- Babesia
-
"Texas fever" redirects here. For other uses, see Texas fever (disambiguation).
Babesia[1][2] 
Scientific classification Domain: Eukaryota Kingdom: Chromalveolata Superphylum: Alveolata Phylum: Apicomplexa Class: Aconoidasida Order: Piroplasmida Family: Babesiidae Genus: Babesia Species Babesia bigemina
Babesia bovis
Babesia canis
Babesia cati
Babesia divergens
Babesia duncani
Babesia felis
Babesia gibsoni
Babesia herpailuri
Babesia jakimovi
Babesia major
Babesia microti
Babesia ovate
Babesia pantheraeBabesia is a protozoan parasite of the blood that causes a hemolytic disease known as Babesiosis. There are over 100 species of Babesia identified; however only a handful have been documented as pathogenic in humans.[3]
In the United States, Babesia microti is the most common strain associated with humans with other species infecting cattle, livestock and occasionally domestic animals.[4][5] People who contract Babesiosis suffer from malaria-like symptoms. As a result malaria is a common misdiagnosis for the disease.
Contents
Classification
Babesia is a protozoan parasite of which Babesia microti and Babesia divergens are the two species to most frequently infect humans. Infections from other species of Babesia have been documented in humans but are not habitually seen. Babesiosis is also known as Piroplasmosis.[4] Due to historical misclassifications, this protozoan was labeled with many names that are no longer used. Common names of the disease include Texas Cattle Fever, Redwater Fever, Tick Fever, and Nantucket Fever.[5]
History
For centuries, babesiosis was known to be a serious illness for wild and domesticated animals, especially cattle. Victor Babeş, a Romanian scientist who first documented the disease in Romania in 1888, described symptoms of a severe hemolytic illness seen uniquely in cattle and sheep.[5] Although he identified the causative agent in 1888, he incorrectly believed it to be due to a bacterium that he named Haematococcus bovis.
In 1893 Americans Theobald Smith and Fred Kilborne identified the parasite as the cause of Texas Cattle Fever, the same disease described by Babeş. Smith and Kilborne also identified the tick as the agent of transmission, a discovery that first introduced the concept of arthropods functioning as disease vectors.[6] Long believed to be a disease that only affected non-human mammals, it wasn’t until 1957 that the first case of babesiosis was seen in humans.[4] The first case was observed in a splenectomized patient as were all people diagnosed up until 1969. The first case of babesiosis seen in a non-splenectomized patient proved that the protozoan parasite was pathogenic to all people.[7]
Clinical presentation
The severity of B. microti infections varies. For 25% of cases in adults and half of cases in children, the disease is asymptomatic or mild with flu-like symptoms. In cases of symptomatic infection, symptoms are characterized by irregular fevers, chills, headaches, general lethargy, pain and malaise.[4] In severe cases, hemolytic anemia, jaundice, shortness of breath, and hemoglobinuria are documented due to the lytic effects of parasitic multiplication.[5][8] Immunocompetent individuals with healthy spleens often recover without treatment.[4] Splenectomized patients are more susceptible to contracting the disease and the course of infection often ends fatally within 5 to 8 days of symptom onset.[9] Parasitemia levels can reach up to 85% in patients without spleens compared to 1-10% in individuals with spleens and effective immune systems. Splenectomized patients suffer from severe hemolytic anemia with occasional incidences of hepatomegaly and splenomegaly documented.[8]
