- Trigonocephaly
-
Trigonocephaly Classification and external resources ICD-10 Q75.0 ICD-9 756.0 DiseasesDB 33252 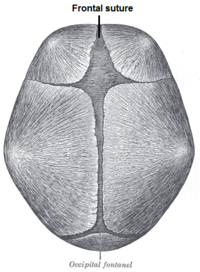
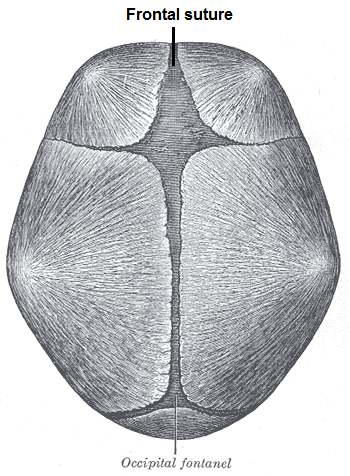
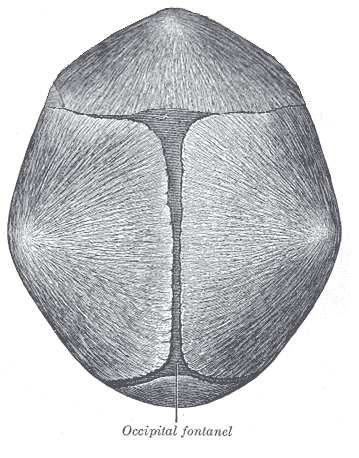
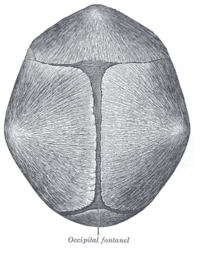 Fused suture in trigonocephaly
Fused suture in trigonocephalyTrigonocephaly (Greek: 'trigonon' = triangle, 'kephale' = head) is a congenital condition of premature fusion of the metopic suture (Greek: 'metopon' = forehead) leading to a triangular shaped forehead. The merging of the two frontal bones leads to transverse growth restriction and parallel growth expansion. It may occur syndromic involving other abnormalities or isolated.
Contents
History
In former times people born with malformed skulls were rejected based upon their appearance.[1] This still persists today in various parts of the world even though the intellectual development is often normal.[2] The Austrian physician Franz Joseph Gall presented the science of phrenology in the early 19th century through his work The Anatomy and Physiology of the Nervous System in General, and of the Brain in Particular.[3][4]
Hippocrates described trigonocephaly as follows: Men's heads are by no means all like to one another, nor are the sutures of the head of all men constructed in the same form. Thus, whoever has a prominence in the anterior part of the head (by prominence is meant the round protuberant part of the bone which projects beyond the rest of it), in him the sutures of the head take the form of the Greek letter 'tau', τ.[5][6]
Hermann Welcker coined the term trigonocephaly in 1862. He described a child with a V-shaped skull and a cleft lip.[7]
Etiology
Trigonocephaly can either occur syndromatic or isolated. Trigonocephaly is associated with the following syndromes: Opitz syndrome, Muenke syndrome, Jacobsen syndrome, Baller-Gerold syndrome and Say-Meyer syndrome. The etiology of trigonocephaly is mostly unknown although there are three main theories.[1] Trigonocephaly is probably a multifactorial congenital condition, but due to limited proof of these theories this cannot safely be concluded.[2]
Intrinsic bone malformation
The first theory assumes that the origin of pathological synostosis lies within disturbed bone formation early on in the pregnancy. Causes can either be genetic[8][9][10][11] (9p22-24, 11q23, 22q11, FGFR1 mutation[12]), metabolic[13] (TSH suppletion in hypothyroidism[14][15]) or pharmaceutical[16] (valproate in epilepsy[17][18]).
Fetal head constrain
The second theory says that synostosis begins when the foetal head gets hindered in the pelvic outlet during birth.[19][20]
Intrinsic brain malformation
The third theory predominates disturbed brain formation of the two frontal lobes as the main issue behind synostosis.[21][22][23] Limited growth of the frontal lobes leads to an absence of stimuli for cranial growth, therefore causing premature fusion of the metopic suture.
Epidemiology
The incidence of metopic synostosis is roughly between 1:700 and 1:15.000 newborns globally (differs per country).[16][24] Trigonocephaly is seen more in males than females ranging from 2:1 to 6,5:1.[25][26][27][28] Hereditary relations in metopic synostosis have been found of which 5,5% were well defined syndromic.[16] Maternal age and a birth weight of less than 2500g may also play a role in trigonocephaly.[29] These data are based on estimations and do not give factual information.
