean and dry sheet or dressing.
Early cooling reduces burn depth and pain, but care must be taken as uncontrolled cooling can result in hypothermia.[21]
Intravenous fluids
Children with >10% total body surface area burns, and adults with >15% total body surface area burns need formal fluid resuscitation and monitoring (blood pressure, pulse rate, temperature and urine output).[22] Once the burning process has been stopped, the injured person should be volume resuscitated according to the Parkland formula. This formula calculates the amount of Ringer's lactate required to be administered over the first 24 hours post-burn.
Parkland formula: 4mL x (percentage of total body-surface-area sustaining non-superficial burns) x (person's weight in kgs).
Half of this total volume should be administered over the first eight hours, with the remainder given over the following 16 hours. It is important to note that this time frame is calculated from the time at which the burn is sustained, and not the time at which fluid resuscitation is begun. Children also require the addition of maintenance fluid volume. Such injuries can disturb a person's osmotic balance.[23] Inhalation injuries in conjunction with thermal burns initially require up to 40–50% more fluid.
The formula is a guide only and infusions must be tailored to the urine output and central venous pressure. Inadequate fluid resuscitation may cause renal failure and death, but over-resuscitation also causes morbidity.
Wound care
 Second degree heat burn, approx 1cm across centre, 6 days after burn.
Second degree heat burn, approx 1cm across centre, 6 days after burn.Debridement cleaning and then dressings are important aspects of wound care. The wound should then be regularly re-evaluated until it is healed.[3] In the management of first and second degree burns little quality evidence exists to determine which type of dressing should be used.[24] Silver sulfadiazine (Flamazine) is not recommended as it potentially prolongs healing time[24] while biosynthetic dressings may speed healing.[25]
Antibiotics
Intravenous antibiotics may improve survival in those with large and severe burns. However due to the poor quality of the evidence, routine use is not currently recommended.[26]
Analgesics
A number of different options are used for pain management. These include simple analgesics (such as ibuprofen and acetaminophen) and narcotics. A local anesthetic may help in managing pain of minor first-degree and second-degree burns.[27]
Surgery
Wounds requiring surgical closure with skin grafts or flaps should be dealt with as early as possible.[3] Circumferential burns of digits, limbs or the chest may need urgent surgical release of the burnt skin (escharotomy) to prevent problems with distal circulation or ventilation.[3]
Alternative treatments
Hyperbaric oxygenation has not been shown to be a useful adjunct to traditional treatments.[28] Honey has been used since ancient times to aid wound healing and may be beneficial in first and second degree burns, but may cause infection.[29]
Complications
Infection is a major complication of burns. Infection is linked to impaired resistance from disruption of the skin's mechanical integrity and generalized immune suppression. The skin barrier is replaced by eschar. This moist, protein rich avascular environment encourages microbial growth. Migration of immune cells is hampered, and there is a release of intermediaries that impede the immune response. Eschar also restricts distribution of systemically administered antibiotics because of its avascularity.
Risk factors of burn wound infection include:
- Burn > 30% BSA
- Full-thickness burn
- Extremes in age (very young, very old)
- Preexisting disease e.g. diabetes
- Virulence and antibiotic resistance of colonizing organism
- Failed skin graft
- Improper initial burn wound care
- Prolonged open burn wound
Burn wounds are prone to tetanus. A tetanus booster shot is required if individual has not been immunized within the last 5 years.
Circumferential burns of extremities may compromise circulation. Elevation of limb may help to prevent dependent edema. An Escharotomy may be required.
Acute Tubular Necrosis of the kidneys can be caused by myoglobin and hemoglobin released from damaged muscles and red blood cells. This is common in electrical burns or crush injuries where adequate fluid resuscitation has not been achieved.
Prognosis
The outcome of any injury or disease depends on three things: the nature of the injury, the nature of the injured or ill person and the treatment available. In terms of injury factors in burns, the prognosis depends primarily on total body surface area percentage and the age of the person. The presence of smoke inhalation injury, other significant injuries such as long bone fractures and serious co-morbidities (heart disease, diabetes, psychiatric illness, suicidal intent etc.) will also adversely influence prognosis. Advances in resuscitation, surgical management, intensive care, control of infection, control of the hyper-metabolic response and rehabilitation have resulted in dramatic improvements in burn mortality and morbidity in the last 60 years. The modified Baux score determines the futility point for major burn injury. The Baux score is determined by adding the size of the burn (% TBSA) to the age of the patient. In most burn units a score of 140 or greater is a non-survivable injury, and comfort care should be offered. In children all burn injuries less than 100% TBSA should be considered a survivable injury.
