- Scar
-
"Scars" redirects here. For the 1998 video game, see S.C.A.R.S. (video game)."Scarring" redirects here. For the act of inflicting scars, see Scarification.This article is about scar tissue. For other uses, see Scar (disambiguation).
Scar Classification and external resources 
A minor scar from a cut to the forearm, approx. one year since the wound.ICD-10 L90.5 MeSH D002921 Scars are areas of fibrous tissue (fibrosis) that replace normal skin after injury. A scar results from the biological process of wound repair in the skin and other tissues of the body. Thus, scarring is a natural part of the healing process. With the exception of very minor lesions, every wound (e.g. after accident, disease, or surgery) results in some degree of scarring. An exception to this is animals with regeneration, which do not form scars and the tissue will grow back exactly as before.
Sherratt et al, explain that scar tissue is the same protein (collagen) as the tissue that it replaces,[1] but the fiber composition of the protein is different; he explains that instead of a random basketweave formation of the collagen fibers found in normal tissue,[1] in fibrosis the collagen cross-links and forms a pronounced alignment in a single direction.[1] This collagen scar tissue alignment is usually of inferior functional quality to the normal collagen randomised alignment. For example, scars in the skin are less resistant to ultraviolet radiation, and sweat glands and hair follicles do not grow back within scar tissue. A myocardial infarction, commonly known as a heart attack, causes scar formation in the heart muscle, which leads to loss of muscular power and possibly heart failure. However, there are some tissues (e.g. bone) that can heal without any structural or functional deterioration.
Contents
Etymology
First attested in English in late 14th century, the word scar derives from Old French escharre, from Late Latin eschara,[2] which is the latinisation of the Greek ἐσχάρα (eskhara), meaning "hearth, fire-place", but in medicine "scab, eschar on a wound caused by burning or otherwise".[3][4]
Types
There are several different kinds of scarring, each caused by differing amounts of collagen over expression. One of the most common types is hypertrophic and keloid scarring,[5] both of which experience excessive stiff collagen bundled growth over extending the tissue, blocking off regeneration of tissues. Another form is atrophic scarring (sunken scarring), which also has an over expression of collagen blocking of regeneration, this scar type is sunken, the collagen bundles do not over extend the tissue. Stretch marks (striae) are regarded as scars to some.
Hypertrophic
Hypertrophic scars occur when the body overproduces collagen, which causes the scar to be raised above the surrounding skin. Hypertrophic scars take the form of a red raised lump on the skin.
Keloid
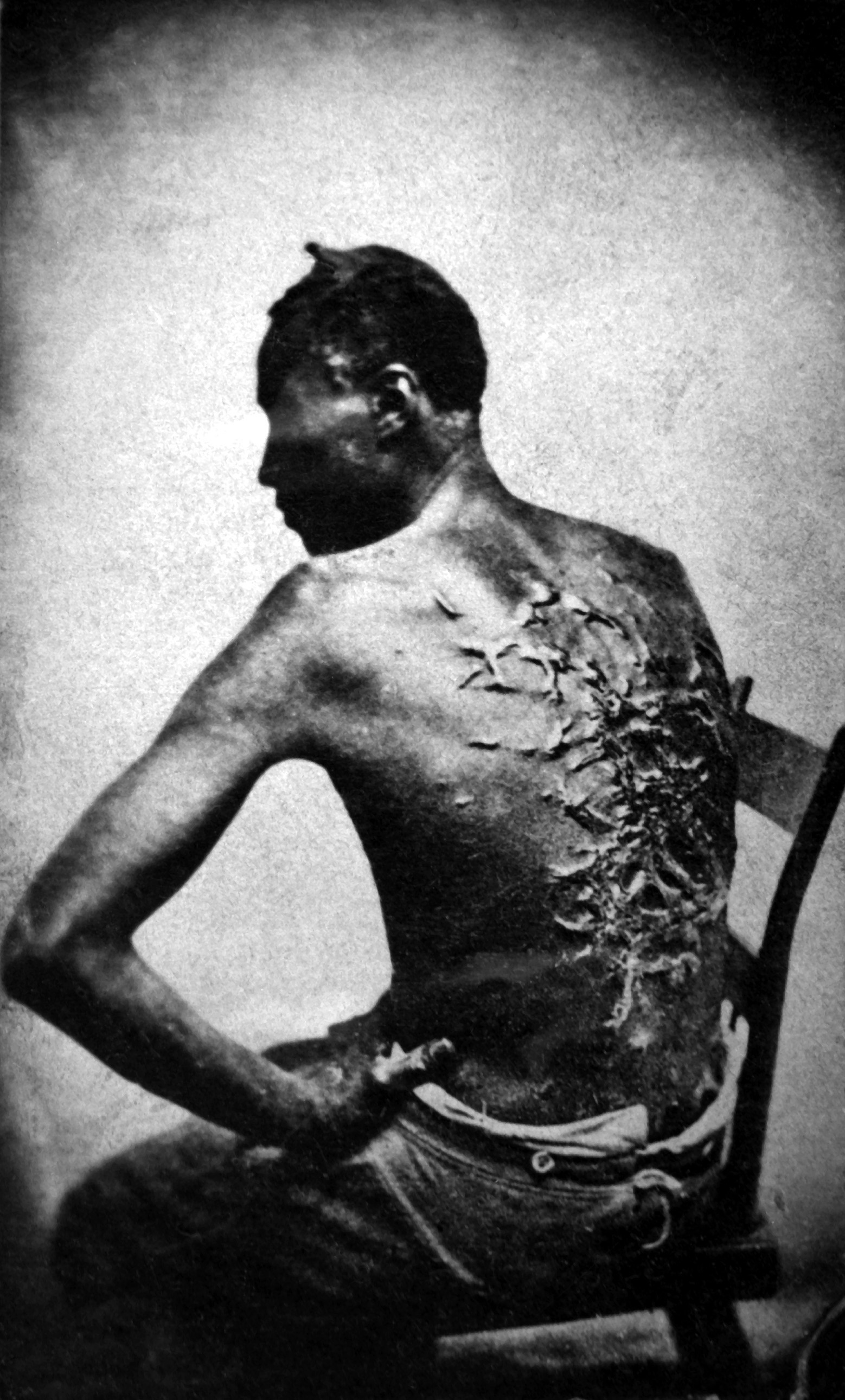
 Keloid scarring on the back of an enslaved African; those with darker skin pigmentations are more prone to the development of keloids.
Keloid scarring on the back of an enslaved African; those with darker skin pigmentations are more prone to the development of keloids.
Keloid scars are a more serious form of scarring, because they can carry on growing indefinitely into a large, tumorous (although benign) neoplasm.[5]
