- Kyphosis
-
"Hunchback" redirects here. For other uses, see Hunchback (disambiguation).
Kyphosis Classification and external resources 
A preoperative image of a 22-year-old male with Scheuermann's disease, a type of structural kyphosisICD-10 M40.0-M40.2, M42.0, E64.3,Q76.4, M84.0, M96.2, M96.3 ICD-9 732.0, 737.0, 737.1, 756.19 DiseasesDB 21885 MedlinePlus 001240 MeSH D007738 Kyphosis (Greek - kyphos, a hump), also called roundback or Kelso's hunchback, is a condition of over-curvature of the thoracic vertebrae (upper back). It can be either the result of degenerative diseases (such as arthritis), developmental problems (the most common example being Scheuermann's disease), osteoporosis with compression fractures of the vertebrae, and/or trauma.
In the sense of a deformity, it is the pathological curving of the spine, where parts of the spinal column lose some or all of their lordotic profile. This causes a bowing of the back, seen as a slouching posture.
While most cases of kyphosis are mild and only require routine monitoring, serious cases can be debilitating. High degrees of kyphosis can cause severe pain and discomfort, breathing and digestion difficulties, cardiovascular irregularities, neurological compromise, and in the more severe cases, significantly shortened life-spans. These types of high end curves typically do not respond well to conservative treatment, and almost always warrant spinal fusion surgery, which can successfully restore the body's natural degree of curvature.
The Cobb angle is the preferred method of measuring kyphosis.Contents
Classification
There are several kinds of kyphosis (ICD-10 codes are provided):
- Postural kyphosis (M40.0), the most common type, normally attributed to slouching, can occur in both the old[1] and the young. In the young, it can be called 'slouching' and is reversible by correcting muscular imbalances. In the old, it may be called 'hyperkyphosis' or 'dowager’s hump'. About one third of the most severe hyperkyphosis cases have vertebral fractures.[2] Otherwise, the aging body tends towards a loss of musculoskeletal integrity,[3] and kyphosis can develop due to aging alone.[2][4]
- Scheuermann's kyphosis (M42.0) is significantly worse cosmetically and can cause varying degrees of pain, and can also affect different areas of the spine (the most common being the mid-thoracic area). Scheuermann's disease is considered a form of juvenile osteochondrosis of the spine, and is more commonly called Scheuermann's disease. It is found mostly in teenagers and presents a significantly worse deformity than postural kyphosis. A patient suffering from Scheuermann’s kyphosis cannot consciously correct posture.[5] The apex of the curve, located in the thoracic vertebrae, is quite rigid. The patient may feel pain at this apex, which can be aggravated by physical activity and by long periods of standing or sitting. This can have a significantly detrimental effect on their lives, as their level of activity is curbed by their condition; they may feel isolated or uneasy amongst peers if they are children, depending on the level of deformity. Whereas in postural kyphosis, the vertebrae and disks appear normal, in Scheuermann’s kyphosis, they are irregular, often herniated, and wedge-shaped over at least three adjacent levels. Fatigue is a very common symptom, most likely because of the intense muscle work that has to be put into standing and/or sitting properly. The condition appears to run in families. Most patients who undergo surgery to correct their kyphosis have Scheuermann's disease.
- Congenital kyphosis (Q76.4) can result in infants whose spinal column has not developed correctly in the womb. Vertebrae may be malformed or fused together and can cause further progressive kyphosis as the child develops.[6] Surgical treatment may be necessary at a very early stage and can help maintain a normal curve in coordination with consistent follow ups to monitor changes. However, the decision to carry out the procedure can be very difficult due to the potential risks to the child. A congenital kyphosis can also suddenly appear in teenage years, more commonly in children with cerebral palsy and other neurological disorders.
- Nutritional kyphosis can result from nutritional deficiencies, especially during childhood, such as vitamin D deficiency (producing rickets), which softens bones and results in curving of the spine and limbs under the child's body weight.
- Gibbus deformity is a form of structural kyphosis, often a sequela to tuberculosis.
