- HIV test
-
 Randall L. Tobias, former U.S. Global AIDS Coordinator, being publicly tested for HIV in Ethiopia in an effort to reduce the stigma of being tested.[1]
Randall L. Tobias, former U.S. Global AIDS Coordinator, being publicly tested for HIV in Ethiopia in an effort to reduce the stigma of being tested.[1]
HIV tests are used to detect the presence of the human immunodeficiency virus (HIV), the virus that causes acquired immunodeficiency syndrome (AIDS), in serum, saliva, or urine. Such tests may detect antibodies, antigens, or RNA.
Contents
Terminology
The window period is the time from infection until a test can detect any change. The average window period with HIV-1 antibody tests is 25 days for subtype B. Antigen testing cuts the window period to approximately 16 days and NAT (Nucleic Acid Testing) further reduces this period to 12 days.[2]
Performance of medical tests is often described in terms of:
- sensitivity: The percentage of the results that will be positive when HIV is present
- specificity: The percentage of the results that will be negative when HIV is not present.
All diagnostic tests have limitations, and sometimes their use may produce erroneous or questionable results.
- False positive: The test incorrectly indicates that HIV is present in a non-infected person.
- False negative: The test incorrectly indicates that HIV is absent in an infected person.
Nonspecific reactions, hypergammaglobulinemia, or the presence of antibodies directed to other infectious agents that may be antigenically similar to HIV can produce false positive results. Autoimmune diseases, such as systemic lupus erythematosus, have also rarely caused false positive results. Most false negative results are due to the window period.
Principles
Screening donor blood and cellular products
Tests selected to screen donor blood and tissue must provide a high degree of confidence that HIV will be detected if present (that is, a high sensitivity is required). A combination of antibody, antigen and nucleic acid tests are used by blood banks in Western countries. The World Health Organization estimated that, as of 2000[update], inadequate blood screening had resulted in 1 million new HIV infections worldwide.[citation needed]
In the USA, since 1985, all blood donations are screened with an ELISA test for HIV-1 and HIV-2, as well as a nucleic acid test.[citation needed] These diagnostic tests are combined with careful donor selection. As of 2001[update], the risk of transfusion-acquired HIV in the U.S. was approximately one in 2.5 million for each transfusion.[3]
Diagnosis of HIV infection
Tests used for the diagnosis of HIV infection in a particular person require a high degree of both sensitivity and specificity. In the United States, this is achieved using an algorithm combining two tests for HIV antibodies. If antibodies are detected by an initial test based on the ELISA method, then a second test using the Western blot procedure determines the size of the antigens in the test kit binding to the antibodies. The combination of these two methods is highly accurate (see below).
Human rights
The UNAIDS/WHO policy statement on HIV Testing states that conditions under which people undergo HIV testing must be anchored in a human rights approach that pays due respect to ethical principles.[4] According to these principles, the conduct of HIV testing of individuals must be
- Confidential;
- Accompanied by counseling (for those who test positive);
- Conducted with the informed consent of the person being tested.
Confidentiality
Considerable controversy exists over the ethical obligations of health care providers to inform the sexual partners of individuals infected with HIV that they are at risk of contracting the virus.[5] Some legal jurisdictions permit such disclosure, while others do not. More state funded testing sites are now using confidential forms of testing. This allows for monitoring of infected individuals easily, compared to anonymous testing that has a number attached to the positive test results. Controversy exists over privacy issues.
Anonymous testing
Testing that has only a number attached to the specimen that will be delivered for testing. Items that are confirmed positive will not have the HIV infected individual's name attached to the specimen. Sites that offer this service advertise this testing option.[clarification needed]
Routine testing recommendation
In the United States, one emerging standard of care is to screen all patients for HIV in all health care settings.[6] In 2006, the Centers for Disease Control announced an initiative for voluntary, routine testing of all Americans aged 13–64 during health care encounters. An estimated 25% of infected individuals were unaware of their status; If successful the effort was expected to reduce new infections by 30% per year.[7] The CDC recommends elimination of requirements for written consent or extensive pre-test counseling as barriers to widespread routine testing.[7]
Antibody tests
HIV antibody tests are specifically designed for routine diagnostic testing of adults; these tests are inexpensive and extremely accurate.