Only one article gives valuable and reliable information regarding the incidence of metopic synsostosis in the Netherlands. The incidence in the Netherlands showed an increase from 0.6 (1997) to 1.9 (2007) for every 10.000 live births.[30]
Diagnosis
Diagnosis can be characterized by typical facial and cranial deformities.[2][31]
Observatory signs of trigonocephaly are:
- a triangular shaped forehead seen from top view leading to a smaller anterior cranial fossa
- a visible and palpable midline ridge
- hypotelorism inducing ethmoidal hypoplasia
Imaging techniques (3D-CT, Röntgenography, MRI) show:- epicanthal folds in limited cases
- teardrop shaped orbits angulated towards the midline of the forehead ('surprised coon' sign) in severe cases
- a contrast difference between a röntgenograph of a normal and a trigonocephalic skull
- anterior curving of the metopic suture seen from lateral view of the cranium on a röntgenograph
- a normal cephalic index (maximum cranium width / maximum cranium length) however, there is bitemporal shortening and biparietal broadening
The neuropsychological development is not always affected. These effects are only visible in a small percentage of children with trigonocephaly or other suture synostoses. Neuropsychological signs are:- problems in behaviour, speech and language
- neurodevelopmental delays such as ADHD (Attention Deficit Hyperactivity Disorder), ODD (Oppositional Defiant Disorder), ASD (Autism Spectrum Disorder) and CD (Conduct Disorder).[34][35][36][37] Many of these delays become evident at school age.[38]
Treatment
Treatment is surgical with attention to form and volume. Surgery usually takes place before the age of one since it has been reported that the intellectual outcome is better.[27][28][32][33][34][39][40][41][42]
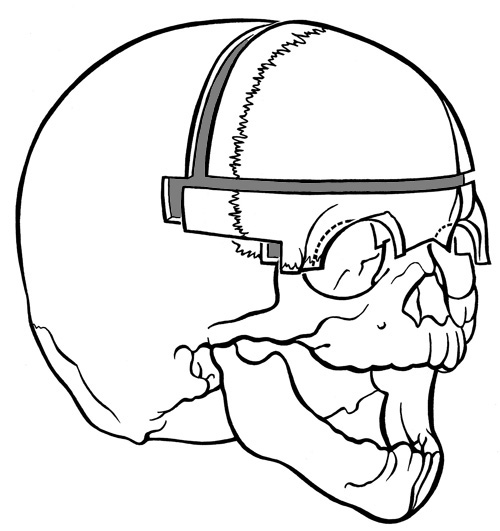
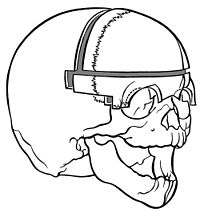 A. Fronto-supraorbital advancement and remodelling - before remodelling.
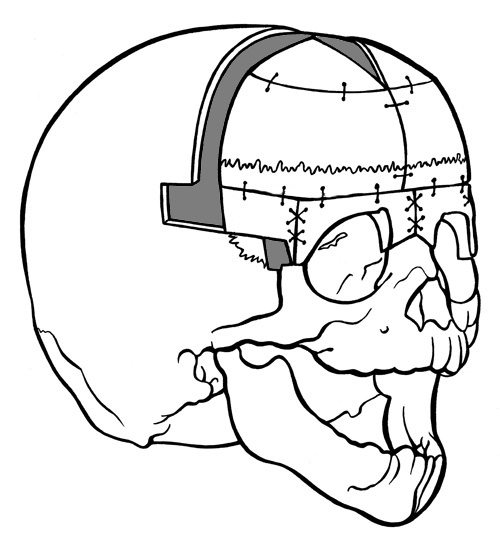
A. Fronto-supraorbital advancement and remodelling - before remodelling.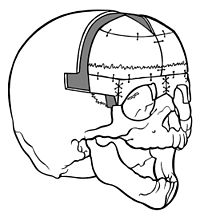 B. Fronto-supraorbital advancement and remodelling - after remodelling.
B. Fronto-supraorbital advancement and remodelling - after remodelling.Fronto-supraorbital advancement and remodelling[43]
A form of surgery is the so called fronto-supraorbital advancement and remodelling. Firstly, the supraorbital bar is remodelled by a wired greenstick fracture to straighten it. Secondly, the supraorbital bar is moved 2 cm. forward and fixed only to the frontal process of the zygoma without fixation to the cranium. Lastly, the frontal bone is divided into two, rotated and attached to the supraorbital bar causing a nude area (craniectomy) between the parietal bone and frontal bone. Bone will eventually regenerate since the dura mater lies underneath (the dura mater has osteogenic capabilities). This results in an advancement and straightening of the forehead.