Epidemiology
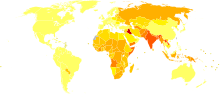 Disability-adjusted life years for fires per 100,000 inhabitants in 2004.[30]no data< 5050-100100-150150-200200-250250-300300-350350-400400-450450-500500-600> 600
Disability-adjusted life years for fires per 100,000 inhabitants in 2004.[30]no data< 5050-100100-150150-200200-250250-300300-350350-400400-450450-500500-600> 600According to the American Burn Association,[6] an estimated 500,000 burn injuries receive medical treatment yearly in the United States.[7]
The 2009 National Burn Repository reports the most common cause of burns as direct fire/flame (43%) followed by scalds (30%). Scald injuries were the predominant cause in children under the age of 5. Burns sustained at home accounted for 65.5% of all burn injuries in the United States that year, and had a mortality rate of 4% overall. This mortality rate was directly associated with advancing age, burn size, the presence of inhalational injury and the female sex.[6] It is estimated that approximately 75% of deaths from burns and fires in the United States occur either at the scene of the incident or enroute to medical facilities.
Demographically, people sustaining burns in the United States tended to be male (70%) and to have suffered their injuries in a residential setting (43%).[6] The highest incidence of burns occurs in the 18-35yr old age group, while the highest incidence of scalds occurs in children 1-5yrs old and adults over 65.
In India about 700,000 people a year are admitted to hospital, though very few are looked after in specialist burn units.[31]
About 90% of burns occur in the developing world and 70% of these are in children. Survival of injuries greater than 40% total body surface area is rare in the developing world.[32]
References
- ^ MedlinePlus. "Burns". http://www.nlm.nih.gov/medlineplus/burns.html. Retrieved 2010-09-22.
- ^ WebMD (January 7, 2009). "Burns-Topic Overview". firstaid&emergencies. http://firstaid.webmd.com/tc/burns-topic-overview. Retrieved 2010-09-22.
- ^ a b c d Total Burn Care, 3rd Edition, Edited by David Herndon, Saunders, 2007.
- ^ Total Burn Care 3rd Edition. Editied David Herndon. Chapter 1 [1] Accessed January 8, 2010
- ^ Sevitt S (May 1979). "A review of the complications of burns, their origin and importance for illness and death". J Trauma 19 (5): 358–69. doi:10.1097/00005373-197905000-00010. PMID 448773.
- ^ a b c d e "American Burn Association". http://www.ameriburn.org/resources_factsheet.php.
- ^ a b Ron Walls MD; John J. Ratey MD; Robert I. Simon MD (2009). Rosen's Emergency Medicine: Expert Consult Premium Edition - Enhanced Online Features and Print (Rosen's Emergency Medicine: Concepts & Clinical Practice (2v.)). St. Louis: Mosby. ISBN 0-323-05472-2.
- ^ http://www.burnsurgery.com/Modules/BurnWound%201/sect_IV.htm SECTION IV: INITIAL WOUND MANAGEMENT
- ^ Ames WA (1999). "Management of the Major Burn". Update in Anaesthesia (Nuffield Department of Anaesthesia, Oxford, UK) (10). http://www.nda.ox.ac.uk/wfsa/html/u10/u1010_01.htm. Retrieved 2010-01-22.
- ^ Perry RJ, Moore CA, Morgan BD, Plummer DL (May 1996). "Determining the approximate area of a burn: an inconsistency investigated and re-evaluated". BMJ 312 (7042): 1338. PMC 2350999. PMID 8646048. http://www.bmj.com/content/312/7042/1338.full.