Window period
Antibody tests may give false negative (no antibodies were detected despite the presence of HIV) results during the window period, an interval of three weeks to six months between the time of HIV infection and the production of measurable antibodies to HIV seroconversion. Most people develop detectable antibodies approximately 30 days after infection, although some seroconvert later. The vast majority of people (97%) have detectable antibodies by three months after HIV infection; a six-month window is extremely rare with modern antibody testing.[8] During the window period, an infected person can transmit HIV to others although their HIV infection may not be detectable with an antibody test. Antiretroviral therapy during the window period can delay the formation of antibodies and extend the window period beyond 12 months.[9] This was not the case with patients that underwent treatment with post exposure prophylaxis (PEP). Those patients must take ELISA tests at various intervals after the usual 28 day course of treatment, sometimes extending outside of the conservative window period of 6 months. Antibody tests may also yield false negative results in patients with X-linked agammaglobulinemia; other diagnostic tests should be used in such patients.
Three instances of delayed HIV seroconversion occurring in health-care workers have been reported;[10] in these instances, the health-care workers[11] tested negative for HIV antibodies greater than 6 months postexposure but were seropositive within 12 months after the exposure.[12] DNA sequencing confirmed the source of infection in one instance. Two of the delayed seroconversions were associated with simultaneous exposure to hepatitis C virus (HCV). In one case, co-infection was associated with a rapidly fatal HCV disease course; however, it is not known whether HCV directly influences the risk for or course of HIV infection or is a marker for other exposure-related factors.
ELISA
The enzyme-linked immunosorbent assay (ELISA), or enzyme immunoassay (EIA), was the first screening test commonly employed for HIV. It has a high sensitivity.
In an ELISA test, a person's serum is diluted 400-fold and applied to a plate to which HIV antigens have been attached. If antibodies to HIV are present in the serum, they may bind to these HIV antigens. The plate is then washed to remove all other components of the serum. A specially prepared "secondary antibody" — an antibody that binds to human antibodies — is then applied to the plate, followed by another wash. This secondary antibody is chemically linked in advance to an enzyme. Thus the plate will contain enzyme in proportion to the amount of secondary antibody bound to the plate. A substrate for the enzyme is applied, and catalysis by the enzyme leads to a change in color or fluorescence. ELISA results are reported as a number; the most controversial aspect of this test is determining the "cut-off" point between a positive and negative result.
Western blot
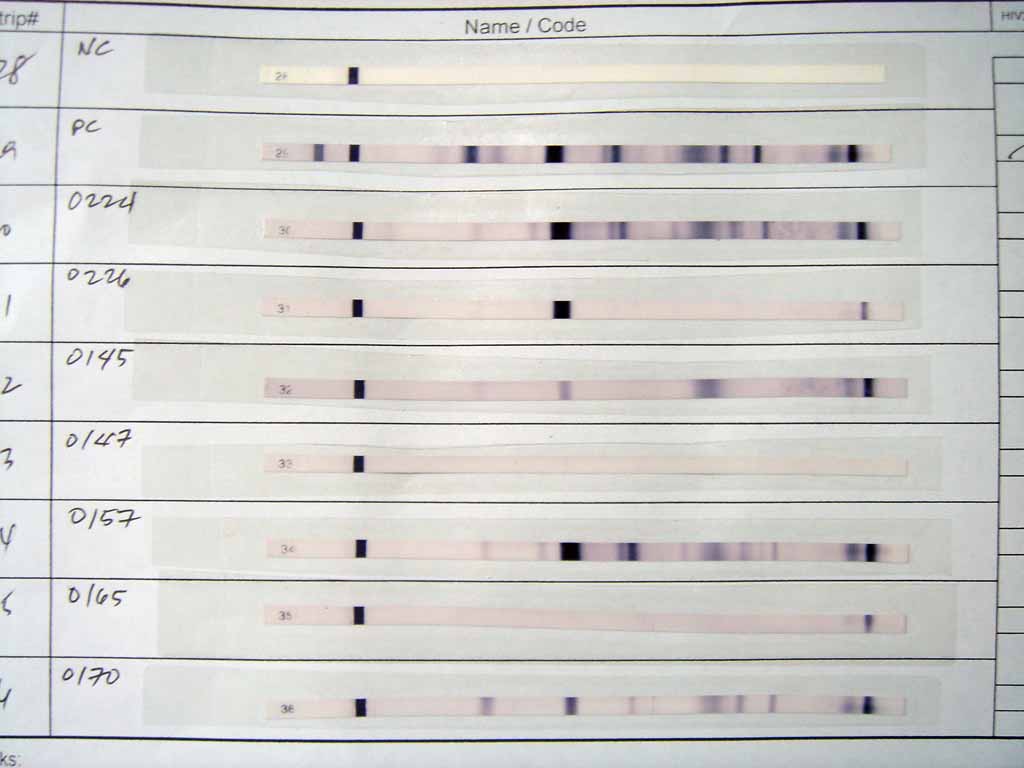
 Western blot test results. The first two strips are a negative and a positive control, respectively. The others are actual tests.