Hypertrophic scars are often distinguished from keloid scars by their lack of growth outside the original wound area, but this commonly taught distinction can lead to confusion.[5] All keloid scars are hypertrophic[5] but "only a small percentage of large scars" are keloid.[5] Phenotypic differences exist between keloid scars and hypertrophic scars.[5] Keloid scars can occur on anyone, but they are most common in dark-skinned people.[6] Keloid scars can be caused by surgery, an accident, by acne or, sometimes, from body piercings. In some people, keloid scars form spontaneously. Although they can be a cosmetic problem, keloid scars are only inert masses of collagen and therefore completely harmless and non-cancerous. However, they can be itchy or painful in some individuals. They tend to be most common on the shoulders and chest. Hypertrophic scars and its subset Keloid tend to be more common in wounds closed by secondary intention.[7]
Atrophic
An atrophic scar takes the form of a sunken recess in the skin, which has a pitted appearance. These are caused when underlying structures supporting the skin, such as fat or muscle, are lost. This type of scarring is often associated with acne,[8][9] chickenpox, other diseases (especially staphylococcus [or MRSA] infection), surgery or accidents.
Stretch marks
Stretch marks (technically called striae) are also a form of scarring. These are caused when the skin is stretched rapidly (for instance during pregnancy,[10] significant weight gain or adolescent growth spurts),[11] or when skin is put under tension during the healing process, (usually near joints). This type of scar usually improves in appearance after a few years.[10]
Elevated corticosteroid levels are implicated in striae development.[12]
Pathophysiology
 Hypertrophic scarring one year after Road rash on the left, and the original wound on the right.
Hypertrophic scarring one year after Road rash on the left, and the original wound on the right.If a wound re-epithelizes within two weeks there will be minimal collagen deposited and there will be no scar.[13] And generally if a wound takes longer than three to four weeks to re-epithelize a scar forms.[13]
The scar is a result of the body's repair mechanism after injury on many tissues.
Any injury does not become a scar until the wound has completely healed; this can take many months, or years in the worst pathological cases like keloids. To begin to patch the defect a clot is created; the clot is the beginning process that results in a provisional matrix. In the process the first layer is a provisional matrix and is not scar. Over time the wounded body tissue then over-expresses collagen inside the provisional matrix to create a collagen matrix. This collagen over expression continues and cross-links the fiber arrangement inside the collagen matrix, making the collagen dense. This densely-packed collagen, morphing into an inelastic whitish collagen[14] scar wall, blocks off cell communication and regeneration and as a result, the new tissue that is generated will have a different texture and quality than the surrounding non-wounded tissue. This prolonged collagen-producing process results in a fortuna scar.