- Post-traumatic kyphosis (M84.0) after untreated or not treated effectively vertebral fractures
Treatments
Orthosis (brace)
 Modern brace for the treatment of a thoracic kyphosis. The brace is constructed using a CAD / CAM device. At this stage, this is the only CAD / CAM brace designed to treat a thoracic kyphosis. It is called kyphologic.[7]
Modern brace for the treatment of a thoracic kyphosis. The brace is constructed using a CAD / CAM device. At this stage, this is the only CAD / CAM brace designed to treat a thoracic kyphosis. It is called kyphologic.[7]
Body braces showed benefit in a randomised controlled trial.[8]
The Milwaukee brace is one particular body brace that is often used to treat kyphosis in the US. Modern CAD / CAM braces are used in Europe to treat different types of kyphosis. These are much easier to wear and have better in-brace corrections than reported for the Milwaukee brace. Since there are different curve patterns (thoracic, thoracolumbar and lumbar) different types of braces are in use. The advantages / disadvantages of different braces are discussed in a recent review article.[7]
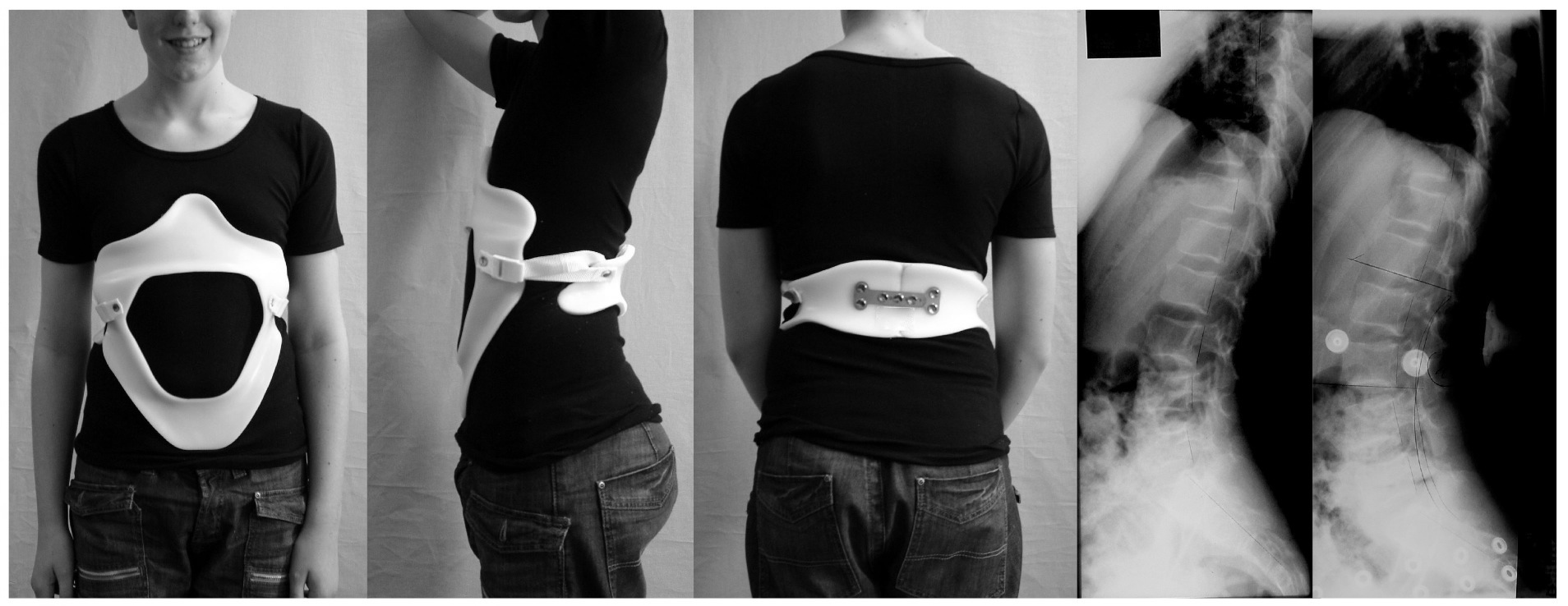
 Modern brace for the treatment of a lumbar / thoracolumbar kyphosis. The brace is constructed using a CAD / CAM device. At this stage this brace is the only CAD / CAM brace designed to treat a lumbar kyphosis and is called physio-logic brace. Restoration of the lumbar lordosis is the major aim.[7]
Modern brace for the treatment of a lumbar / thoracolumbar kyphosis. The brace is constructed using a CAD / CAM device. At this stage this brace is the only CAD / CAM brace designed to treat a lumbar kyphosis and is called physio-logic brace. Restoration of the lumbar lordosis is the major aim.[7]Specialised physical therapy
In Germany, a standard treatment for both Scheuermann's disease and lumbar kyphosis is the Schroth method, a system of physical therapy for scoliosis and related spinal deformities.[9]
Surgery
Surgical treatment can be used in severe cases. In patients with progressive kyphotic deformity due to vertebral collapse, a procedure called a kyphoplasty may arrest the deformity and relieve the pain. Kyphoplasty is a minimally invasive procedure, requiring only a small opening in the skin. The main goal is to return the damaged vertebra as close as possible to its original height.[10]
Complications
The risk of serious complications from spinal fusion surgery for kyphosis is estimated to be 5%, similar to the risks of surgery for scoliosis. Possible complications may be inflammation of the soft tissue or deep inflammatory processes, breathing impairments, bleeding, and nerve injuries. According to the latest evidence, the actual rate of complications may be substantially higher. Even among those who do not suffer serious complications, 5% of patients require reoperation within five years of the procedure, and in general it is not yet clear what to expect from spine surgery in the long-term.[11][12] Taking into account that signs and symptoms of spinal deformity cannot be changed by surgical intervention, surgery remains to be a cosmetic indication.[11][13] Unfortunately, the cosmetic effects of surgery are not necessarily stable.[11] In case one decides to undergo surgery, a specialised centre should be preferred.
