- Cryopreservation
-
 Cryopreservation of plant shoots. Open tank of liquid nitrogen behind.
Cryopreservation of plant shoots. Open tank of liquid nitrogen behind.
 A tank of liquid nitrogen, used to supply a cryogenic freezer (for storing laboratory samples at a temperature of about −150 degrees Celsius).
A tank of liquid nitrogen, used to supply a cryogenic freezer (for storing laboratory samples at a temperature of about −150 degrees Celsius).Cryopreservation is a process where cells or whole tissues are preserved by cooling to low sub-zero temperatures, such as (typically) 77 K or −196 °C (the boiling point of liquid nitrogen). At these low temperatures, any biological activity, including the biochemical reactions that would lead to cell death, is effectively stopped. However, when cryoprotectant solutions are not used, the cells being preserved are often damaged due to freezing during the approach to low temperatures or warming to room temperature.
Contents
Temperature
Cryogenic storage at very low temperatures is presumed to provide an indefinite, if not near infinite, longevity to cells although the actual “shelf life” is rather difficult to prove. In experiments with dried seeds, researchers found that there was noticeable variability in deterioration when samples were kept at different ‘frozen’ temperatures–even ultra cold ones. Temperatures below the glass transition point (Tg) of polyol's water solutions (around minus 136°C) appear to be accepted as the range where biological activity very substantially slows down, and minus 196°C (liquid phase of liquid nitrogen) is the preferred temperature for the storage of important specimens. While fridges, deep freezers and extra cold deep freezers, all similar to domestic ones, are used for many items, generally the ultra cold of liquid nitrogen at -196°C is required for successful preservation of the more complex biological structures to virtually stop all biological activity.
Risks
Phenomena which can cause damage to cells during cryopreservation mainly occur during the freezing stage, and include: solution effects, extracellular ice formation, dehydration and intracellular ice formation. Many of these effects can be reduced by cryoprotectants.
When having reached the frozen stage, the preserved material is relatively safe from further damage. However, estimates based on the accumulation of radiation-induced DNA damage during cryogenic storage have suggested a maximum storage period of 1000 years.
Solution effects
As ice crystals grow in freezing water, solutes are excluded, causing them to become concentrated in the remaining liquid water. High concentrations of some solutes can be very damaging.
Extracellular ice formation
When tissues are cooled slowly, water migrates out of cells and ice forms in the extracellular space. Too much extracellular ice can cause mechanical damage to the cell membrane due to crushing.
Dehydration
The migration of water causing extracellular ice formation can also cause cellular dehydration. The associated stresses on the cell can cause damage directly.
Intracellular ice formation
While some organisms and tissues can tolerate some extracellular ice, any appreciable intracellular ice is almost always fatal to cells.
Main methods to prevent risks
The main techniques to prevent cryopreservation damages are a well established combination of controlled rate and slow freezing on one hand, and a newer flash-freezing process known as vitrification on the other.
Slow programmable freezing
Controlled-rate and slow freezing, also called slow programmable freezing (SPF),[1] is a set of well established techniques pioneered in the early 1970s which enabled the first human embryo frozen birth Zoe Leyland in 1984. Since then machines that freeze biological samples using programmable steps, or controlled rates, have been used all over the world for human, animal and cell biology – 'freezing down' a sample to better preserve it for eventual thawing, before it is deep frozen, or cryopreserved, in liquid nitrogen. Such machines are used for freezing oocyte, skin, blood products, embryo, sperm, stem cells and general tissue preservation in hospitals, veterinary practices and research labs around the world. As an example, estimates put the number of live births from frozen embryos 'slow frozen' at some 300,000 to 400,000 or 20% of the estimated 3 million IVF births.[2]
Lethal intracellular freezing can be avoided if cooling is slow enough to permit sufficient water to leave the cell during progressive freezing of the extracellular fluid. That rate differs between cells of differing size and water permeability: a typical cooling rate around 1°C/minute is appropriate for many mammalian cells after treatment with cryoprotectants such as glycerol or dimethyl sulphoxide, but the rate is not a universal optimum. The 1°C/minute rate can be easily achieved by using a rate-controlled freezer or a benchtop portable freezing container such as CoolCell.