The scarring is created by fibroblast proliferation,[14] a process that begins with a reaction to the clot.[15]
To mend the damage, fibroblasts slowly form the collagen scar. The fibroblast proliferation is circular[16] and cyclically, the fibroblast proliferation lays down thick whitish collagen[14] inside the provisional and collagen matrix, resulting in the packed abundant production of collagen on the fibers[14][15][17] giving scars their uneven texture. Over time, the fibroblasts continue to crawl around the matrix, adjusting more fibers and, in the process, the scarring settles and becomes stiff.[18] This fibroblast proliferation also contracts the tissue.[16][19] In non-wounded tissue, these fibers are not over expressed with thick collagen and do not contract.
The fibroblast involved in scarring and contraction is the myofibroblast.[20] The myofibroblast is a specialized contractile fibroblast[21] and these cells express a a-smooth muscle actin (a-SMA).[22]
The myofibroblast are absent in the first trimester in the embryonic stage which heals scar free;[23] in small incisional or excision wounds less than 2mm that also heal without scarring;[23] and in adult non wounded tissues were the fibroblast in itself is arrested ; however the myofibroblast is found massively in adult wound healing which heals with scar.[21]
The myofibroblasts make up a big proportion of the fibroblasts proliferating in the post embryonic wound at the onset of healing. In the rat model for instance the myofibroblast can be up to 70% of the fibroblasts.[20] and is responsible for fibrosis on tissue[24] Generally the myofibroblast disappear from the wound within 30 days;[25] but can stay around in pathological cases in hypertrophy like keloids.[21][25]
As well as the fibroblast proliferation[14] there is prolonged inflammation.
Redness that often follows an injury to the skin is not a scar, and is generally not permanent (see wound healing). The time it takes for this redness to dissipate may, however, range from a few days to, in some serious and rare cases, a few years.[citation needed]
Scars form differently based on the location of the injury on the body and the age of the person who was injured.[citation needed]
The worse the initial damage is, the worse the scar will generally be.[citation needed]
Skin Scars: Skin scars occur when the dermis (the deep, thick layer of skin) is damaged. Most skin scars are flat and leave a trace of the original injury that caused them.[citation needed]
Wounds that heal by secondary intention tend to scar worse than wounds closed by primary intention.[7]
Treatments
Early and effective treatment of acne scarring can prevent severe acne and the scarring that often follows[26] High melanin levels and either African or Asian ancestry may make adverse scarring more noticeable.[27] As of 2004[update] no prescription drugs for the treatment or prevention of scars were available.[28]
Chemical peels
Chemical peels are chemicals which destroy the epidermis in a controlled manner, leading to exfoliation and the alleviation of certain skin conditions including superficial acne scars.[29] Various chemicals can be used depending upon the depth of the peel and caution should be used, particularly for dark-skinned individuals and also including individuals susceptible to keloid formation or those with active infections.[30]
Filler injections
Filler injections of Collagen or ArteFill can be used to raise atrophic scars to the level of surrounding skin.[31] Risks vary based upon the filler used, and can include temporary improvement, further disfigurement, and allergic reaction.[32]
Dermabrasion
Dermabrasion involves the removal of the surface of the skin with specialist equipment and usually involves a local anaesthetic.
Laser Treatment
Non-ablative lasers such as the 585 nm Pulsed dye laser, 1064 nm and 1320 nm Nd:YAG, or the 1540 nm Er:Glass are used as the standard laser therapy for hypertrophic scars and keloids.[33] This therapy smooths the skin by heating up and redistributing collagen while avoiding damage to the epidermis via contact cooling. Multiple sessions are usually required for a significant reduction in redness and improvement in the texture and pliability of hypertrophic scars and keloids.
Ablative lasers such as the carbon dioxide laser or Er:YAG offer the best results for atrophic and acne scars.[34] Like dermabrasion, ablative lasers work by destroying the epidermis to a certain depth. Healing times for ablative therapy are much longer and the risk profile is greater compared to non-ablative therapy; however, non-ablative therapy offers only minor improvements in cosmetic appearance of atrophic and acne scars.[33]
Radiotherapy
Low-dose, superficial radiotherapy is sometimes used to prevent recurrence of severe keloid and hypertrophic scarring. It is thought to be effective despite a lack of clinical trials, but only used in extreme cases due to the perceived risk of long-term side effects.[35]
Semiocclusive Ointments & Pressure dressing
Silicone scar treatments are commonly used in preventing scar formation and improving existing scar appearance.[36] The effectiveness and safety of silicone sheeting for the treatment and prevention of scars is supported by an abundance of clinical studies.