- ^ Chemical Burn Causes emedicine Health Accessed February 24, 2008
- ^ Chemical Burn Causes eMedicine Accessed February 24, 2008
- ^ Hydrofluoric Acid Burns emedicine Accessed February 24, 2008
- ^ Mechanism of Electrical Injury Chicago Electrical Trauma Research Institute Accessed April 27, 2010
- ^ Electrical Burns: First Aid Mayo Clinic Accessed February 24, 2008
- ^ Wright RK, Davis JH: The investigation of electrical deaths: A report of 220 fatalities. J Forensic Sci 25:514, 1980
- ^ Mosby’s Medical, Nursing and Allied Health Dictionary, Fourth Edition, Mosby-Year Book Inc., 1994, p. 1395
- ^ Scald and Burn Care, Public Education City of Rochester Hills Accessed February 24, 2008
- ^ Allasio D, Fischer H (May 2005). "Immersion scald burns and the ability of young children to climb into a bathtub". Pediatrics 115 (5): 1419–21. doi:10.1542/peds.2004-1550. PMID 15867058.
- ^ Ashley G. Smart: "Kinetic Experiments Shed Light on Protein-folding Thermodynamics", Physics Today August 2011
- ^ Tintinalli, Judith E. (2010). Emergency Medicine: A Comprehensive Study Guide (Emergency Medicine (Tintinalli)). New York: McGraw-Hill Companies. ISBN 0-07-148480-9.
- ^ Herndon, David N. (2007). "Chapter 9 Total Burn Care". Total Burn Care. Philadelphia: Saunders. pp. 880. ISBN 1-4160-3274-6.
- ^ Lee JA (December 1981). "Sydney Ringer (1834-1910) and Alexis Hartmann (1898-1964)" (PDF). Anaesthesia 36 (12): 1115–21. doi:10.1111/j.1365-2044.1981.tb08698.x. PMID 7034584. http://www.dr-green.co.uk/PDFs/Ringer%20and%20Hartmann.pdf.
- ^ a b Wasiak J, Cleland H, Campbell F (2008). Wasiak, Jason. ed. "Dressings for superficial and partial thickness burns". Cochrane Database Syst Rev (4): CD002106. doi:10.1002/14651858.CD002106.pub3. PMID 18843629.
- ^ Hubley P (July 2009). "Review: evidence on dressings for superficial burns is of poor quality". Evid Based Nurs 12 (3): 78. doi:10.1136/ebn.12.3.78. PMID 19553415.
- ^ Avni T, Levcovich A, Ad-El DD, Leibovici L, Paul M (2010). "Prophylactic antibiotics for burns patients: systematic review and meta-analysis". BMJ 340: c241. doi:10.1136/bmj.c241. PMC 2822136. PMID 20156911. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2822136.
- ^ Minor Burns quickcare.org Accessed February 25, 2008
- ^ Villanueva E, Bennett MH, Wasiak J, Lehm JP (2004). Wasiak, Jason. ed. "Hyperbaric oxygen therapy for thermal burns". Cochrane Database Syst Rev (3): CD004727. doi:10.1002/14651858.CD004727.pub2. PMID 15266540.
- ^ Jull AB, Rodgers A, Walker N (2008). Jull, Andrew B. ed. "Honey as a topical treatment for wounds". Cochrane Database Syst Rev (4): CD005083. doi:10.1002/14651858.CD005083.pub2. PMID 18843679.
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Retrieved Nov. 11, 2009.
- ^ Bhattacharya S. Principles and Practice of Burn Care. Indian J Plast Surg 2009;42:282-3
- ^ Potokar T, Chamania S, Ali S. International network for training, education and research in burns. Indian J Plast Surg 2007;40:107
Further reading
Herndon, David (2007). Total Burn Care. Saunders. ISBN 978-1-4160-3274-8.
External links
- NHS Choices - Burns and Scalds
- British Burn Association
- American Burn Association
- European Burn Association
- The UK National Burn Care Government Review
- Cochrane Injuries Group, systematic reviews on the prevention, treatment and rehabilitation of traumatic injury
General wounds and injuries (T08-T35, 870-949) General Wound/
traumaBlister (Blood blister • Coma blister • Delayed blister • Edema blister • Fracture blister • Friction blister • Sucking blister)
Bruise/Hematoma/Ecchymosis (Battle's sign, Raccoon eyes, Black eye, Subungual hematoma, Cullen's sign, Grey Turner's sign, Retroperitoneal hemorrhage)
Animal bite: Insect bite · Spider biteAnimal bite: Snakebite · Lizard bite
Ballistic traumaForeign body Other By region Categories:- Skin conditions resulting from physical factors
- Medical emergencies
- Injuries









Wikimedia Foundation. 2010.