‘Floating forehead technique’[2]
The so-called ‘floating forehead technique’ combined with the remodelling of the supraorbital bar is derived from the fronto-supraorbital advancement and remodelling. The supraorbital bar is remodelled as described above.[44] The frontal bone is split in two pieces. Instead of using both pieces as in fronto-supraorbital advancement and remodelling, only one piece is rotated and attached to the supraorbital bar. This technique also leaves a craniectomy behind.[45]
Other
- Suturectomy[2]
Distraction osteogenesis is based on creating more cranial space for the brain by gradually moving the bones apart. This can be achieved by using springs.[48]- Minimal invasive endoscopic surgery[2]
These approaches are 2D solutions for a 3D problem, therefore the results are not optimal. Distraction osteogenesis and minimal invasive endoscopic surgery are yet in experimental fase.Treatment results
Surgical
Trigonocephaly seems to be the most compliant form of craniosynostosis for surgery.[34] Because of standardization of current surgical approaches there is no surgical mortality and complications are few to none.[2][49][50] The simple suturectomy is presently insufficient to adjust the complicated growth restrictions caused by metopic synostosis.[2] On the other hand the fronto-supraorbital advancement and remodelling and the ‘floating forehead technique’ create sufficient space for brain growth and result in a normal horizontal axis of the orbits and supraorbital bar. The fronto-supraorbital advancement and remodelling is the most used method nowadays.[49] Over the past few years distraction osteogenesis has been gradually acknowledged since it has a positive effect on hypotelorism. Expanding the distance between the orbits using springs seems to be successful.[2][51][52][53] However, there are discussions whether hypotelorism really needs to be corrected.[54] The minimal invasive endoscopic surgery has been gaining attention since the early 90’s, however, it has technical limitations (only strip craniectomy is possible).[2] Attempts have been made to reach beyond these limits.[55][56][57][58][59]
Aesthetic
Aesthetic outcome of metopic synostosis surgery is persistently good with reoperation hazards below 20%.[60][61] In 1981 Anderson advised that craniofacial operations for synostosis should be as extensive as necessary after a study of 107 cases of metopic and coronal synostosis.[33] Surgery does not provide a 100% natural outcome, mostly there will be minor irregularities. Reoperations are usually performed on more severe cases (including syndromic metopic synostosis). The hypotelorism and temporal hollowing are the most difficult to correct: the hypotelorism usually remains under corrected and a second operation is often needed for correction of temporal hollowing.[60][62]
Neurological
The highest rate of neurological problems of single suture synostosis are seen in patients with trigonocephaly.[2] Surgery is performed generally before the age of one because of claims of better intellectual outcome.[27][28][32][33][34][39][40][41][42] Seemingly surgery does not influence the high incidence of neurodevelopment problems in patients with metopic synostosis. Neurological disorders such as ADHD, ASD, ODD and CD are seen in patients with trigonocephaly. These disorders are usually also associated with decreased IQ. The presence of ADHD, ASD and ODD is higher in cases with an IQ below 85. This is not the case with CD which showed an insignificant increase at an IQ below 85.[2]
References
- ^ a b Strickler M, van der Meulen J, Rahael B, Mazolla R. Craniofacial malformations. Edinburgh, London, Melbourne, New York: Churchill Livingston, 1990.Vermeij-Keers, C; Mazzola, RF; Van Der Meulen, JC; Strickler, M (1983). "Cerebro-craniofacial and craniofacial malformations: An embryological analysis". The Cleft palate journal 20 (2): 128–45. PMID 6406099.
- ^ a b c d e f g h i j k l m van der Meulen J.J.N.M (2009). 'On Trigonocephaly'. Publisher: Optima Grafische Communicatie. ISBN 9789085596011
- ^ Wikipedia. http://en.wikipedia.org/wiki/Cognitive_neuroscience.
- ^ Phrenology. http://www.phrenology.org/
- ^ Hippocrates. On injuries of the head. Med classics 1938: 3: 145-60.
- ^ Dimopoulos VG, Machinis TG, Fountas KN, Robinson JS. Head injury management algorithm as describes in Hippocrates' Peri ton en cephali traumaton. Neurosurgery 2005: 57: 1303-5; Discussion 03-5.Dimopoulos, VG; MacHinis, TG; Fountas, KN; Robinson, JS (2005). "Head injury management algorithm as described in Hippocrates' "peri ton en cephali traumaton"". Neurosurgery 57 (6): 1303–5; discussion 1303–5. PMID 16331180.
- ^ Welcker H. Untersugungen uber wachtsum und bau des menschlischen Schädels. Leipzig: Engelmann, 1862.
- ^ Wilkie AO. Craniosynostosis: genes and mechanisms. Hum Mol Genet 1997: 6: 1647-56.Wilkie, AO (1997). "Craniosynostosis: Genes and mechanisms". Human molecular genetics 6 (10): 1647–56. doi:10.1093/hmg/6.10.1647. PMID 9300656.
- ^ Wilkie AO, Bochukova EG, Hansen RM, et al. Clinical dividends from the molecular genetic diagnosis of craniosynostosis.Wilkie, AO; Bochukova, EG; Hansen, RM; Taylor, IB; Rannan-Eliya, SV; Byren, JC; Wall, SA; Ramos, L et al. (2007). "Clinical dividends from the molecular genetic diagnosis of craniosynostosis". American journal of medical genetics. Part A 143A (16): 1941–9. doi:10.1002/ajmg.a.31905. PMID 17621648.