There have been more controlled clinical trials performed on the treatment of scars using Silicone Gel Sheeting than most other methods.1
“the treated scars were improved significantly at 4, 8, and 12 weeks, compared with both their own treatment value and the control scars”2 “We conclude that this simple method of treating hypertrophic scar is efficacious, even in relatively chronic cases.”2 “Keloids and hypertrophic scars in children are effectively treated with silicone gel sheeting.”3 “Topical silicone gel sheeting is an effective method for the treatment of hypertrophic and keloid scars.” 4 For treatment of scars, “First-line therapy is silicone sheeting”5
Silicone gel sheeting is the only non-invasive option for which evidence-based recommendations have been made for both scar treatment and prevention.
“Overall, the success rate (somewhat improved to greatly improved) for the treatment of hypertrophic and keloid scars is high (95%).”6
1. Mustoe TA, Cooter RD, Gold MH, et al. International Clinical Recommendations on scar management. Plast Reconstr Surg 2002;110:560-71
2. Ahn ST, Monafo W, Mustoe TA Surgery 1989 Oct, 106 4:781-786
3. Laude TA ;Current Opinion Pediatrics, 1996 Aug 8 4: 381-385
4. Gold MH / Journal of Dermatology - Surgical Oncology Topical Silicone Gel Sheeting in the Treatment of Hypertrophic Scars and Keloids:A Dermatological Experience 1993; 19:912-916
5. Tønseth KA, Tindholdt TT, Solberg US, Busic V, Mesic H, Begic A Tidsskr Nor Laegeforen. 2003 Nov 6;123(21):3033-5
6. Dockery GL, Nilson RZ. Journal of Foot and Ankle Surgery 1994 Mar-Apr; 33 2:110 Treatment of Hypertrophic and Keloid Scars with Silastic Gel Sheeting
Semiocclusive silicone based ointments [37] are used to speed healing and reduce the appearance of scars and likely work in a similar manner as silicone scar sheets.Pressure dressings are commonly used in managing burn and hypertrophic scars, although supporting evidence is lacking.[38] These involve elastic materials or gauze which apply pressure to the area. For large scars and particularly large burns, pressure garments may be worn. It is believed that they work by applying constant pressure to surface blood vessels and eventually causing scars to flatten and become softer.[citation needed] Retrospective and ultrasonic studies since the 1960s have supported their use, but the only randomized clinical trial found no statistically significant difference in wound healing.[38] Care providers commonly report improvements, however, and pressure therapy has been effective in treating ear keloids.[38] The general acceptance of the treatment as effective may prevent it from being further studied in clinical trials.[38]
Steroids
A long term course of steroid injections under medical supervision, into the scar may help flatten and soften the appearance of keloid or hypertrophic scars.[39]
The steroid is injected into the scar itself; since very little is absorbed into the blood stream, side effects of this treatment are minor. However, it does cause thinning of the scar tissue so it does carry risks when injected into scars caused by operations into ruptured tendons. This treatment is repeated at 4-6 week intervals.
Topical steroids are ineffective.[40]
Surgery
 Scarring caused by acne (left), and photo 1 day after scar revision surgery. Area around sutures is still swollen from surgery
Scarring caused by acne (left), and photo 1 day after scar revision surgery. Area around sutures is still swollen from surgeryScar revision is a process of cutting the scar tissue out. After the excision, the new wound is usually closed up in order to heal by primary intention, instead of secondary intention. Deeper cuts need a multi-layered closure to heal optimally, otherwise depressed or dented scars can result.[41]
Surgical excision of hypertrophic or keloid scars is often associated to other methods such as pressotherapy or silicone gel sheeting. Lone excision of keloid scars however shows a high recurrence rate close to 45%. A clinical study is currently ongoing to assess the benefits of a treatment combining surgery and laser-assisted healing in hypertrophic or keloid scars.
Vitamins
Research shows the use of vitamin E and onion extract (sold under Mederma) as treatments for scars is ineffective.[38] Vitamin E causes contact dermatitis in up to 33% of users and in some cases it may worsen scar appearance.[40] Vitamin C and some of its esters also fade the dark pigment associated with some scars.[42]
Intentional scarring
The permanence of scarring has led to its intentional use as a form of body art within some cultures and subcultures (see scarification). These forms of ritual and non-ritual scarring practices can be found in many groups and cultures around the world.