Western blot test results. The first two strips are a negative and a positive control, respectively. The others are actual tests.Like the ELISA procedure, the western blot is an antibody detection test. However, unlike the ELISA method, the viral proteins are separated first and immobilized. In subsequent steps, the binding of serum antibodies to specific HIV proteins is visualized.
Specifically, cells that may be HIV-infected are opened and the proteins within are placed into a slab of gel, to which an electrical current is applied. Different proteins will move with different velocities in this field, depending on their size, while their electrical charge is leveled by a surfactant called sodium lauryl sulfate. Some commercially prepared Western blot test kits contain the HIV proteins already on a cellulose acetate strip. Once the proteins are well-separated, they are transferred to a membrane and the procedure continues similar to an ELISA: the person's diluted serum is applied to the membrane and antibodies in the serum may attach to some of the HIV proteins. Antibodies that do not attach are washed away, and enzyme-linked antibodies with the capability to attach to the person's antibodies determine to which HIV proteins the person has antibodies.
There are no universal criteria for interpreting the western blot test: The number of viral bands that must be present may vary. If no viral bands are detected, the result is negative. If at least one viral band for each of the GAG, POL, and ENV gene-product groups are present, the result is positive. The three-gene-product approach to western blot interpretation has not been adopted for public health or clinical practice. Tests in which less than the required number of viral bands are detected are reported as indeterminate: a person who has an indeterminate result should be retested, as later tests may be more conclusive. Almost all HIV-infected persons with indeterminate western blot results will develop a positive result when tested in one month; persistently indeterminate results over a period of six months suggests the results are not due to HIV infection. In a generally healthy low-risk population, indeterminate results on western blot occur on the order of 1 in 5,000 patients.[13]:However for those individuals that have had high-risk exposures to individuals where HIV-2 is most prevalent, Western Africa, an inconclusive western blot test may prove infection with HIV-2.[14]
The HIV proteins used in western blotting can be produced by recombinant DNA in a technique called recombinant immunoblot assay (RIBA).[15]
Rapid or point-of-care tests
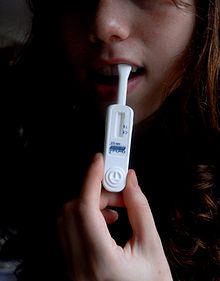 A woman demonstrates the use of the OraQuick rapid HIV test
A woman demonstrates the use of the OraQuick rapid HIV testRapid antibody tests are qualitative immunoassays intended for use as a point-of-care test to aid in the diagnosis of HIV infection. These tests should be used in conjunction with the clinical status, history, and risk factors of the person being tested. The positive predictive value of Rapid Antibody Tests in low-risk populations has not been evaluated. These tests should be used in appropriate multi-test algorithms designed for statistical validation of rapid HIV test results.
If no antibodies to HIV are detected, this does not mean the person has not been infected with HIV. It may take several months after HIV infection for the antibody response to reach detectable levels, during which time rapid testing for antibodies to HIV will not be indicative of true infection status. For most people, HIV antibodies reach a detectable level after two to six weeks.
Although these tests have high specificity, false positives do occur. Any positive test result should be confirmed by a lab using the western blot.
Home Access Express HIV-1 Test is the only FDA-approved home test: the patient collects a few blood drops from a fingerstick, and mails the sample to a laboratory; results and counseling are obtained over the phone. All results are anonymous and confirmed before they are released.
OraQuick is an antibody test that provides results in 20 minutes. The blood, plasma or oral fluid is mixed in a vial with developing solution, and the results are read from a sticklike testing device. Usually detects HIV 1 and HIV 2.
