- Eye injury
-
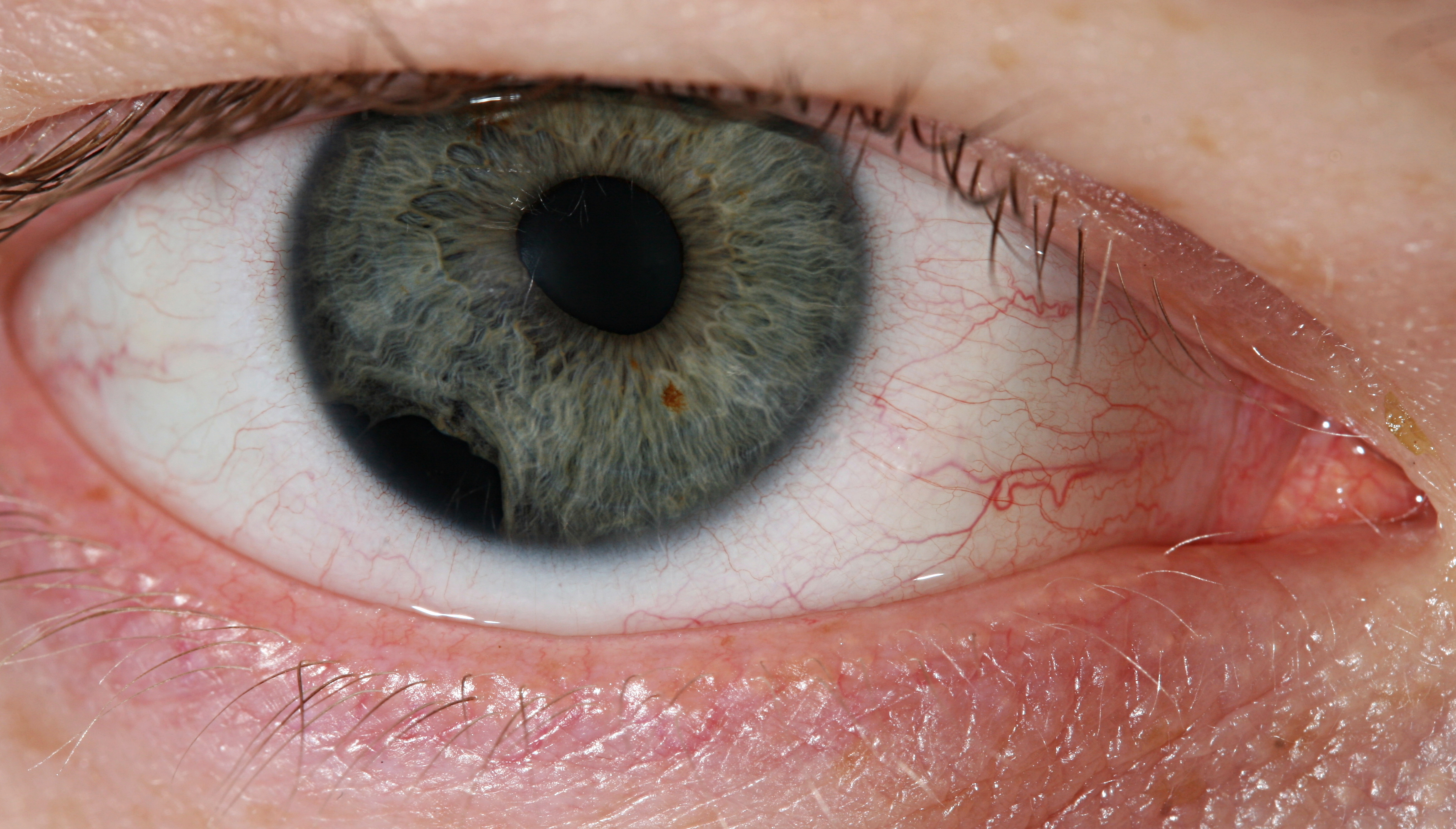
 A small piece of iron has lodged near the margin of the cornea
A small piece of iron has lodged near the margin of the cornea
 Eye injury by impact of small plastic body.
Eye injury by impact of small plastic body.Physical or chemical injuries of the eye can be a serious threat to vision if not treated appropriately and in a timely fashion. The most obvious presentation of ocular (eye) injuries is redness and pain of the affected eyes. This is not, however, universally true, as tiny metallic projectiles may cause neither symptom. Tiny metallic projectiles should be suspected when a patient reports metal on metal contact, such as with hammering a metal surface. Intraocular foreign bodies do not cause pain because of the lack of nerve endings in the vitreous humour and retina that can transmit pain sensations. As such, general or emergency room doctors should refer cases involving the posterior segment of the eye or intraocular foreign bodies to an ophthalmologist. Ideally, ointment would not be used when referring to an ophthalmologist, since it diminishes the ability to carry out a thorough eye examination.