Complications that arise from B. microti infections include acute respiratory failure, congestive heart failure, and renal failure. Infections can be fatal in 5-10% of hospitalized patients with increased risk of death in the immunosuppressed, the elderly, and those co-infected with Lyme disease.[8] B. divergens infections have a much higher fatality rate (42%) and present with the most severe symptoms. Infected individuals suffer from hemoglobinuria followed by jaundice, a persistently high fever, chills and sweats. If left untreated, B. divergens infections can develop into shock-like symptoms with pulmonary edema and renal failure.[8]
Signs of infection usually arise 1 to 8 weeks after a bite from an infectious tick.[9] Infections from B. divergens have a shorter latent period usually ranging from 1–3 weeks.[8]
Transmission
Babesia is spread through the saliva of a tick when it bites. At its nymphal stage, a tick will bite into the skin for a blood meal. The tick, if not removed, will stay attached for 3 to 6 days with longer periods of feeding associated with a higher probability of acquiring the parasite. The parasite can survive in the tick as it molts through its various developmental stages resulting in all stages being potentially infectious. Some species of Babesia can be transmitted from a female tick to its offspring before migrating to salivary glands for feeding.[4] B. microti, the most common variety of Babesia in humans however, has not been shown to transmit transovarially.[3]
In the Americas, Ixodes scapularis is the most common vector. This hard tick, commonly known as a deer tick, is also the vector for other tick-associated illnesses such as Lyme disease. Many species of Babesia only infect non-human mammalian hosts, most commonly cattle, horses, and sheep. B. microti and B. divergens are the two main pathogenic species in humans. Their reservoirs are theorized to be the white-footed mouse (Peromyscus leucopus Rafinesque), microtus voles (Microtus spp.), and the white-tailed deer (Odocoileus virginianus).[10] These woodland species are hypothesized reservoirs because although they are known to harbor the disease, complete reservoir competence has not yet been shown.[11]
Most cases of transmission between humans are attributed to a tick vector. However, as of 2003 the Centers for Disease Control and Prevention (CDC) acknowledged more than 40 cases of Babesiosis contracted from packed red blood cell (PRBC) transfusions and 2 infections documented from organ transplantation. PRBC transfusions that cause infections were identified through testing of the blood donor for B. microti antibodies.[12] The occurrence of PRBC transfusions as a mechanism of Babesia transmission puts pressure on governmental organizations, such as the CDC, to heighten standard measures for screening blood donations.