Several independent studies have provided evidence that frozen embryos stored using slow-freezing techniques may in some ways be 'better' than fresh in IVF. The studies were presented at the American Society for Reproductive Medicine conference in San Francisco, US, 2008. The studies indicate that using frozen embryos rather than fresh embryos reduced the risk of stillbirth and premature delivery though the exact reasons are still being explored.[3]
Vitrification
Researchers who have developed a new technique, vitrification, as of 2000 claim to provide the benefits of cryopreservation without damage due to ice crystal formation.[4] In clinical cryopreservation, vitrification usually requires the addition of cryoprotectants prior to cooling. The cryoprotectants act like antifreeze: they lower the freezing temperature. They also increase the viscosity. Instead of crystallizing, the syrupy solution turns into an amorphous ice—i.e., it vitrifies. Rather than a phase change from liquid to solid by crystallization, the amorphous state is like a "solid liquid", and the transformation is over a small temperature range described as the glass transition temperature.
Vitrification of water is promoted by rapid cooling, and can be achieved without cryoprotectants by an extremely rapid drop in temperature (megakelvins per second). The rate that is required to attain glassy state in pure water was considered to be impossible until 2005.[5]
Two conditions usually required to allow vitrification are an increase in the viscosity and a depression of the freezing temperature. Many solutes do both, but larger molecules generally have larger effect, particularly on viscosity. Rapid cooling also promotes vitrification.
In established methods of cryopreservation, the solute must penetrate the cell membrane in order to achieve increased viscosity and depress freezing temperature inside the cell. Sugars do not readily permeate through the membrane. Those solutes that do, such as dimethyl sulfoxide, a common cryoprotectant, are often toxic in high concentration. One of the difficult compromises faced in vitrifying cryopreservation is limiting the damage produced by the cryoprotectant itself due to cryoprotectant toxicity. Mixtures of cryoprotectants and the use of ice blockers have enabled Twenty-First Century Medicine to vitrify a rabbit kidney to -135ºC with their proprietary vitrification cocktail. Upon rewarming, the kidney was successfully transplanted into a rabbit, with complete functionality and viability, able to sustain the rabbit indefinitely as the sole functioning kidney.[6]
Freezable tissues
In general, cryopreservation is easier for thin samples and small clumps of individual cells, because these can be cooled more quickly and so require lower doses of toxic cryoprotectants. Therefore, the goal of cryopreserving human livers and hearts for storage and transplant is still some distance away.
Nevertheless, suitable combinations of cryoprotectants and regimes of cooling and rinsing during warming often allow the successful cryopreservation of biological materials, particularly cell suspensions or thin tissue samples. Examples include:
- Semen
- Blood
- Special cells for transfusion
- Stem cells. It is optimal in high concentration of synthetic serum, stepwise equilibration and slow cooling.[7]
- Umbilical cord blood Further information: Cord blood bank#Cryopreservation
- Tissue samples like tumors and histological cross sections
- Eggs (oocytes) See oocyte cryopreservation
- Embryos that are 2, 4 or 8 cells when frozen
- Ovarian tissue
- Plant seeds or shoots may be cryopreserved for conservation purposes.
In addition, efforts are underway to preserve humans cryogenically, known as cryonics. In such efforts either the brain within the head or the entire body may undergo the above process. Cryonics is in a different category from the aforementioned examples, however: while countless cryopreserved cells, vaccines, tissue and other biologial samples have been thawed and successfully used, this has not yet been the case at all for cryopreserved brains or bodies. At issue are the criteria for defining "success". Proponents of cryonics claim that cryopreservation using present technology, particularly vitrification of the brain, may be sufficient to preserve people in an "information theoretic" sense so that they could be revived and made whole by hypothetical vastly advanced future technology.
Semen
Main article: Semen cryopreservationSemen can be used successfully almost indefinitely after cryopreservation. The longest reported successful storage is 22 years.[8] It can be used for sperm donation where the recipient wants the treatment in a different time or place, or for men undergoing a vasectomy to still have the option to have children.