- ^ Frydman M, Kauschansky A, Elian E. Trigonocephaly; a new familiail syndrome. Am J Med Genet 1984: 18: 55-9.Frydman, M; Kauschansky, A; Elian, E; Opitz, John M. (1984). "Trigonocephaly: A new familial syndrome". American journal of medical genetics 18 (1): 55–9. doi:10.1002/ajmg.1320180109. PMID 6741996.
- ^ Hennekam RC, van den Boogaard MJ. Autosomal dominant craniosynostosis of the sutura metopica. Clin genet 1990: 38: 374-7.Hennekam, RC; Van Den Boogaard, MJ (1990). "Autosomal dominant craniosynostosis of the sutura metopica". Clinical genetics 38 (5): 374–7. PMID 2282717.
- ^ Kress W, Petersen B, Collmann H, Grimm T. An unusual FGFR1 mutation (fibroblast growth factor receptor 1 mutation) in a girl with non-syndromic trigonocephaly. Cytogenet Cell Genet 2000:91: 138-40.Kress, W; Petersen, B; Collmann, H; Grimm, T (2000). "An unusual FGFR1 mutation (fibroblast growth factor receptor 1 mutation) in a girl with non-syndromic trigonocephaly". Cytogenetics and cell genetics 91 (1–4): 138–40. doi:10.1159/000056834. PMID 11173846.
- ^ Penfold JL, Simpson DA. Premature craniosynostosis-a complication of thyroid replacement therapy. J Pediatr 1975: 86: 360-3.Penfold, JL; Simpson, DA (1975). "Premature craniosynostosis-a complication of thyroid replacement therapy". The Journal of pediatrics 86 (3): 360–3. doi:10.1016/S0022-3476(75)80963-2. PMID 1113223.
- ^ Johnsonbaugh RE, Bryan RN, Hierlwimmer R, Georges LP. Premature craniosynostosis; A common complication of juvenile thyrotoxicosis. J Pediatr 1978: 93: 188-91.Johnsonbaugh, RE; Bryan, RN; Hierlwimmer, R; Georges, LP (1978). "Premature craniosynostosis: A common complication of juvenile thyrotoxicosis". The Journal of pediatrics 93 (2): 188–91. doi:10.1016/S0022-3476(78)80493-4. PMID 209162.
- ^ Rasmussen SA, Yazdy MM, Carmichael SL, et al. Maternal thyroid disease as a risk factor for craniosynostosis. Obstet Gynecol 2007: 110: 369-77.Rasmussen, SA; Yazdy, MM; Carmichael, SL; Jamieson, DJ; Canfield, MA; Honein, MA (2007). "Maternal thyroid disease as a risk factor for craniosynostosis". Obstetrics and gynecology 110 (2 Pt 1): 369–77. doi:10.1097/01.AOG.0000270157.88896.76. PMID 17666613.
- ^ a b c Lajeunie E, Le_Merrer M, Marchac D, Renier D. Syndromal and nonsyndromal primary trigonocephaly: analysis of a series of 237 patients. American Journal of Medical Genetics 1998: 75: 211-5.Lajeunie, E; Le Merrer, M; Marchac, D; Renier, D (1998). "Syndromal and nonsyndromal primary trigonocephaly: Analysis of a series of 237 patients". American journal of medical genetics 75 (2): 211–5. doi:10.1002/(SICI)1096-8628(19980113)75:2<211::AID-AJMG19>3.0.CO;2-S. PMID 9450889.
- ^ Valentin M, Ducarme G, Yver C, Vuillard E, Belarbi N, Renier D, Luton D. Trigonocephaly and valproate: a case report and review of literature. Prenat Diagn 2008: 28: 259-261.Valentin, M; Ducarme, G; Yver, C; Vuillard, E; Belarbi, N; Renier, D; Luton, D (2008). "Trigonocephaly and valproate: A case report and review of literature". Prenatal diagnosis 28 (3): 259–61. doi:10.1002/pd.1948. PMID 18264949.
- ^ Ardinger HH, Atkin JF, Blackston RD, et al. Verification of the fetal valproate syndrome phenotype. Am J Med Genet 1988: 29: 171-85Ardinger, HH; Atkin, JF; Blackston, RD; Elsas, LJ; Clarren, SK; Livingstone, S; Flannery, DB; Pellock, JM et al. (1988). "Verification of the fetal valproate syndrome phenotype". American journal of medical genetics 29 (1): 171–85. doi:10.1002/ajmg.1320290123. PMID 3125743.
- ^ Graham JM Jr., Smith DW. Metopic craniosynostisis as a consequence of fetal head constraint; two interesting experiments of nature. Pediatrics 1980: 65: 1000-2.Graham Jr, JM; Smith, DW (1980). "Metopic craniostenosis as a consequence of fetal head constraint: Two interesting experiments of nature". Pediatrics 65 (5): 1000–2. PMID 7367110.