Orasure is an HIV test that uses mucosal transudate from the tissues of cheeks and gums. It is an antibody test that first employs ELISA, then western blot.
Uni-Gold is a rapid HIV antibody test that provides results in 10–12 minutes. A drop of blood is placed on the device with developing solution. Uni-Gold is only FDA approved to test for HIV 1.
Clearview Complete HIV 1/2 and Clearview HIV 1/2 Stat-Pak are rapid tests for the detection of HIV 1 and HIV 2 antibodies in blood, serum, or plasma samples. Results are provided within 15 minutes.
There is also a urine test; it employs both the ELISA and the western blot techniques.
iDiagnostics Rapid HIV Test is, according only to their website, a non-FDA-approved home test. The company sells a blood test and a urine test produced by InTec PRODUCTS, INC. Similar to a home pregnancy test the patient collects a drop of blood/urine and drops the sample onto a cassette. Results are read visually in 15 minutes.[16][unreliable source?] The accuracy of this test has not been confirmed by the FDA, and it is not authorized for sale in the United States.[17]
The INSTI HIV-1/HIV-2* Rapid Antibody Test is a rapid in vitro qualitative test for the detection of antibodies to Human Immunodeficiency Virus Type 1 in human whole blood, serum or plasma. The test is intended for use by trained personnel in medical facilities, clinical laboratories, emergency care situations, and physicians' offices as a screening assay capable of providing test results in less than 60 seconds. The assay is packaged as a kit containing INSTI Membrane Units, Sample Diluent, Color Developer and Clarifying Solution, and is available in point-of-care use packaging, or packaging suitable for laboratory use.[18]
Reveal HIV is a rapid in vitro qualitative test for the detection of antibodies to HIV in whole blood, serum or plasma. Reveal is among the fastest rapid HIV test available and it detects signs of early infection better than some other rapid tests.[19] Reveal HIV is approved in Canada, the United States, Europe, Africa, Asia, and South America.[20]
Interpreting antibody tests
ELISA testing alone cannot be used to diagnose HIV, even if the test suggests a high probability that antibody to HIV-1 is present. In the United States, such ELISA results are not reported as "positive" unless confirmed by a Western Blot.
The ELISA antibody tests were developed to provide a high level of confidence that donated blood was NOT infected with HIV. It is therefore not possible to conclude that blood rejected for transfusion because of a positive ELISA antibody test is in fact infected with HIV. Sometimes, retesting the donor in several months will produce a negative ELISA antibody test. This is why a confirmatory Western Blot is always used before reporting a "positive" HIV test result.
Rare false positive results due to factors unrelated to HIV exposure are found more often with the ELISA test than with the Western Blot. False positives may be associated with medical conditions such as recent acute illnesses and allergies. A rash of false positive tests in the fall of 1991 was initially blamed on the influenza vaccines used during that flu season, but further investigation traced the cross-reactivity to several relatively non-specific test kits.[21] A false positive result does not indicate a condition of significant risk to health. When the ELISA test is combined with Western Blot, the rate of false positives is extremely low, and diagnostic accuracy is very high (see below).
- HIV antibody tests are highly sensitive, meaning they react preferentially with HIV antibodies, but not all positive or inconclusive HIV ELISA tests mean the person is infected by HIV. Risk history, and clinical judgement should be included in the assessment, and a confirmation test (Western blot) should be administered. An individual with an inconclusive test should be re-tested at a later date.
Accuracy of HIV testing
Modern HIV testing is highly accurate. The evidence regarding the risks and benefits of HIV screening was reviewed in July 2005 by the U.S. Preventive Services Task Force.[22] The authors concluded that:
...the use of repeatedly reactive enzyme immunoassay followed by confirmatory Western blot or immunofluorescent assay remains the standard method for diagnosing HIV-1 infection. A large study of HIV testing in 752 U.S. laboratories reported a sensitivity of 99.7% and specificity of 98.5% for enzyme immunoassay, and studies in U.S. blood donors reported specificities of 99.8% and greater than 99.99%. With confirmatory Western blot, the chance of a false-positive identification in a low-prevalence setting is about 1 in 250 000 (95% CI, 1 in 173 000 to 1 in 379 000).