Research
An intradermal injection of Transforming Growth Factor Beta 3 (TGFβ3) is being tested. The results of three trials already completed were published in the Lancet along with an editorial commentary.[43]
A study implicated the protein Ribosomal s6 kinase (RSK) in the formation of scar tissue and found that the introduction of a chemical to counteract RSK could halt the formation of Cirrhosis. This treatment also has the potential to reduce or even prevent altogether other types of scarring.[44]
Research has also implicated osteopontin in scarring.[45][46]
A research group in South Africa has a combination approach using a microporous tape in addition to Bulbine frutescens for hydration and Centella asiatica for collagen conversion.[47] A small study has shown an improved appearance of scars.[48]
See also
References
- ^ a b c Sherratt, Jonathan A. (2010). "Mathematical Modelling of Scar Tissue Formation". Department of Mathematics, Heriot-Watt University. http://www.ma.hw.ac.uk/~jas/researchinterests/scartissueformation.html. Retrieved 2010-08-20. "This is composed of the same main protein (collagen) as normal skin, but with differences in details of composition. Most crucially, the protein fibres in normal tissue have a random (basketweave) appearance, while those in scar tissue have pronounced alignment in a single direction."
- ^ eschara, Charlton T. Lewis, Charles Short, A Latin Dictionary, on Perseus
- ^ ἐσχάρα, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on perseus
- ^ Online Etymology Dictionary
- ^ a b c d e f Roseborough IE, Grevious MA, Lee RC (January 2004). "Prevention and treatment of excessive dermal scarring". J Natl Med Assoc 96 (1): 108–16. PMC 2594768. PMID 14746360. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2594768.
- ^ Martini, Frederic H. (2006). Fundamentals of Anatomy & Physiology, Seventh Edition, p. 171. Benjamin Cummings, San Francisco.
- ^ a b "Practical Plastic Surgery for Nonsurgeons - Secondary Wound Closure - Scarring". http://www.practicalplasticsurgery.org/docs/Practical_10.pdf. Retrieved 2011-04-02. "Wounds that are allowed to heal secondarily tend to have larger and more noticeable scars than the scars that results from primary closure. Secondary healing also has a greater tendency for hypertrophic scar/keloid formation. (page 86)"
- ^ Goodman, G. (2000). "Postacne scarring: A review of its pathophysiology and treatment". Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.] 26 (9): 857–871. PMID 10971560.
- ^ Fabbrocini, G.; Annunziata, M. C.; D'arco, V.; De Vita, V.; Lodi, G.; Mauriello, M. C.; Pastore, F.; Monfrecola, G. (2010). "Acne Scars: Pathogenesis, Classification and Treatment". Dermatology Research and Practice 2010: 1–13. doi:10.1155/2010/893080. PMC 2958495. PMID 20981308. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2958495.
- ^ a b Young, G.; Jewell, D. (1996). Young, Gavin. ed. Creams for preventing stretch marks in pregnancy. doi:10.1002/14651858.CD000066.
- ^ Elsaie, M. L.; Baumann, L. S.; Elsaaiee, L. T. (2009). "Striae Distensae (Stretch Marks) and Different Modalities of Therapy: An Update". Dermatologic Surgery 35 (4): 563–573. doi:10.1111/j.1524-4725.2009.01094.x. PMID 19400881.
- ^ Hengge, U.; Ruzicka, T.; Schwartz, R.; Cork, M. (2006). "Adverse effects of topical glucocorticosteroids". Journal of the American Academy of Dermatology 54 (1): 1–15. doi:10.1016/j.jaad.2005.01.010. PMID 16384751.
- ^ a b "POST BURN SCAR RELATIVE TO RE-EPITHELIALIZATION". Burnsurgery.org. 2011. http://www.burnsurgery.com/Modules/BurnWound%201/sect_IX.htm. Retrieved 2011-03-16. "Healing in 2 weeks – minimal to no scar; Healing in 3 weeks – minimal to no scar except in high risk scar formers;Healing in 4 weeks or more – hypertrophic in more than 50% of patients"
- ^ a b c d e "Facts about fibroblast: scar tissue formation,". Britannica.com. http://www.britannica.com/facts/5/264152/fibroblast-as-discussed-in-scar-biology. Retrieved 2010-04-19. "As part of the healing process, specialized cells called fibroblasts in adjacent areas of skin produce a fibrous connective tissue made up of collagen. The bundles formed by these whitish, rather inelastic fibres make up the bulk of the scar tissue..."
- ^ a b Parlange, Mary (2007-12-17). "New mechanical insights into wound healing and scar tissue formation". Ecole Polytechnique Fédérale de Lausanne. eurekalert.org. http://www.eurekalert.org/pub_releases/2007-12/epfd-nmi121707.php. Retrieved 2010-08-28. "The body launches a complex rescue operation. Specialized cells called fibroblasts lurking just beneath the surface of the skin jump into action, enter the provisional wound matrix (the clot) and start secreting collagen to close the wound as fast as possible."