- ^ Smartt JM Jr., Karmacharya J, Gannon FH, et al. Intrauterine fetal constraint induces chondrocyte apoptosis and premature ossification of the cranial base. Plast Reconstr Surg 2005: 116: 1363-9.Smartt Jr, JM; Karmacharya, J; Gannon, FH; Teixeira, C; Mansfield, K; Hunenko, O; Shapiro, IM; Kirschner, RE (2005). "Intrauterine fetal constraint induces chondrocyte apoptosis and premature ossification of the cranial base". Plastic and reconstructive surgery 116 (5): 1363–9. doi:10.1097/01.prs.0000182224.98761.cf. PMID 16217480.
- ^ Riemenschneider PA. Trigonocephaly. Radiology 1957: 68: 863-5.Riemenschneider, PA (1957). "Trigonocephaly". Radiology 68 (6): 863–5. PMID 13441914.
- ^ Moss ML. The pathogenesis of premature cranial synostosis in man. Acta Anat (Basel) 1959: 37: 351-70.Moss, ML (1959). "The pathogenesis of premature cranial synostosis in man". Acta anatomica 37 (4): 351–70. doi:10.1159/000141479. PMID 14424622.
- ^ Kapp-Simon KA, Speltz ML, Cunningham ML, Patel PK, Tomita T. Neurodevelopment of children with single suture craniosynostosis: a review. Childs Nerv Syst 2007: 23: 269-81.Kapp-Simon, KA; Speltz, ML; Cunningham, ML; Patel, PK; Tomita, T (2007). "Neurodevelopment of children with single suture craniosynostosis: A review". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 23 (3): 269–81. doi:10.1007/s00381-006-0251-z. PMID 17186250.
- ^ Alderman BW, Fernbach SK, Greene C, Mangione EJ, Ferguson SW. Diagnostic practice and the estimated prevalence of craniosynostosis in Colorado. Arch Pediatr. Adolesc Med 1997: 151: 159-64.Alderman, BW; Fernbach, SK; Greene, C; Mangione, EJ; Ferguson, SW (1997). "Diagnostic practice and the estimated prevalence of craniosynostosis in Colorado". Archives of pediatrics & adolescent medicine 151 (2): 159–64. PMID 9041871.
- ^ a b Friede H, Alberius P, Lilja J, Lauritzen C. Trigonocephaly: clinical and cephalometric assessment of craniofacial morphology in operated and nontreated patients. Cleft Palate J 1990: 27: 362-7; discussion 68.Friede, H; Alberius, P; Lilja, J; Lauritzen, C (1990). "Trigonocephaly: Clinical and cephalometric assessment of craniofacial morphology in operated and nontreated patients". The Cleft palate journal 27 (4): 362–7; discussion 368. doi:10.1597/1545-1569(1990)027<0362:TCACAO>2.3.CO;2. PMID 2253382.
- ^ Genitori L, Cavalheiro S, Lena G, Dollo C, Choux M. Skull base in trigonocephaly. Pediatr Neurosurg 1991: 17: 175-81.Genitori, L; Cavalheiro, S; Lena, G; Dollo, C; Choux, M (1991). "Skull base in trigonocephaly". Pediatric neurosurgery 17 (4): 175–81. doi:10.1159/000120591. PMID 1822130.
- ^ a b c DiRocco C, Caldarelli M, Ceddia A, Iannelli A, Velardi F. [Craniostenosis. Analysis of 161 cases surgically treated during the first year of life]. Minerva Pediatr 1989: 41: 393-404.Dirocco, C; Caldarelli, M; Ceddia, A; Iannelli, A; Velardi, F (1989). "Craniostenosis. Analysis of 161 cases surgically treated during the first year of life". Minerva pediatrica 41 (8): 393–404. PMID 2601658.
- ^ a b c Dhellemmes P, Pellerin P, Lejeune JP, Lepoutre F. Surgical treatment of trigonocephaly. Experience with 30 cases. Childs Nerv Syst 1986: 2: 228-32.Dhellemmes, P; Pellerin, P; Lejeune, JP; Lepoutre, F (1986). "Surgical treatment of trigonocephaly. Experience with 30 cases". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2 (5): 228–32. PMID 3791279.
- ^ Boulet SL, Rasmussen SA, Honein MA. A population-based study of craniosynostosis in metropolitan Atlanta, 1989-2003.Am J Med Genet A. 2008:984-91 Boulet, SL; Rasmussen, SA; Honein, MA (2008). "A population-based study of craniosynostosis in metropolitan Atlanta, 1989-2003". American journal of medical genetics. Part A 146A (8): 984–91. doi:10.1002/ajmg.a.32208. PMID 18344207.