The specificity rate given here for the inexpensive enzyme immunoassay screening tests indicates that, in 1,000 HIV test results, about 15 of these results will be a false positive. Confirming the test result (i.e., by repeating the test, if this option is available) could reduce the ultimate likelihood of a false positive to about 1 result in 250,000 tests given. The sensitivity rating, likewise, indicates that, in 1,000 negative HIV test results, 3 will actually be a false negative result. However, based upon the HIV prevalence rates at most testing centers within the United States, the negative predictive value of these tests is extremely high, meaning that a negative test result will be correct more than 9,997 times in 10,000 (99.97% of the time). The very high negative predictive value of these tests is why the CDC recommends that a negative test result be considered conclusive evidence that an individual does not have HIV.
Of course, the actual numbers vary depending on the testing population. This is because interpreting of the results of any medical test (assuming no test is 100% accurate) depends upon the initial degree of belief, or the prior probability that an individual has, or does not have a disease. Generally the prior probability is estimated using the prevalence of a disease within a population or at a given testing location. The positive predictive value and negative predictive value of all tests, including HIV tests, take into account the prior probability of having a disease along with the accuracy of the testing method to determine a new degree of belief that an individual has or does not have a disease (also known as the posterior probability). The chance that a positive test accurately indicates an HIV infection increases as the prevalence or rate of HIV infection increases in the population. Conversely, the negative predictive value will decrease as the HIV prevalence rises. Thus a positive test in a high-risk population, such as people who frequently engage in unprotected anal intercourse with unknown partners, is more likely to correctly represent HIV infection than a positive test in a very low-risk population, such as unpaid blood donors.
Many studies have confirmed the accuracy of current methods of HIV testing in the United States, reporting false-positive rates of 0.0004 to 0.0007 and false-negative rates of 0.003 in the general population.[23][24][25][26][27][28][29][30]
Antigen tests
The p24 antigen test detects the presence of the p24 protein of HIV (also known as CA), the capsid protein of the virus. Monoclonal antibodies specific to the p24 protein are mixed with the person's blood. Any p24 protein in the person's blood will stick to the monoclonal antibody and an enzyme-linked antibody to the monoclonal antibodies to p24 causes a color change if p24 was present in the sample.
This test is no longer used routinely in the US [2] or the EU [3] to screen blood donations since the objective was to reduce the risk of false negatives in the window period. Nucleic acid testing (NAT) is more effective for this purpose, and p24 antigen testing is no longer indicated if a NAT test is performed. The p24 antigen test is not useful for general diagnostics, as it has very low sensitivity and only works during a certain time period after infection before the body produces antibodies to the p24 protein.
Nucleic acid-based tests (NAT)
Nucleic-acid-based tests amplify and detect one or more of several target sequences located in specific HIV genes, such as HIV-I GAG, HIV-II GAG, HIV-env, or the HIV-pol.[31][32] Since these tests are relatively expensive, the blood is screened by first pooling some 8-24 samples and testing these together; if the pool tests positive, each sample is retested individually. Although this results in a dramatic decrease in cost, the dilution of the virus in the pooled samples decreases the effective sensitivity of the test, lengthening the window period by 4 days (assuming a 20-fold dilution, ~20hr virus doubling time, detection limit 50 copies/ml, making limit of detection 1,000 copies/ml). Since 2001, donated blood in the United States has been screened with nucleic-acid-based tests, shortening the window period between infection and detectability of disease to a median of 17 days (95% CI, 13-28 Days, assumes pooling of samples).[33] A different version of this test is intended for use in conjunction with clinical presentation and other laboratory markers of disease progress for the management of HIV-1-infected patients.
In the RT-PCR test, viral RNA is extracted from the patient's plasma and is treated with reverse transcriptase (RT) to convert the viral RNA into cDNA. The polymerase chain reaction (PCR) process is then applied, using two primers unique to the virus's genome. After PCR amplification is complete, the resulting DNA products are hybridized to specific oligonucleotides bound to the vessel wall, and are then made visible with a probe bound to an enzyme. The amount of virus in the sample can be quantified with sufficient accuracy to detect threefold changes.