- ^ a b Parlange, Mary (2007-12-17). "New mechanical insights into wound healing and scar tissue formation". Ecole Polytechnique Fédérale de Lausanne. eurekalert.org. http://www.eurekalert.org/pub_releases/2007-12/epfd-nmi121707.php. Retrieved 2010-08-28. "In the process, it liberates yet more growth factor that in turn stimulates other fibroblasts to become contractile…"
- ^ Inhibitor effects of local pretreated epidermis on wound scarring.. 2005. http://www.medwelljournals.com/fulltext/java/2008/1087-1089.pdf.[dead link]
- ^ Parlange, Mary (2007-12-17). "New mechanical insights into wound healing and scar tissue formation". Ecole Polytechnique Fédérale de Lausanne. eurekalert.org. http://www.eurekalert.org/pub_releases/2007-12/epfd-nmi121707.php. Retrieved 2010-08-28. "The fibroblasts "crawl" around the matrix, pulling and reorganizing the fibers. The matrix grows stiffer,"
- ^ Parlange, Mary (2007-12-17). "New mechanical insights into wound healing and scar tissue formation". Ecole Polytechnique Fédérale de Lausanne. eurekalert.org. http://www.eurekalert.org/pub_releases/2007-12/epfd-nmi121707.php. Retrieved 2010-08-28. "The matrix grows stiffer and, at a certain point, the fibroblasts stop migrating and, like Popeye, change into powerful contractile cells, anchoring themselves to the matrix and pulling the edges of the wound together."
- ^ a b "Method of preventing or reducing scarring of human skin". freepatentsonline.com. http://www.freepatentsonline.com/y2005/0054608.html. Retrieved 2010-03-26. "myofibroblasts become differentiated from other cells in the wound within a few days after the onset of healing, and in the rat model can reach a peak where about 70% of the fibroblastic cells present are of the myofibroblast phenotype."
- ^ a b c "Method of preventing or reducing scarring of human skin". freepatentsonline.com. http://www.freepatentsonline.com/y2005/0054608.html. Retrieved 2010-03-26. "These cells, which differentiate from the unwounded tissue cell type (fibroblasts), are responsible for laying down scar tissue. Indeed myofibroblasts remain present in hypertrophic scars up to four years after the original wounding event. An in vitro assay was accordingly developed to identify actives which prevent or reduce myofibroblast formation and thus identify actives which are effective in reducing and/or preventing scar tissue formation."
- ^ "Regenerative Healing in Fetal Skin: A Review of the Literature". o-wm.com. 2008-03-09. http://www.o-wm.com/content/regenerative-healing-fetal-skin-a-review-literature?page=0,11. Retrieved 2011-03-26. "Aside from normal fibroblasts, myofibroblasts, specialized contractile fibroblasts, also can contribute to wound repair. These cells express a-smooth muscle actin (a-SMA) and are characterized using transmission electron microscopy by a well-developed rough endoplasmic reticulum, nuclei with irregular borders, secretory vesicles denoting active collagen synthesis, and organized microfilament bundles."
- ^ a b "Regenerative Healing in Fetal Skin: A Review of the Literature". o-wm.com. 2008-03-09. http://www.o-wm.com/content/regenerative-healing-fetal-skin-a-review-literature?page=0,11. Retrieved 2011-03-26. "Studies in sheep have indicated that myofibroblasts are absent in early scarless fetal wounds but are present during healing at later stages when prominent scarring occurs. In addition, incisional or small excisional wounds (2 mm) heal without a scar and do not contain myofibroblasts. In contrast, larger excisional wounds that heal with a scar contain strong a-SMA staining, with the number of myofibroblasts correlating with the size of the wound and amount of scarring."
- ^ Leask, Andrew (2008-09-23). "When Healing Turns To Scarring: Research Reveals Why It Happens And How To Stop It". the Canadian Foundation for Innovation, CIHR, the Arthritis Research Campaign, the Reynaud's and Scleroderma Foundation, and the Scleroderma Society.: sciencedaily.com. http://www.sciencedaily.com/releases/2008/09/080918192824.htm. Retrieved 2011-02-26. "During tissue repair, specialized cells called myofibroblasts migrate to the wound where they generate the adhesive and tensile forces required for wound closure. Normally, these myofibroblasts then disappear from the wound. But if they persist and continue to make connective tissue, it can become too thick, preventing the organ from functioning properly."