- ^ Kweldam CF, van der Vlugt JJ, van der Meulen JJNM. The incidence of craniosynostosis in the Netherlands, 1997-2007. J Plast Reconstr Aesthet Surg 2010 Sep 29.Kweldam, CF; Van Der Vlugt, JJ; Van Der Meulen, JJ (2010). "The incidence of craniosynostosis in the Netherlands, 1997-2007". Journal of plastic, reconstructive & aesthetic surgery : JPRAS 64 (5): 583–588. doi:10.1016/j.bjps.2010.08.026. PMID 20888312.
- ^ Frank M, Anderson MD, John L, Gwinn MD, John C, Todt MD. Trigonocephaly: Identity and surgical treatment. J Neurosurg 1962 Sep: 19: 723-30.Anderson, FM; Gwinn, JL; Todt, JC (1962). "Trigonocephaly. Identity and surgical treatment". Journal of neurosurgery 19 (9): 723–30. doi:10.3171/jns.1962.19.9.0723. PMID 13861226.
- ^ a b c Shillito J Jr., Matson DD. Craniosynostosis: a review of 519 surgical patients. Pediatrics 1968: 41: 829-53.Shillito Jr, J; Matson, DD (1968). "Craniosynostosis: A review of 519 surgical patients". Pediatrics 41 (4): 829–53. PMID 5643989.
- ^ a b c d e Anderson FM. Treatment of coronal and metopic synostosis: 107 cases. Neurosurgery 1981: 8: 143-9.Anderson, FM (1981). "Treatment of coronal and metopic synostosis: 107 cases". Neurosurgery 8 (2): 143–9. doi:10.1227/00006123-198102000-00001. PMID 7207779.
- ^ a b c d Collmann H, Sorensen N, Krauss J. Consensus: trigonocephaly. Childs Nerv Syst 1996: 12: 664-8.Collmann, H; Sörensen, N; Krauss, J (1996). "Consensus: Trigonocephaly". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 12 (11): 664–8. PMID 9118128.
- ^ Aryan HE, Jandial R, Ozgur BM, et al. Surgical correction of metopic synostosis. Childs Nerv Syst 2005: 21: 392-8.Aryan, HE; Jandial, R; Ozgur, BM; Hughes, SA; Meltzer, HS; Park, MS; Levy, ML (2005). "Surgical correction of metopic synostosis". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 21 (5): 392–8. doi:10.1007/s00381-004-1108-y. PMID 15714353.
- ^ Oi S, Matsumoto S. Trigonocephaly (metopic synostosis). Clinical, surgical and anatomical concepts. Childs Nerv Syst 1987: 3: 259-65.Oi, S; Matsumoto, S (1987). "Trigonocephaly (metopic synostosis). Clinical, surgical and anatomical concepts". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 3 (5): 259–65. PMID 3427566.
- ^ Sidoti EJ Jr., Marsh JL, Marty-Grames L, Noetzel MJ. Long-term studies of metopic synostosis: frequency of cognitive impairment and behavioural disturbances. Plast Reconstr Surg 1996: 97: 276-81.Sidoti Jr, EJ; Marsh, JL; Marty-Grames, L; Noetzel, MJ (1996). "Long-term studies of metopic synostosis: Frequency of cognitive impairment and behavioral disturbances". Plastic and reconstructive surgery 97 (2): 276–81. doi:10.1097/00006534-199602000-00002. PMID 8559809.
- ^ Kapp-Simon KA. Mental development and learning disorders in children with single suture craniosysnostosis. Cleft Palate Craniofac J 1998: 35: 197-203.Kapp-Simon, KA (1998). "Mental development and learning disorders in children with single suture craniosynostosis". The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association 35 (3): 197–203. doi:10.1597/1545-1569(1998)035<0197:MDALDI>2.3.CO;2. PMID 9603552.
- ^ a b Marchac D, Renier D, Broumand S. Timing of treatment for craniosynostosis and facio-craniosynostosis: a 20-year experience. Br J Plast Surg 1994: 47: 211-22.Marchac, D; Renier, D; Broumand, S (1994). "Timing of treatment for craniosynostosis and facio-craniosynostosis: A 20-year experience". British journal of plastic surgery 47 (4): 211–22. doi:10.1016/0007-1226(94)90001-9. PMID 8081607.
- ^ a b McCarthy JG, Epstein F, Sadove M, Grayson B, Zide B. Early surgery for craniofacial synostosis: a 8-year experience. Plast Reconstr Surg 1984; 73: 521-33.McCarthy, JG; Epstein, F; Sadove, M; Grayson, B; Zide, B; McCarthy, Joseph G. (1984). "Early surgery for craniofacial synostosis: An 8-year experience". Plastic and reconstructive surgery 73 (4): 521–33. doi:10.1097/00006534-198404000-00001. PMID 6709733.