Morphology
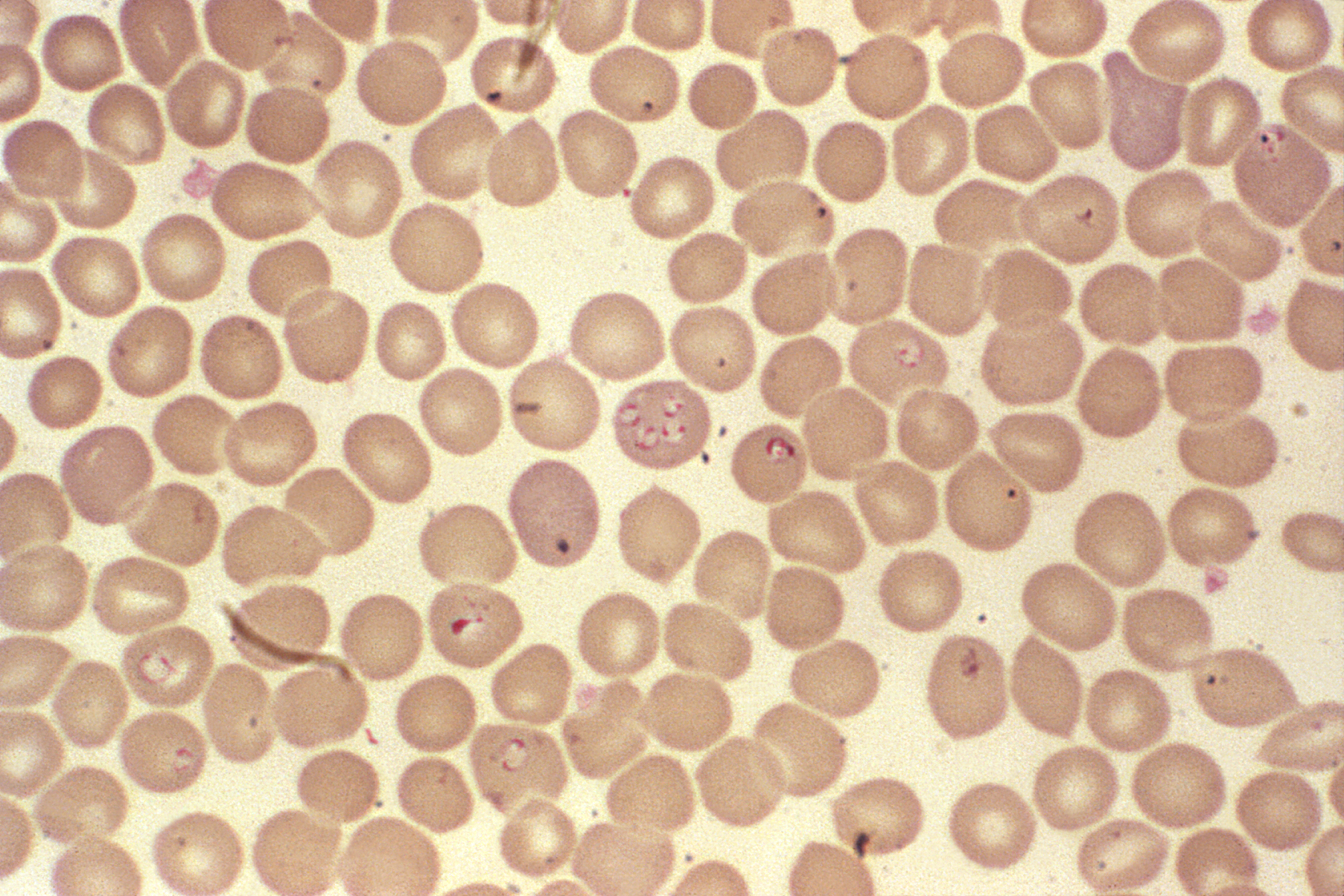
Babesia enters erythrocytes at the sporozoite stage. Within the red blood cell, the protozoa become cyclical and develop into a trophozoite ring. The trophozoites morph into merozoites, which have a tetrad structure coined a Maltese-cross form.[13] The tetrad morphology, which can be seen with Giemsa staining of a thin blood smear, is unique to Babesia and serves as a distinguishing feature from Plasmodium falciparum, a protozoan of similar morphology that causes Malaria. Trophozoite and merozoite growth ruptures the host erythrocyte leading to the release of vermicules, the infectious parasitic bodies, which rapidly spread the protozoa throughout the blood.[4]
Life cycle
The life cycle of Babesia microti, which is typical of parasites in the Babesia genus, requires a biological stage in a rodent or deer host and is transmitted by ticks of the genus Ixodidae between these hosts. To begin, the ticks introduce the sporozoites into the rodent when taking a blood meal. Sporozoites enter erythrocytes in the blood and begin the cyclical development between trophozoites and merozoites. Rather than producing more trophozoites, some merozoites produce gametocytes. The definitive tick host, of the Ixodidae genus, takes up the gametocytes when attached for a blood meal. The gametes are fertilized in the gut of the tick and develop into sporozoites in the salivary glands. The sporozoites are introduced into a human upon inoculation at the bite of an infected tick. Even as an incidental host, the phase changes that occur in the parasite are the same within humans as in the biological hosts. Babesia can be diagnosed at the trophozoite stage and can be transmitted from human to human either through the tick vector or through blood transfusions.[3]
 Life Cycle of Babesia
Life Cycle of Babesia
Diagnosis and treatment
Diagnostic tests
As a protozoan parasite, the most effective way to identify Babesia infection is through blood sample testing. It is important to pay specific attention to particular morphologies of Babesia in blood smears because its substantial similarity to the malarial parasite Plasmodium falciparum results in many patients suffering from Babesiosis being misdiagnosed. The few distinguishing factors for Babesia include protozoa with varying shapes and sizes, the potential to contain vacuoles, and the lack of pigment production. Trophozoites within an erythrocyte that appear in a tetrad formation are also indicative of Babesia. A trained eye is necessary to distinguish the two species.
Even with much study of Babesiosis and Malaria, misdiagnosis with blood smear can be frequent and problematic. To supplement a blood smear, diagnoses should be made with an indirect fluorescent antibody (IFA) test. IFA testing has a much higher specificity than stained blood smears with antibody detection in 88-96 % of infected patients.[3] Diagnostic measures through antibody testing are also particularly useful for identifying serum prevalence in asymptomatic individuals. Due to the transmissibility of Babesia through blood transfusions, IFA testing would be an effective means of screening for the disease in blood donations.