Testicular tissue
Cryopreservation of immature testicular tissue is a developing method to avail reproduction to young boys who need to go through gonadotoxic therapies. Animal data look promising, since healthy offsprings have been obtained after transplantation of frozen testicular cell suspensions or tissue pieces. However, none of the fertility restoration options from frozen tissue, i.e. cell suspension transplantation, tissue grafting and in vitro maturation (IVM) has proved efficient and safe in humans as yet.[9]
Oocytes
Main article: Oocyte cryopreservationHuman Oocyte cryopreservation is a new technology in which a woman’s eggs (oocytes) are extracted, frozen and stored. Later, when she is ready to become pregnant, the eggs can be thawed, fertilized, and transferred to the uterus as embryos.
Embryos
Main article: Embryo cryopreservationCryopreservation for embryos are used for embryo storage, e.g. when in vitro fertilization has resulted in more embryos than is currently needed.
Pregnancies have been reported from embryos stored for 16 years.[10] Many studies have evaluated the children born from frozen embryos, or “frosties”. The result has uniformly been positive with no increase in birth defects or development abnormalities.[11] A study of more than 11,000 cryopreserved human embryos showed no significant effect of storage time on postthaw survival for IVF or oocyte donation cycles, or for embryos frozen at the pronuclear or cleavage stages.[12] In addition, the duration of storage had no significant effect on clinical pregnancy, miscarriage, implantation, or live birth rate, whether from IVF or oocyte donation cycles.[12] Rather, oocyte age, survival proportion, and number of transferred embryos are predictors of pregnancy outcome.[12]
Ovarian tissue