- ^ a b Renier D, Lajeunie E, Arnaud E, Marchac D. Management of craniosynostoses. Childs Nerv Syst 2000: 16: 645-58.Renier, D; Lajeunie, E; Arnaud, E; Marchac, D (2000). "Management of craniosynostoses". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 16 (10–11): 645–58. PMID 11151714.
- ^ a b Whitaker LA, Bartlett SP, Schut L, Bruce D. Craniosynostosis: an analysis of the timing, treatment, and complications in 164 consecutive patients. Plast Reconstr Surg 1987: 80: 195-212.Whitaker, LA; Bartlett, SP; Schut, L; Bruce, D (1987). "Craniosynostosis: An analysis of the timing, treatment, and complications in 164 consecutive patients". Plastic and reconstructive surgery 80 (2): 195–212. doi:10.1097/00006534-198708000-00006. PMID 3602170.
- ^ Van der Meulen JJ, Nazir PRN, Mathijssen IMJ, Van Adrichem LNA, Ongkosuwito E, Stolk-Liefferink SAH, Vaandrager MJM. Bitemporal depressions after cranioplasty for trigonocephaly: a long-term evaluation of (supra) orbital growth in 92 patients. J Craniofac Surg 2008: 19(1): 72-9.Van Der Meulen, JJ; Nazir, PR; Mathijssen, IM; Van Adrichem, LN; Ongkosuwito, E; Stolk-Liefferink, SA; Vaandrager, MJ (2008). "Bitemporal depressions after cranioplasty for trigonocephaly: A long-term evaluation of (supra) orbital growth in 92 patients". The Journal of craniofacial surgery 19 (1): 72–9. doi:10.1097/scs.0b013e31815c8a68. PMID 18216668.
- ^ a b Marchac D. Radical forehead remodelling for craniostenosis. Plast Reconstr Surg 1978: 61: 823-35.Meling, TR; Due-Tønnessen, BJ; Helseth, E (2000). "Metotopic craniosynostoses". Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke 120 (26): 3147–50. PMID 11109361.
- ^ Marchac D, Renier D, Jones BM. Experience with the “floating forehead”. British Journal of Plastic Surgery 1988: 41: l-15.Marchac, D; Renier, D; Jones, BM (1988). "Experience with the "floating forehead"". British journal of plastic surgery 41 (1): 1–15. doi:10.1016/0007-1226(88)90137-3. PMID 3345401.
- ^ Hoffman HJ. Mohr G. Lateral canthal advancement of the supraorbital margin. A new corrective techmique in the treatment of coronal synostosis. J Neurosurg 1976: 45: 376-81.Hoffman, HJ; Mohr, G (1976). "Lateral canthal advancement of the supraorbital margin. A new corrective technique in the treatment of coronal synostosis". Journal of neurosurgery 45 (4): 376–81. doi:10.3171/jns.1976.45.4.0376. PMID 956873.
- ^ Delashaw JB, Persing JA, Park TS, Jane JA. Surgical approaches for the correction of metopic synostosis. Neurosurgery 1986: 19: 228-34.Delashaw, JB; Persing, JA; Park, TS; Jane, JA (1986). "Surgical approaches for the correction of metopic synostosis". Neurosurgery 19 (2): 228–34. doi:10.1227/00006123-198608000-00008. PMID 3748350.
- ^ Takuya A, Hideaki I, Shigehiko K. Treatment of Craniosynostosis by Distraction Osteogenesis. Pediatr Neurosurg 2006: 42: 288–292.Akai, T; Iizuka, H; Kawakami, S (2006). "Treatment of craniosynostosis by distraction osteogenesis". Pediatric neurosurgery 42 (5): 288–92. doi:10.1159/000094064. PMID 16902340.
- ^ a b DiRocco C, Velardi F, Ferrario A, Marchese E. Metopic synostosis: in favour of a "simplified" surgical treatment. Child's Nerv Syst 1996: 12: 654-663.Di Rocco, C; Velardi, F; Ferrario, A; Marchese, E (1996). "Metopic synostosis: In favour of a "simplified" surgical treatment". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 12 (11): 654–63. PMID 9118127.
- ^ Galassi E, Giulioni M, Acciarri N, Cavina C, Pistorale T. Marchac procedure in the early treatment of metopic and coronal synostoses. Presented at the Consensus Conference on Craniosynostoses, Rome 1995.
- ^ Lauritzen CG, Davis C, Ivarsson A, Sanger C, Hewitt TD. The evolving role of springs in craniofacial surgery: the first 100 clinical cases. Plast Reconstr Surg 2008: 121: 545-54.Lauritzen, CG; Davis, C; Ivarsson, A; Sanger, C; Hewitt, TD (2008). "The evolving role of springs in craniofacial surgery: The first 100 clinical cases". Plastic and reconstructive surgery 121 (2): 545–54. doi:10.1097/01.prs.0000297638.76602.de. PMID 18300975.