- ^ a b "Method of preventing or reducing scarring of human skin". freepatentsonline.com. http://www.freepatentsonline.com/y2005/0054608.html. Retrieved 2010-03-26. "the number of myofibroblasts present in the forming scar tissue begins to reduce via apoptosis, until by about 30 days no myofibroblasts are obvious within the scar."
- ^ "What is a Scar". American Academy of Dermatology. 2011. http://www.aad.org/public/publications/pamphlets/cosmetic_scar.html. Retrieved 2011-08-25. "Early and effective acne treatment can prevent severe acne and the scarring that often follows"
- ^ Kelly, A. P. (2009). "Update on the Management of Keloids". Seminars in Cutaneous Medicine and Surgery 28 (2): 71–76. doi:10.1016/j.sder.2009.04.002. PMID 19608056.
- ^ Ferguson MW, O'Kane S (May 2004). "Scar-free healing: from embryonic mechanisms to adult therapeutic intervention". Philos. Trans. R. Soc. Lond., B, Biol. Sci. 359 (1445): 839–50. doi:10.1098/rstb.2004.1475. PMC 1693363. PMID 15293811. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1693363.
- ^ Khunger, N.; Iadvl Task, F. (2008). "Standard guidelines of care for acne surgery". Indian journal of dermatology, venereology and leprology 74 Suppl: S28–S36. PMID 18688101.
- ^ Khunger N. Standard guidelines of care for chemical peels. Indian J Dermatol Venereol Leprol [serial online] 2008 [cited 2010 May 22];74(Suppl):S5-S12. Free full-text.
- ^ Cooper, J.; Lee, B. (2009). "Treatment of Facial Scarring: Lasers, Filler, and Nonoperative Techniques". Facial Plastic Surgery 25 (5): 311–315. doi:10.1055/s-0029-1243079. PMID 20024872.
- ^ Lemperle, G.; Rullan, P. P.; Gauthier-Hazan, N. (2006). "Avoiding and Treating Dermal Filler Complications". Plastic and Reconstructive Surgery 118 (3 Suppl): 92S–107S. doi:10.1097/01.prs.0000234672.69287.77. PMID 16936549.
- ^ a b Elsaie, ML; Choudhary, S (2010). "Lasers for scars: a review and evidence-based appraisal". Journal of drugs in dermatology : JDD 9 (11): 1355–62. PMID 21061757.
- ^ Khatri, Khalil A.; Mahoney, Danielle L.; McCartney, Melissa J. (2011). "Laser scar revision: A review". Journal of Cosmetic and Laser Therapy 13 (2): 54–62. doi:10.3109/14764172.2011.564625. PMID 21401378.
- ^ Ogawa, Rei; Yoshitatsu, Sumiko; Yoshida, Ken; Miyashita, Tsuguhiro (2009). "Is Radiation Therapy for Keloids Acceptable? The Risk of Radiation-Induced Carcinogenesis". Plastic and Reconstructive Surgery 124 (4): 1196–1201. doi:10.1097/PRS.0b013e3181b5a3ae. PMID 19935303.
- ^ Stavrou, Demetris; Weissman, Oren; Winkler, Eyal; Yankelson, Lior; Millet, Eran; Mushin, Oren Paul; Liran, Alon; Haik, Joseph (2010). "Silicone-Based Scar Therapy: A Review of the Literature". Aesthetic Plastic Surgery 34 (5): 646–651. doi:10.1007/s00266-010-9496-8. PMID 20354695.
- ^ Ziegler UE (2004). "[International clinical recommendations on scar management]" (in German). Zentralbl Chir 129 (4): 296–306. doi:10.1055/s-2004-822830. PMID 15354252.
- ^ a b c d e Shih R, Waltzman J, Evans GR (March 2007). "Review of over-the-counter topical scar treatment products". Plast. Reconstr. Surg. 119 (3): 1091–5. doi:10.1097/01.prs.0000255814.75012.35. PMID 17312518.
- ^ Roques, C.; Teot, L. (2008). "The Use of Corticosteroids to Treat Keloids: A Review". The International Journal of Lower Extremity Wounds 7 (3): 137–145. doi:10.1177/1534734608320786. PMID 18611924.
- ^ a b Jenkins M, Alexander JW, MacMillan BG, Waymack JP, Kopcha R. Failure of topical steroids and vitamin E to reduce postoperative scar formation following reconstructive surgery. J Burn Care Rehabil. 1986 Jul–Aug;7(4):309–312.
