- Acid–base homeostasis
-
Blood gas, acid-base, & gas exchange terms PaO2 Arterial oxygen tension, or partial pressure PAO2 Alveolar oxygen tension, or partial pressure PACO2 Arterial carbon dioxide tension, or partial pressure PaCO2 Alveolar carbon dioxide tension, or partial pressure PvO2 Oxygen tension of mixed venous blood P(A-a)O2 Alveolar-arterial oxygen tension difference. The term formerly used (A-a DO2) is discouraged. P(a/A)O2 Alveolar-arterial tension ratio; PaO2:PAO2 The term oxygen exchange index describes this ratio. C(a-v)O2 Arteriovenous oxygen content difference SaO2 Oxygen saturation of the hemoglobin of arterial blood SpO2 Oxygen saturation as measured by pulse oximetry CaO2 Oxygen content of arterial blood pH Symbol relating the hydrogen ion concentration or activity of a solution to that of a standard solution; approximately equal to the negative logarithm of the hydrogen ion concentration. pH is an indicator of the relative acidity or alkalinity of a solution Acid dissociation constant
Acid-base extraction
Acid–base reaction
Acid–base titration
Dissociation constant
Acidity function
Buffer solutions
pH
Proton affinity
Self-ionization of waterAcid types Brønsted · Lewis · Mineral
Organic · Strong
Superacids · WeakBase types Brønsted · Lewis · Organic
Strong · Superbases
Non-nucleophilic · WeakAcid–base homeostasis is the part of human homeostasis concerning the proper balance between acids and bases, in other words, the pH. The body is very sensitive to its pH level, so strong mechanisms exist to maintain it. Outside the acceptable range of pH, proteins are denatured and digested, enzymes lose their ability to function, and death may occur.
Contents
Mechanism

The body's acid–base balance is tightly regulated. Several buffering agents that reversibly bind hydrogen ions and impede any change in pH exist. Extracellular buffers include bicarbonate and ammonia, whereas proteins and phosphate act as intracellular buffers. The bicarbonate buffering system is especially key, as carbon dioxide (CO2) can be shifted through carbonic acid (H2CO3) to hydrogen ions and bicarbonate (HCO3-) as shown below.
Acid–base imbalances that overcome the buffer system can be compensated in the short term by changing the rate of ventilation. This alters the concentration of carbon dioxide in the blood, shifting the above reaction according to Le Chatelier's principle, which in turn alters the pH. For instance, if the blood pH drops too low (acidemia), the body will compensate by increasing breathing, expelling CO2, and shifting the above reaction to the left such that less hydrogen ions are free; thus the pH will rise back to normal. For alkalemia, the opposite occurs.
The kidneys are slower to compensate, but renal physiology has several powerful mechanisms to control pH by the excretion of excess acid or base. In responses to acidosis, tubular cells reabsorb more bicarbonate from the tubular fluid, collecting duct cells secrete more hydrogen and generate more bicarbonate, and ammoniagenesis leads to increased formation of the NH3 buffer. In responses to alkalosis, the kidney may excrete more bicarbonate by decreasing hydrogen ion secretion from the tubular epithelial cells, and lowering rates of glutamine metabolism and ammonia excretion.
Imbalance
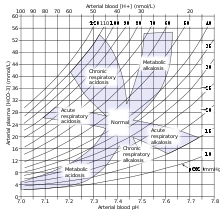
Acid–base imbalance occurs when a significant insult causes the blood pH to shift out of the normal range (7.35 to 7.45). In the fetus, the normal range differs based on which umbilical vessel is sampled (umbilical vein pH is normally 7.25 to 7.45; umbilical artery pH is normally 7.18 to 7.38).[1] An excess of acid in the blood is called acidemia and an excess of base is called alkalemia. The process that causes the imbalance is classified based on the etiology of the disturbance (respiratory or metabolic) and the direction of change in pH (acidosis or alkalosis). There are four basic processes: metabolic acidosis, respiratory acidosis, metabolic alkalosis, and respiratory alkalosis. One or a combination may occur at any given time.
References
- ^ Yeomans, ER; Hauth, JC; Gilstrap, LC III; Strickland DM (1985). "Umbilical cord pH, PCO2, and bicarbonate following uncomplicated term vaginal deliveries (146 infants)". Am J Obstet Gynecol 151: 798–800.
External links
- Stewart's original text at acidbase.org
- On-line text at AnaesthesiaMCQ.com
- Overview at kumc.edu
- Tutorial at acid-base.com
- Online acid–base physiology text
- Diagnoses at lakesidepress.com
- Interpretation at nda.ox.ac.uk
Cardiopulmonary therapy Diagnostic Pulmonary function testing • PolysomnographyDisease Therapy Hyperinflation therapy • Pulmonary hygiene • Mechanical ventilation • Oxygen therapySee also Urinary system, physiology: renal physiology and acid-base physiology Filtration Hormones affecting filtration Secretion/clearance Reabsorption Endocrine Assessing Renal function/
Measures of dialysisGlomerular filtration rate · Creatinine clearance · Renal clearance ratio · Urea reduction ratio · Kt/V · Standardized Kt/V · Hemodialysis product · PAH clearance (Effective renal plasma flow · Extraction ratio)Acid-base physiology Fluid balance · Darrow Yannet diagram
Body water: Intracellular fluid/Cytosol · Extracellular fluid · (Interstitial fluid · Plasma · Transcellular fluid)
Base excess · Davenport diagram · Anion gap · Arterial blood gas · Winter's formulaBuffering/compensation Other Human homeostasis Blood composition Blood sugar · Osmoregulation · Pressure: Renin-angiotensin system · Acid-base · Fluid balance · HemostasisOther Categories:- Respiratory therapy
- Human homeostasis
- Acid-base physiology
- Acid-base disturbances
- Equilibrium chemistry
-


Wikimedia Foundation. 2010.