Main article: Ovarian tissue cryopreservationCryopreservation of ovarian tissue is of interest to women who want to preserve their reproductive function beyond the natural limit, or whose reproductive potential is threatened by cancer therapy,[13] for example in hematologic malignancies or breast cancer.[14] The procedure is to take a part of the ovary and carry out slow freezing before storing it in liquid nitrogen whilst therapy is undertaken. Tissue can then be thawed and implanted near the fallopian, either orthotopic (on the natural location) or heterotopic (on the abdominal wall),[14] where it starts to produce new eggs, allowing normal conception to take place.[15] The ovarian tissue may also be transplanted into mice that are immunocompromised (SCID mice) to avoid graft rejection, and tissue can be harvested later when mature follicles have developed.[16]
Moss
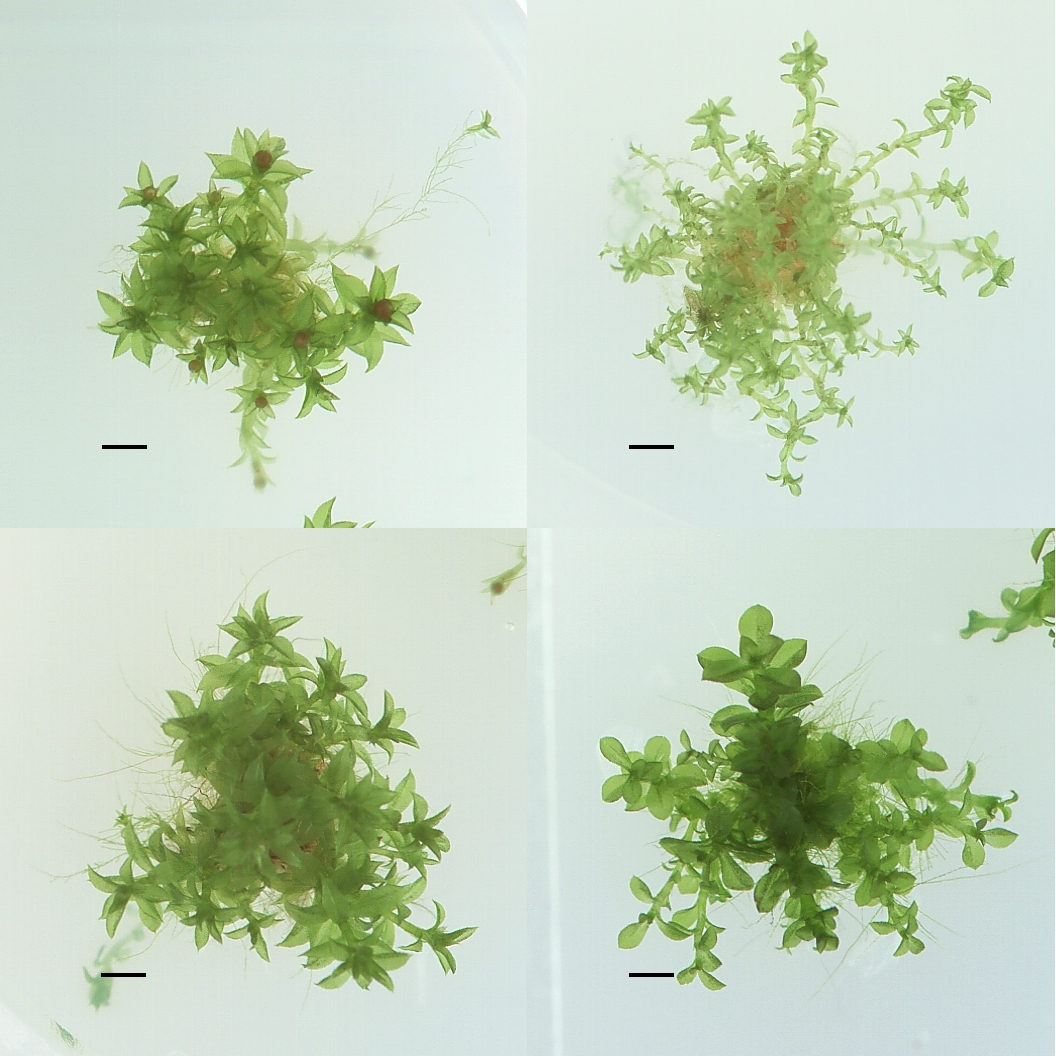
 Four different ecotypes of Physcomitrella patens stored at the IMSC.
Four different ecotypes of Physcomitrella patens stored at the IMSC.Cryopreservation of whole moss plants, especially Physcomitrella patens, has been developed by Ralf Reski and coworkers [17] and is performed at the International Moss Stock Center. This biobank collects, preserves, and distributes moss mutants and moss ecoptypes [18]
Natural cryopreservation
Water bears (Tardigrada), microscopic multicellular organisms, can survive freezing at low temperatures by replacing most of their internal water with the sugar trehalose, preventing it from crystallization that otherwise damage cell membranes. Mixtures of solutes can achieve similar effects. Some solutes, including salts, have the disadvantage that they may be toxic at high concentrations. In addition to the Water bear, wood frogs can tolerate the freezing of their blood and other tissues. Urea is accumulated in tissues in preparation for overwintering, and liver glycogen is converted in large quantities to glucose in response to internal ice formation. Both urea and glucose act as "cryoprotectants" to limit the amount of ice that forms and to reduce osmotic shrinkage of cells. Frogs can survive many freeze/thaw events during winter if not more than about 65% of the total body water freezes. Research exploring the phenomenon of "Freezing frogs" has been primarily carried out by the Canadian researcher, Dr. Kenneth B. Storey.