See also
- Ehlers–Danlos syndrome
- Hyperkyphosis
- Lordosis
- Pott's disease
- Scoliosis
References
- ^ Annals of Human Biology, Volume 1, Number 3 / July 1974.
- ^ a b Kado DM, Prenovost K, Crandall C (2007). "Narrative review: hyperkyphosis in older persons". Ann. Intern. Med. 147 (5): 330–8. PMID 17785488. http://www.annals.org/cgi/content/full/147/5/330.
- ^ Keller TS, Harrison DE, Colloca CJ, Harrison DD, Janik TJ (2003). "Prediction of osteoporotic spinal deformity". Spine 28 (5): 455–62. doi:10.1097/00007632-200303010-00009. PMID 12616157.
- ^ Osteopathy: A Complete Health Care System, by Leon Chaitow N.D., D.O., M.R.O.
- ^ Back.com and [1] Emedicine.com
- ^ Natural History of Congenital Kyphosis and Kyphoscoliosis. A Study of One Hundred and Twelve Patients - MCMASTER and SINGH 81 (10): 1367 - Journal of Bone no People and Joint Surgery
- ^ a b c Weiss HR, Turnbull D. 2010. Kyphosis (Physical and technical rehabilitation of patients with Scheuermann's disease and kyphosis). In: JH Stone, M Blouin, editors. International Encyclopedia of Rehabilitation. Available online: http://cirrie.buffalo.edu/encyclopedia/article.php?id=125&language=en
- ^ Pfeifer M, Begerow B, Minne HW (2004). "Effects of a new spinal orthosis on posture, trunk strength, and quality of life in women with postmenopausal osteoporosis: a randomized trial". American journal of physical medicine & rehabilitation / Association of Academic Physiatrists 83 (3): 177–86. doi:10.1097/01.PHM.0000113403.16617.93. PMID 15043351.
- ^ Lehnert-Schroth, Christa (2007). Three-Dimensional Treatment for Scoliosis: A Physiotherapeutic Method for Deformities of the Spine. (Palo Alto, CA: The Martindale Press): 185-187 and passim.
- ^ http://www.spineuniversity.com/kyphoplasty
- ^ a b c Hawes M. 2006. Impact of spine surgery on signs and symptoms of spinal deformity. Pediatr Rehabil. Oct-Dec;9(4):318-39.
- ^ Weiss HR, Goodall D: Rate of complications in scoliosis surgery - a systematic review of the Pub Med literature. Scoliosis. 2008 Aug 5;3:9.
- ^ Hawes MC, O'Brien JP. 2008. A century of spine surgery: What can patients expect? Disabil Rehabil. 30(10):808-17.
External links
- AAOS.org, Kyphosis (Curvature of the spine)
Dorsopathies / spinal disease (M40–M54, 720–724, 737) Deforming dorsopathies OtherSpondylopathy inflammatory: Spondylitis (Ankylosing spondylitis) · Sacroiliitis · Discitis · Spondylodiscitis · Pott diseaseBack pain Intervertebral disc disorder M: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Congenital malformations and deformations of musculoskeletal system / musculoskeletal abnormality (Q65–Q76, 754–756.3) Appendicular
limb / dysmeliahand deformity:Lowerhip:knee:Genu valgum · Genu varum · Genu recurvatum · Discoid meniscus · Congenital patellar dislocation · Congenital knee dislocationfoot deformity:Either / bothdactyly / digit:reduction deficits / limb:multiple joints:Axial Craniofacial dysostosis:other:spinal curvature (Scoliosis) · Klippel-Feil syndrome · Spondylolisthesis · Spina bifida occulta · SacralizationThoracic skeletonribs:sternum:M: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Categories:- Deforming dorsopathies
- Congenital disorders of musculoskeletal system


Wikimedia Foundation. 2010.