In the Quantiplex bDNA or branched DNA test, plasma is centrifugated to concentrate the virus, which is then opened to release its RNA. Special oligonucleotides that bind to viral RNA and to certain oligonucleotides bound to the wall of the vessel are added. In this way, viral RNA is fastened to the wall. Then new oligonucleotides that bind at several locations to this RNA are added, and other oligonucelotides that bind at several locations to those oligonucleotides. This is done to amplify the signal. Finally, oligonucleotides that bind to the last set of oligonucleotides and that are bound to an enzyme are added; the enzyme action causes a color reaction, which allows quantification of the viral RNA in the original sample. Monitoring the effects of antiretroviral therapy by serial measurements of plasma HIV-1 RNA with this test has been validated for patients with viral loads greater than 25,000 copies per milliliter.[34]
Further information: Viral load testingOther tests used in HIV treatment
The CD4 T-cell count is not an HIV test, but rather a procedure where the number of CD4 T-cells in the blood is determined.
A CD4 count does not check for the presence of HIV. It is used to monitor immune system function in HIV-positive people. Declining CD4 T-cell counts are considered to be a marker of progression of HIV infection. In HIV-positive people, AIDS is officially diagnosed when the count drops below 200 cells/μL or when certain opportunistic infections occur. This use of a CD4 count as an AIDS criterion was introduced in 1992; the value of 200 was chosen because it corresponded with a greatly increased likelihood of opportunistic infection. Lower CD4 counts in people with AIDS are indicators that prophylaxis against certain types of opportunistic infections should be instituted.
Low CD4 T-cell counts are associated with a variety of conditions, including many viral infections, bacterial infections, parasitic infections, sepsis, tuberculosis, coccidioidomycosis, burns, trauma, intravenous injections of foreign proteins, malnutrition, over-exercising, pregnancy, normal daily variation, psychological stress, and social isolation.[citation needed]
This test is also used occasionally to estimate immune system function for people whose CD4 T cells are impaired for reasons other than HIV infection, which include several blood diseases, several genetic disorders, and the side effects of many chemotherapy drugs.
In general, the lower the number of T cells the lower the immune system's function will be. Normal CD4 counts are between 500 and 1500 CD4+ T cells/microliter, and the counts may fluctuate in healthy people, depending on recent infection status, nutrition, exercise, and other factors. Women tend to have somewhat lower counts than men.
Criticisms of HIV tests
As a result of an increase in false positive rates with rapid oral HIV testing in 2005, New York City's Department of Health and Mental Hygiene added the option of testing finger-stick whole blood after any reactive result, before using a Western Blot test to confirm the positive result. Following a further increase of false positives in NYC DOHMH STD Clinics during the end of 2007 and beginning of 2008, their clinics opted to forgo further oral screenings, and instead reinsituted testing using finger-stick whole blood.[35] Despite the increase in false positives in NYC DOHMH, the CDC still continues to support the use of noninvasive oral fluid specimens due to their popularity in health clinics and convenience of use. The director of the HIV control program for public health at Seattle King county, reported OraQuick failed to spot at least 8 percent of 133 people found to be infected with a comparable diagnostic test.[36] Strategies implemented to determine quality control and false positive rates were implemented. It is to be understood that any reactive OraQuick test result is a preliminary positive result and will always require a confirmatory test, regardless of the mean of testing (venipuncture whole blood, fingerstick whole blood or oral mucosal transudate fluid) [37] Several other testing sites who did not experience a spike in false positive rates continue to use OraSure's OraQuick HIV Anti-body Testing.[38][39]
HIV tests have been criticized by AIDS denialists (a fringe group that believes that HIV either does not exist or is harmless). The accuracy of serologic testing has been verified by isolation and culture of HIV and by detection of HIV RNA by PCR, which are widely accepted "gold standards" in microbiology.[25][26] While AIDS denialists focus on individual components of HIV testing, the combination of ELISA and Western blot used for the diagnosis of HIV is remarkably accurate, with very low false-positive and -negative rates as described above. The views of AIDS denialists are based on highly selective analysis of mostly outdated scientific papers; there is broad scientific consensus that HIV is the cause of AIDS.[40][41][42]
Fraudulent testing
There have been a number of cases of fraudulent tests being sold via mail order or the Internet to the general public. In 1997, a California man was indicted on mail fraud and wire charges for selling supposed home test kits. In 2004, the US Federal Trade Commission asked Federal Express and US Customs to confiscate shipments of the Discreet home HIV test kits, produced by Gregory Stephen Wong of Vancouver, BC. In February 2005, the US FDA issued a warning against using the rapid HIV test kits and other home use kits marketed by Globus Media of Montreal, Canada.