- ^ "Scar revisions". http://www.haplasticsurgery.com/scar-revision-surgery-dallas-texas.html. Retrieved 2010-10-16. "Deep cuts need multi-layered closure to heal optimally; otherwise, depressed or dented scars can result"
- ^ Farris PK. Topical vitamin C: a useful agent for treating photoaging and other dermatologic conditions. Dermatol Surg 2005;31:814-818.
- ^ Renovo. [1]. Lancet trials in: 11 April 2009 (vol. 373, pages 1264-1274). Lancet commentary by Edward Tredget in: vol 373, pages 1226-1228
- ^ "Liver damage 'could be reversed'". BBC News. 27 December 2007. http://news.bbc.co.uk/2/hi/health/7152415.stm. Retrieved 2008-01-01.
- ^ 'Molecular mechanisms linking wound inflammation and fibrosis: knockdown of osteopontin leads to rapid repair and reduced scarring'
- ^ "Gel 'to speed up wound healing'". BBC News. 2008-01-22. http://news.bbc.co.uk/2/hi/health/7199897.stm. Retrieved 2010-05-23.
- ^ Widgerow AD. (2010). Scar management–marrying the practical with the science. Wound Healing South Africa.
- ^ Widgerow AD, Chait LA, Stals PJ, Stals R, Candy G (July 2009). "Multimodality scar management program". Aesthetic Plast Surg 33 (4): 533–43. doi:10.1007/s00266-008-9276-x. PMID 19048338.
External links
- WebMD.com article
- American Academy of Dermatology: "What is a scar?"
- Ohio State University Medical Center article
- International Scar Meeting in Tokyo 2010 International Scar Meeting
Wound healing Blood vessels Other Cutaneous keratosis, ulcer, atrophy, and necrobiosis (L82–L94, 700–701.5) Epidermal thickening keratoderma: Keratoderma climactericum • Paraneoplastic keratoderma (Acrokeratosis paraneoplastica of Bazex ) • Aquagenic keratoderma · Drug-induced keratoderma · Paraneoplastic keratoderma • psoriasis (Keratoderma blennorrhagica)
keratosis: Seborrheic keratosis (Clonal seborrheic keratosis · Common seborrheic keratosis · Irritated seborrheic keratosis · Seborrheic keratosis with squamous atypia · Reticulated seborrheic keratosis · Dermatosis papulosa nigra) • Keratosis punctata of the palmar creases
other hyperkeratosis: Acanthosis nigricans (Confluent and reticulated papillomatosis) · Callus • Ichthyosis acquisita · Arsenical keratosis · Chronic scar keratosis · Hyperkeratosis lenticularis perstans · Hydrocarbon keratosis · Hyperkeratosis of the nipple and areola · Inverted follicular keratosis · Lichenoid keratosis · Multiple minute digitate hyperkeratosis · PUVA keratosis · Reactional keratosis · Stucco keratosis · Thermal keratosis · Viral keratosis · Warty dyskeratoma · Waxy keratosis of childhood
other hypertrophy: Keloid · Hypertrophic scar • Cutis verticis gyrata ·Necrobiosis/granuloma Granuloma annulare (Perforating, Generalized, Subcutaneous, Granuloma annulare in HIV disease, Localized granuloma annulare, Patch-type granuloma annulare) · Necrobiosis lipoidica · Annular elastolytic giant cell granuloma · Granuloma multiforme · Necrobiotic xanthogranuloma · Palisaded neutrophilic and granulomatous dermatitis · Rheumatoid nodulosis · Interstitial granulomatous dermatitis/Interstitial granulomatous drug reactionForeign body granulomaBeryllium granuloma • Mercury granuloma • Silica granuloma • Silicone granuloma • Zirconium granuloma • Soot tattoo • Tattoo • Carbon stainOther/ungroupedeosinophilic dermatosis (Granuloma faciale)Dermis/
localized CTDCutaneous lupus
erythematosusLocalized scleroderma (Localized morphea, Morphea–lichen sclerosus et atrophicus overlap, Generalized morphea, Atrophoderma of Pasini and Pierini, Pansclerotic morphea, Morphea profunda, Linear scleroderma)Atrophic/
atrophodermaLichen sclerosus · Anetoderma (Schweninger–Buzzi anetoderma, Jadassohn–Pellizzari anetoderma) · Atrophoderma of Pasini and Pierini · Acrodermatitis chronica atrophicans · Semicircular lipoatrophy · Follicular atrophoderma · Linear atrophoderma of MoulinKyrle disease · Reactive perforating collagenosis · Elastosis perforans serpiginosa · Perforating folliculitis · Acquired perforating dermatosisOtherCategories:- Diseases involving the fasciae
- Greek loanwords



Wikimedia Foundation. 2010.