Freeze tolerance, in which organisms survive the winter by freezing solid and ceasing life functions, is known in a few vertebrates: five species of frogs (Rana sylvatica, Pseudacris triseriata, Hyla crucifer, Hyla versicolor, Hyla chrysoscelis), one salamander (Hynobius keyserlingi), one snake (Thamnophis sirtalis) and three turtles (Chrysemys picta, Terrapene carolina, Terrapene ornata).[19] Snapping turtle Chelydra serpentina and wall lizard Podarcis muralis also survive nominal freezing but it has not been established to be adaptive for overwintering. In the case of Rana sylvatica one cryopreservant is ordinary glucose, which rises in concentration by approximately 19 mmol/l when the frogs are slowly cooled;[19]
History
One of the most important early workers on the theory of cryopreservation was James Lovelock of Gaia theory fame. He suggested that damage to red blood cells during freezing was due to osmotic stresses. Lovelock in early 1950s had also suggested that increasing salt concentrations in a cell as it dehydrates to lose water to the external ice might cause damages to the cell.[20] Cryopreservation of tissue in recent times started with the freezing of fowl sperm, which in 1957 was cryopreserved by a team of scientists in the UK led by Christopher Polge.[21] The process moved into the human world in the 1950s with pregnancies obtained after insemination of frozen sperm. However, the rapid immersion of the samples in liquid nitrogen did not, for certain of these samples–such as types of embryos, bone marrow and stem cells–produce the necessary viability to make them usable on thawing. Increased understanding of the mechanism of freezing injury to cells emphasised the importance of controlled or slow cooling to obtain maximum survival on thawing of the living cells. A controlled rate cooling process, allowing biological samples to equilibrate to optimal physical parameters osmotically in a cryoprotectant (a form of anti-freeze) before cooling in a predetermined, controlled way proved necessary. The ability of cryoprotectants, in the early cases glycerol, to protect cells from freezing injury was discovered accidentally. Freezing injury has two aspects–direct damage from the ice crystals and secondary damage caused by the increase in concentration of solutes as progressively more ice is formed. In 1963 Peter Mazur, at Oak Ridge National Laboratory in the USA, showed that lethal intracellular freezing could be avoided if cooling was slow enough to permit sufficient water to leave the cell during progressive freezing of the extracellular fluid. That rate differs between cells of differing size and water permeability: a typical cooling rate around 1°C/minute is appropriate for many mammalian cells after treatment with cryoprotectants such as glycerol or dimethyl sulphoxide, but the rate is not a universal optimum.
See also
- Chemical brain preservation
- Cryobiology
- Cryonics
- Cryogenics
- Cryostasis (clathrate hydrates)
- Ex-situ conservation
- Frozen Zoo
References
- ^ Vutyavanich T, Piromlertamorn W, Nunta S (April 2010). "Rapid freezing versus slow programmable freezing of human spermatozoa". Fertil. Steril. 93 (6): 1921–8. doi:10.1016/j.fertnstert.2008.04.076. PMID 19243759.
- ^ "?". http://www.bionews.org.uk/commentary.lasso?storyid=4055.[dead link]
- ^ (PDF) Supplement to Fertility and Sterility. 90. September 2008. http://www.asrm.org/Professionals/Meetings/sanfrancisco2008/Abstracts2008.pdf. Retrieved 2009-07-27.[dead link]
- ^ "Alcor: The Origin of Our Name". Alcor Life Extension Foundation. Winter 2000. http://www.alcor.org/cryonics/cryonics2000-4.pdf. Retrieved 2009-08-25.
- ^ Bhat SN, Sharma A, Bhat SV (2005). "Vitrification and glass transition of water: insights from spin probe ESR". Phys Rev Lett 95 (23): 235702. Bibcode 2005PhRvL..95w5702B. doi:10.1103/PhysRevLett.95.235702. PMID 16384318.
- ^ Fahy GM, Wowk B, Pagotan R, Chang A, Phan J, Thomson B, Phan L (2009). "Physical and biological aspects of renal vitrification". Organogenesis 5 (3): 167–175. doi:10.4161/org.5.3.9974. PMC 2781097. PMID 20046680. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2781097.
- ^ Lee JY, Lee JE, Kim DK, Yoon TK, Chung HM, Lee DR (November 2008). "High concentration of synthetic serum, stepwise equilibration and slow cooling as an efficient technique for large-scale cryopreservation of human embryonic stem cells". Fertil. Steril. 93 (3): 976–85. doi:10.1016/j.fertnstert.2008.10.017. PMID 19022437.
- ^ Planer NEWS and Press Releases > Child born after 22 year semen storage using Planer controlled rate freezer 14/10/2004
- ^ Wyns C, Curaba M, Vanabelle B, Van Langendonckt A, Donnez J (2010). "Options for fertility preservation in prepubertal boys". Hum. Reprod. Update 16 (3): 312–28. doi:10.1093/humupd/dmp054. PMID 20047952.