Historically, Babesiosis diagnosis was carried out with xenodiagnosis in hamsters for B. microti and in gerbils for B.divergens.[4] While successful at identifying the disease, this diagnostic technique has been abandoned for faster diagnostic measures.
Treatment
There are several ways to manage and treat Babesiosis in animals. In many cases, patients spontaneously recover having only experienced mild symptoms undiagnosed as the disease. This occurrence is almost always seen in B. microti infections, which are generally more common in the United States. For B. divergens and more severe B. microti infections, the standard treatment historically for symptomatic individuals was oral or intravenous Clindamycin with oral quinine.[3] With the results of research completed in 2000 however, treatment regimens have been increasingly leaning towards oral Atovaquone with oral azithromycin. The latter medications are preferred as they are equally effective and exhibit fewer associated adverse reactions.[14] In severe cases, blood exchange transfusions have been performed to lower the parasitic load in the individual.[4] Other rudimentary treatment measures include addressing and correcting abnormal clinical signals.[5]
Epidemiology
Of the species to infect humans, B. microti is most common in the Americas whereas B. divergens is the predominant strain found in Europe. Endemic areas are regions of tick habitat, including the forest regions of the Northeastern United States and temperate regions of Europe.[9] Ixodidae, the tick vector of B. microti, also transmits the better-known Lyme disease. For reasons that remain unclear, in areas endemic to both Lyme disease and Babesiosis, Lyme disease transmission prevails and is more predominant in the region.[4] Prevalence of Babesiosis is regions endemic to Malaria remains unknown due to the likelihood of misdiagnosis as Malaria.[8] As the disease results in a high number of asympomatic individuals, many populations can possess high seroprevalence without much documentation of illness. For example, in Rhode Island and Nantucket, seroprevalence has been measured to be 20-25%.[4] Prevalence of Babesiosis is most documented during the months of May to September where there is high tick activity in endemic regions.[9]
Prevention
The most effective public health measure for Babesia is avoidance of tick exposure. This can be performed through personal prevention strategies such as avoiding tick infested areas (especially during high tick season between May and September), remaining covered with light clothing, searching for ticks after being outdoors and removing discovered ticks from the skin.[8] Other preventative measures include applying Diethyltoluamide (DEET), a common bug repellent that is effective against ticks, amongst other insects. (For people who react adversely to DEET, alternative insect repellents should be used.) On a state level, if health departments are particularly motivated, tick elimination is a possibility. In 1906, efforts were made to eradicate the tick vector of the bovine disease form of Babesiosis in the United States. This eradication was recorded as being successfully completed four decades later.[5] Complete eradication efforts would be a long-term project, which would significantly reduce the prevalence of both Babesiosis and Lyme disease. However, as public health departments are often short on funding, preventative measures seem to be more recommended over vector control. Due to the relatively low prevalence of the disease and the presence of several reservoirs, Babesiosis is currently not a candidate for vaccine-based prevention.
Useful links
- Lyme and Tick-Borne Diseases Research Center: Babesiosis
- Connecticut Department of Public Health: Babesiosis Fact Sheet
- New York State Department of Health: Babesiosis
- Centers for Disease Control and Prevention: Babesia
- DPDx: Laboratory Identification of Parasites of Public Health Concern: Babesiosis
See also
References
- ^ Khayat, Abeer; Rathore, Mobeen (2008). The Neurological Manifestations of Pediatric Infectious Diseases and Immunodeficiency Syndromes. Humana Press. pp. 343–346 (Chap 36).
- ^ National Center for Biotechnology Information: Taxonomy Browser
- ^ a b c d e DPDx: Laboratory Identification of Parasites of Public Health Concern. Babesiosis. CDC. Retrieved on 2009-03-05.
- ^ a b c d e f g h i j k Despommier, Dickson D.; et al. (1995). Parasitic Diseases. Ed 3. New York City, New York: Spinger-Verlag Inc. pp. 224–226.
- ^ a b c d e f Ristic, M. et al. Ed. (1984). Malaria and Babesiosis: New Perspectives in Clinical Microbiology. Dordrecht, The Netherlands: Martinus Nijhoff Publishers. pp. 100–170.