- ^ Maltese G, Tanrow P, Lauritze CG. Spring-asssisted correction of hypotelorism in metopic synostosis. Plast Reconstr Surg 2007: 119: 977-84.Maltese, G; Tarnow, P; Lauritzen, CG (2007). "Spring-assisted correction of hypotelorism in metopic synostosis". Plastic and reconstructive surgery 119 (3): 977–84. doi:10.1097/01.prs.0000252276.46113.ee. PMID 17312504.
- ^ Davis C, Lauritzen CG. Frontobasal suture distraction corrects hypotelorism in metopic synostosis. J Craniofac Surg 2009: 20: 121-4.Davis, C; Lauritzen, CG (2009). "Frontobasal suture distraction corrects hypotelorism in metopic synostosis". The Journal of craniofacial surgery 20 (1): 121–4. doi:10.1097/SCS.0b013e318190e25d. PMID 19165007.
- ^ Fearon JA, Kolar JC, Munro IR. Trigonocephaly-associated hypotelorism: is treatment necessary? Plast Reconstr Surg 1996: 97: 503-9; discussion 10-11.Fearon, JA; Kolar, JC; Munro, IR (1996). "Trigonocephaly-associated hypotelorism: Is treatment necessary?". Plastic and reconstructive surgery 97 (3): 503–9; discussion 510–11. doi:10.1097/00006534-199603000-00001. PMID 8596780.
- ^ Barone CM, Jimenez DF. Endoscopic craniectomy for early correction of craniosynostosis. Plast Reconstr Surg 1999: 104(7): 1965-73; discussion 1974-5.Barone, CM; Jimenez, DF (1999). "Endoscopic craniectomy for early correction of craniosynostosis". Plastic and reconstructive surgery 104 (7): 1965–73; discussion 1974–5. doi:10.1097/00006534-199912000-00003. PMID 11149758.
- ^ Hinojosa J, Esparza J, Garcia-RecueroI, Romance A. [Endoscopically assisted fronto-orbitary correction in trigonocephaly]. Cir Pediatr 2007: 20: 33-8.Hinojosa, J; Esparza, J; García-Recuero, I; Romance, A (2007). "Endoscopically assisted fronto-orbitary correction in trigonocephaly". Cirugia pediatrica : organo oficial de la Sociedad Espanola de Cirugia Pediatrica 20 (1): 33–8. PMID 17489491.
- ^ Murad GJ, Clayman M, Seagle MB, et al. Endoscopic-assisted repair of craniosynostosis. Neurosurg Focus 2005: 19: E6.Murad, GJ; Clayman, M; Seagle, MB; White, S; Perkins, LA; Pincus, DW (2005). "Endoscopic-assisted repair of craniosynostosis". Neurosurgical focus 19 (6): E6. PMID 16398483.
- ^ Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis. J Neurosurg 1998: 88: 77-81.Jimenez, DF; Barone, CM (1998). "Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis". Journal of neurosurgery 88 (1): 77–81. doi:10.3171/jns.1998.88.1.0077. PMID 9420076.
- ^ Hinojosa J, Esparza J, Munoz MJ. Endoscopic-assisted osteotomies for the treatment of craniosynostosis. Childs Nerv Syst 2007: 23: 1421-30.Hinojosa, J; Esparza, J; Muñoz, MJ (2007). "Endoscopic-assisted osteotomies for the treatment of craniosynostosis". Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 23 (12): 1421–30. doi:10.1007/s00381-007-0473-8. PMID 17899127.
- ^ a b Greenberg BM, Schneider SJ. Trigonocephaly: surgical considerations and long term evaluation. J Craniofac Surg 2006: 17: 528-35.Greenberg, BM; Schneider, SJ (2006). "Trigonocephaly: Surgical considerations and long term evaluation". The Journal of craniofacial surgery 17 (3): 528–35. PMID 16770193.
- ^ Cohen SR, Maher H, Wagner JD, et al. Metopic synostosis: evaluation of aesthetic results. Plast Reconstr Surg 1994: 94:759-67.Cohen, SR; Maher, H; Wagner, JD; Dauser, RC; Newman, MH; Muraszko, KM (1994). "Metopic synostosis: Evaluation of aesthetic results". Plastic and reconstructive surgery 94 (6): 759–67. doi:10.1097/00006534-199411000-00002. PMID 7972420.
- ^ Posnick JC, Lin KY, Chen P, Armstrong D. Metopic synostosis: quantitative assessment of presenting deformity and surgical results based on CT scans. Plast Reconstr Surg 1994: 93: 16-24.Posnick, JC; Lin, KY; Chen, P; Armstrong, D (1994). "Metopic synostosis: Quantitative assessment of presenting deformity and surgical results based on CT scans". Plastic and reconstructive surgery 93 (1): 16–24. doi:10.1097/00006534-199401000-00003. PMID 8278471.
Categories:- Congenital disorders of musculoskeletal system
Wikimedia Foundation. 2010.