- ^ Planer NEWS and Press Releases > 'Twins' born 16 years apart. 01/06/2006
- ^ "Genetics & IVF Institute". Givf.com. Archived from the original on 2009-07-27. http://web.archive.org/web/*/http://givf.com/embryov.cfm. Retrieved 2009-07-27.
- ^ a b c Riggs R, Mayer J, Dowling-Lacey D, Chi TF, Jones E, Oehninger S (November 2008). "Does storage time influence postthaw survival and pregnancy outcome? An analysis of 11,768 cryopreserved human embryos". Fertil. Steril. 93 (1): 109–15. doi:10.1016/j.fertnstert.2008.09.084. PMID 19027110.
- ^ Isachenko V, Lapidus I, Isachenko E, et al. (2009). "Human ovarian tissue vitrification versus conventional freezing: morphological, endocrinological, and molecular biological evaluation.". Reproduction 138 (2): 319–27. doi:10.1530/REP-09-0039. PMID 19439559.
- ^ a b Oktay K, Oktem O (November 2008). "Ovarian cryopreservation and transplantation for fertility preservation for medical indications: report of an ongoing experience". Fertil. Steril. 93 (3): 762–8. doi:10.1016/j.fertnstert.2008.10.006. PMID 19013568.
- ^ Livebirth after orthotopic transplantation of cryopreserved ovarian tissue The Lancet, September 24, 2004
- ^ Lan C, Xiao W, Xiao-Hui D, Chun-Yan H, Hong-Ling Y (December 2008). "Tissue culture before transplantation of frozen-thawed human fetal ovarian tissue into immunodeficient mice". Fertil. Steril. 93 (3): 913–9. doi:10.1016/j.fertnstert.2008.10.020. PMID 19108826.
- ^ Schulte, J., Ralf Reski (2004): High-throughput cryopreservation of 140000 Physcomitrella patens mutants. Plant Biol. 6, 119-127. Schulte J.; Reski R.. "High throughput cryopreservation of 140,000 Physcomitrella patens mutants". Plant Biotechnology, Freiburg University, Freiburg, Germany. http://www.ncbi.nlm.nih.gov/pubmed/15045662. Retrieved 17 August 2010.
- ^ ScienceDaily: Mosses, deep frozen. "?". http://www.sciencedaily.com/releases/2010/02/100224134325.htm.
- ^ a b Jon P. Costanzo, Richard E. Lee, Michael F. Wright (1991). "Glucose loading prevents freezing injury in rapidly cooled wood frogs". American Journal of Physiology: R1549–R1553. http://www.units.muohio.edu/cryolab/publications/documents/CostanzoLeeWright91AJP.pdf.
- ^ Mazur P (1970). "Cryobiology: the freezing of biological systems". Science 168 (3934): 939–49. doi:10.1126/science.168.3934.939. PMID 5462399.
- ^ Polge C (1957). "Low-Temperature Storage of Mammalian Spermatozoa". Royal Society of London 147 (929): 498–508. doi:10.1098/rspb.1957.0068.
7. Engelmann, F., M. E. Dulloo, C. Astorga, S. Dussert and F. Anthony, editors (2007). Conserving coffee genetic resources. Bioversity International, CATIE, IRD. http://www.bioversityinternational.org/Publications/pubfile.asp?ID_PUB=1244. 61 p.
8. Panis, B and Tien Thinh, N. (2001). Cryopreservation of Musa germplasm. INIBAP (now Bioversity International). http://www.bioversityinternational.org/Publications/pubfile.asp?ID_PUB=722. 45 p.
External links
- Vitrification for storage of embryos, HFEA website
- Photo of Programmable Freezer
- Mouse Embryo Freezer[dead link]
- The Freezing of Human Oocytes (Eggs)
- Society for Cryobiology
- The Society for Low Temperature Biology
- Cellular cryobiology and anhydrobiology
- Death in the Deep Freeze
- In vitro storage and cryopreservation
- Cryonics
- Cryogenics
Categories:


Wikimedia Foundation. 2010.