References
- ^ "Blacklist of English teachers suspected of having AIDS pursued." This image of Randall L. Tobias is used in a Korean news article suggesting that foreign English teachers residing in Korea are at risk for AIDS. Accessed 16 Feb., 2010.
- ^ FDA Approves First Nucleic Acid Test (NAT) Systems to Screen Plasma for Human Immunodeficiency Virus (HIV) and Hepatitis C Virus (HCV)[dead link], (archived copy)
- ^ Adverse reactions associated with blood transfusion. From the Puget Sound Blood Center. Accessed 5 Oct 2006.
- ^ UNAIDS/WHO policy statement on HIV Testing (PDF), accessed 5 Oct 2006.
- ^ JM Appel (June 2006). "Must My Doctor Tell My Partner? Rethinking Confidentiality in the HIV Era". Medicine and Health Rhode Island 89 (6): 223–4. PMID 16875013.
- ^ Armstrong WS, Taege AJ (April 2007). "HIV screening for all: the new standard of care". Cleve Clin J Med 74 (4): 297–301. doi:10.3949/ccjm.74.4.297. PMID 17438679.
- ^ a b CDC fact sheet
- ^ Skip CDC - HIV Testing Basics for Consumers, from the Seattle and King County Public Health Department. Accessed 21 Feb 2007.
- ^ C B Hare, B L Pappalardo, M P Busch, B Phelps, S S Alexander, C Ramstead, J A Levy, F M Hecht (2004). "Negative HIV antibody test results among individuals treated with antiretroviral therapy (ART) during acute/early infection". The XV International AIDS Conference. pp. Abstract no. MoPeB3107. http://www.iasociety.org/ejias-search/show.asp?abstract_id=2172342&iConferenceID=2004.
- ^ Ridzon R, Gallagher K, Ciesielski C et al. (1997). "Simultaneous transmission of human immunodeficiency virus and hepatitis C virus from a needle-stick injury". N Engl J Med 336 (13): 919–22. doi:10.1056/NEJM199703273361304. PMID 9070472.
- ^ HIV Seroconversion in HEALTH-CARE WORKERS
- ^ J.L. Gerberding, San Francisco General Hospital, unpublished data, May 1997
- ^ Bartlett, JG. Serologic tests for the diagnosis of HIV infection, in UpToDate. Accessed 5 October 2006.
- ^ Scand J Infect Dis. 1992;24(4):419-21. Accessed 23 September 2008.
- ^ Mas, A.; Soriano, V.; Gutiérrez, M.; Fumanal, F.; Alonso, A.; González-Lahoz, J. (1997). "Reliability of a new recombinant immunoblot assay (RIBA HIV-1/HIV-2 SIA) as a supplemental (confirmatory) test for HIV-1 and HIV-2 infections". Transfusion science 18 (1): 63–69. PMID 10174294.
- ^ http://www.idiagnosticsco.com/index.php/about/
- ^ http://www.fda.gov/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/ComplianceActivities/Enforcement/UntitledLetters/ucm091993.htm
- ^ http://www.biolytical.com/ourtechnology.html
- ^ Owen SM, Yang C, Spira T, et al. (May 2008). "Alternative algorithms for human immunodeficiency virus infection diagnosis using tests that are licensed in the United States". J. Clin. Microbiol. 46 (5): 1588–95. doi:10.1128/JCM.02196-07. PMC 2395119. PMID 18322061. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2395119.
- ^ http://www.medmira.com
- ^ Simonsen L, Buffington J, (June 1995). "Multiple false reactions in viral antibody screening assays after influenza vaccination". Am J Epidemiol 141 (11): 1089–96. PMID 7539579.
- ^ Chou R, Huffman LH, Fu R, Smits AK, Korthuis PT (July 2005). "Screening for HIV: a review of the evidence for the U.S. Preventive Services Task Force". Ann. Intern. Med. 143 (1): 55–73. PMID 15998755. http://www.annals.org/cgi/content/full/143/1/55.
- ^ Kleinman S, Busch M, Hall L, Thomson R, Glynn S, Gallahan D, Ownby H, Williams A (1998). "False-positive HIV-1 test results in a low-risk screening setting of voluntary blood donation. Retrovirus Epidemiology Donor Study". JAMA 280 (12): 1080–5. doi:10.1001/jama.280.12.1080. PMID 9757856.