- ^ Schultz, Myron (December 2008). "Photo Quiz: Theobald Smith". Emerg Infect Dis 14 (12): 1939. doi:10.3201/eid1412.081188. ISSN 1080-6059. http://www.cdc.gov/eid/content/14/12/1939.htm.
- ^ Beaver; Paul Chester, et al.. Clinical Parasitology (9th ed.). Philadelphia, Pennsylvania: Lea and Febiger. pp. 205–208.
- ^ a b c d e f g Gelfand, Jeffrey A.; Vannier, Edouard. Harrison's Principles of Internal Medicine, 17e - Babesiosis. McGraw-Hill’s Access Medicine. pp. Chap 204. http://www.accessmedicine.com/content.aspx?aID=2892931.
- ^ a b c d Babesiosis National Institute of Allergy and Infectious Diseases, National Institutes of Health.
- ^ Karbowiak G (2004). "Zoonotic reservoir of Babesia microti in Poland". Pol. J. Microbiol. 53 Suppl: 61–5. PMID 15787199.
- ^ Telford SR, Spielman A (January 1993). "Reservoir competence of white-footed mice for Babesia microti". J. Med. Entomol. 30 (1): 223–7. PMID 8433329.
- ^ Lux JZ, Weiss D, Linden JV, et al. (January 2003). "Transfusion-associated babesiosis after heart transplant". Emerging Infect. Dis. 9 (1): 116–9. PMC 2873739. PMID 12533293. http://www.cdc.gov/ncidod/EID/vol9no1/02-0149.htm.
- ^ Herwaldt BL, Cacciò S, Gherlinzoni F, et al. (August 2003). "Molecular characterization of a non-Babesia divergens organism causing zoonotic babesiosis in Europe". Emerging Infect. Dis. 9 (8): 942–8. PMID 12967491. http://www.cdc.gov/ncidod/EID/vol9no8/02-0748.htm. "Figure 2. Panel of computer-generated electronic images of photomicrographs of Babesia-infected erythrocytes on a Giemsa-stained smear of peripheral blood..."
- ^ Krause PJ, Lepore T, Sikand VK, et al. (November 2000). "Atovaquone and azithromycin for the treatment of babesiosis". N. Engl. J. Med. 343 (20): 1454–8. doi:10.1056/NEJM200011163432004. PMID 11078770. http://content.nejm.org/cgi/content/full/343/20/1454.
Ciliophora Spirotrichea (Stylonychia) · Litostomatea (Didinium, Balantidium) · Phyllopharyngea (Tokophrya) · Nassophorea (Nassula) · Colpodea (Colpoda) · Oligohymenophorea (Tetrahymena, Ichthyophthirius, Vorticella, Paramecium) · Plagiopylea (Plagiopyla) · Prostomatea (Coleps)OtherMyzozoa Plasmodiidae/Haemosporida (Plasmodium, Haemoproteus, Leucocytozoon)
Piroplasmida (Babesia, Theileria)Adele-Eimeri-Cryptosporidiidae (Cryptosporidium)
Eimeriidae (Isospora, Cyclospora, Eimeria)
Sarcocystidae (Toxoplasma, Sarcocystis, Besnoitia, Neospora)Agamo-Rhytidocystidae (Rhytidocystis)GregariniaGregarinasina (Gregarina)ColpodellidaeChromeridaWith a theca: Peridiniales (Pfiesteria, Peridinium) · Gonyaulacales (Ceratium, Gonyaulax) · Prorocentrales (Prorocentrum) · Dinophysiales (Dinophysis, Histioneis, Ornithocercus, Oxyphysis)
Without theca: Gymnodiniales (Gymnodinium, Karenia, Karlodinium, Amphidinium) · Suessiales (Polarella, Symbiodinium)
Noctilucales (Noctiluca)Syndiniales: Amoebophryaceae (Amoebophyra) · Duboscquellaceae (Duboscquella) · Syndiniaceae (Hematodinium, Syndinium)OtherRelatedCategories:- Parasites
- Tick-borne diseases
- Apicomplexa
- Parasitic protists

Wikimedia Foundation. 2010.