- ^ Burke D, Brundage J, Redfield R, Damato J, Schable C, Putman P, Visintine R, Kim H (1988). "Measurement of the false positive rate in a screening program for human immunodeficiency virus infections". N Engl J Med 319 (15): 961–4. doi:10.1056/NEJM198810133191501. PMID 3419477.
- ^ a b MacDonald K, Jackson J, Bowman R, Polesky H, Rhame F, Balfour H, Osterholm M (1989). "Performance characteristics of serologic tests for human immunodeficiency virus type 1 (HIV-1) antibody among Minnesota blood donors. Public health and clinical implications". Ann Intern Med 110 (8): 617–21. PMID 2648922.
- ^ a b Busch M, Eble B, Khayam-Bashi H, Heilbron D, Murphy E, Kwok S, Sninsky J, Perkins H, Vyas G (1991). "Evaluation of screened blood donations for human immunodeficiency virus type 1 infection by culture and DNA amplification of pooled cells". N Engl J Med 325 (1): 1–5. doi:10.1056/NEJM199107043250101. PMID 2046708.
- ^ Van de Perre P, Simonon A, Msellati P, Hitimana D, Vaira D, Bazubagira A, Van Goethem C, Stevens A, Karita E, Sondag-Thull D (1991). "Postnatal transmission of human immunodeficiency virus type 1 from mother to infant. A prospective cohort study in Kigali, Rwanda". N Engl J Med 325 (9): 593–8. doi:10.1056/NEJM199108293250901. PMID 1812850.
- ^ Update: serologic testing for HIV-1 antibody--United States, 1988 and 1989. MMWR Morb Mortal Wkly Rep 1990; 39:380.
- ^ Urnovitz H, Sturge J, Gottfried T (1997). "Increased sensitivity of HIV-1 antibody detection". Nat Med 3 (11): 1258. doi:10.1038/nm1197-1258. PMID 9359701.
- ^ Farzadegan H, Vlahov D, Solomon L, Muñoz A, Astemborski J, Taylor E, Burnley A, Nelson K (1993). "Detection of human immunodeficiency virus type 1 infection by polymerase chain reaction in a cohort of seronegative intravenous drug users". J Infect Dis 168 (2): 327–31. doi:10.1093/infdis/168.2.327. PMID 8335969.
- ^ "Simultaneous detection of multiplex-amplified human immunodeficiency virus type 1 RNA, hepatitis C virus RNA, and hepatitis B virus DNA using a flow cytometer microsphere-based hybridization assay", J Clin Microbiol. 2000 Mar;38(3):1066-71
- ^ Instruction Manual - MPCR Kit for Human Immunodeficiency Virus (HIV) Type I/II, MaximBio
- ^ "Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection", AIDS. 2003 Sep 5;17(13):1871-9.
- ^ FDA summary of branched DNA test, accessed 5 Oct 2006.
- ^ http://www.cdc.gov/mmwr/preview/mmwrhtml/mm57e618a1.htm?s_cid=mm57e618a1_e
- ^ http://www.aboutmyhealth.us/oraquick.htm
- ^ [1]
- ^ http://freehivtesting.hafnyc.org/node/2
- ^ http://www.harlemunited.org/pep/testing.html
- ^ AIDSTruth.org, a site focused on examining AIDS denialist claims. Accessed 5 October 2006.
- ^ National Institutes of Health fact sheet on the connection between HIV and AIDS. Accessed 5 October 2006.
- ^ Series of articles from Science magazine, debunking the claims of AIDS denialists. Accessed 5 October 2006.
External links
- UNAIDS issues HIV testing policy June 2004
- HIV Antibody Assays resource from UCSF
- List of HIV tests approved by the U.S. FDA
- A toolkit to design campaigns to promote HIV testing in different scenarios
- Summary of HIV Test Methods (presentation with photographs)
Medical test: Infectious blood tests (CPT 87001-87999) Bacterial infection Viral infection HIV (HIV test, BDNA test, mChip) · Epstein-Barr virus (monospot test) · Dengue fever (NS1 antigen test)Protozoan infection Categories:- Infectious disease blood tests
- HIV/AIDS


Wikimedia Foundation. 2010.