Contents
Causes
Flicking sand, flying pieces of wood, metal, glass, stone and other material are notorious for causing much of the eye trauma. Sporting balls such as cricket ball, lawn tennis ball, squash ball), shuttle cock (from Badminton) and other high speed flying objects can strike the eye. The eye is also succeptible to blunt trauma in a fistfight. The games of young children such as bow-and-arrows, bb guns and firecrackers can lead to eye trauma. Road traffic accidents (RTAs) with head and facial trauma may also have an eye injury - these are usually severe in nature with multiple lacerations, shards of glasses embedded in tissues, orbital fractures, severe hematoma and penetrating open-globe injuries with prolapse of eye contents. Other causes of intraocular trauma may arise from workplace tools or even common household implements.[1]
Effects of eye injury
- Closed globe injury or Non-penetrating trauma: The eye globe is intact, but the seven rings of the eye have been classically described as affected by blunt trauma.
- Penetrating trauma: The globe integrity is disrupted by a full-thickness entry wound and may be associated with prolapse of the internal contents of the eye.
- Perforating trauma: The globe integrity is disrupted in two places due to an entrance and exit wound (through and through injury). This is a quite severe type of eye injury.
- Blowout fracture of the orbit is caused by blunt trauma, classically described for fist or ball injury, leading to fracture of the floor or medial wall of the orbit due to sudden increased pressure on the orbital contents.
Epidemiology
A recent study estimated that from 2002-2003 there were 27,152 injuries in the United States related to the wearing of eyeglasses.[2] The same study concluded that sports-related injuries due to eyeglasses wear were more common in those under the age of 18 and that fall-related injuries due to eyeglasses wear were more common in those aged 65 or more.[2] Although eyeglasses-related injuries do occur, prescription eyeglasses and non-prescription sunglasses have been found to "offer measurable protection which results in a lower incidence of severe eye injuries to those wearing [them]".[3]
Investigation
The goal of investigation is the assessment of the severity of the ocular injury with an eye to implementing a management plan as soon as is required. The usual eye examination should be attempted, and may require a topical anesthetic in order to be tolerable. Many topical agents cause burning upon instillation. Proxymetacaine has been found to have the best tolerance.[4]
The first step is to assess the external condition of the eye and orbit, and check for perforations, hyphema, uveal prolapse, or globe penetration. If the pupil is teardrop-shaped, and the anterior chamber is flat, this is almost always a perforating injury of the cornea or limbal area.
Depending on the medical history and preliminary examination, the primary care physician should designate the eye injury as a true emergency, urgent or semi-urgent.
Emergency
An emergency must be treated within minutes. This would include chemical burns of the conjunctiva and cornea.
Urgent
An urgent case must be treated within hours. This includes penetrating globe injuries; corneal abrasions or corneal foreign bodies; hyphema (must be referred)' eyelid lacerations that are deep, involve the lid margin or involve the lacrimal canaliculi; radiant energy burns such as arc eye (welder's burn) or snow blindness; or, rarely, traumatic optic neuropathy.
Semi-urgent
Semi-urgent cases must be managed within 1–2 days. They include orbital fractures and subconjunctival hemorrhages.
Management
Irrigation
The first line of management for chemical injuries is usually copious irrigation of the eye with an isotonic saline or sterile water. In the cases of chemical burns, one should not try to buffer the solution, but instead dilute it with copious flushing.
Patching
Depending on the type of ocular injury, either a pressure patch or shield patch should be applied. In most cases, such as those of corneal abrasion or the like, a pressure patch should be applied that ensures some tension is applied to the eye, and that the patient cannot open his or her eye under the patch. In cases of globe penetration, pressure patches should never be applied, and instead a shield patch should be applied that protects the eye without applying any pressure. If a shield patch is applied to one eye, the other eye should be also be patched due to eye movement. If the uninjured eye moves, the injured eye will also move involuntarily possibly causing more damage.
Suturing
In cases of eyelid laceration, sutures may be a part of appropriate management by the primary care physician so long as the laceration does not threaten the canaliculi, is not deep, and does not affect the lid margins.
Complications
Multiple complications are known to occur following eye injury: corneal scarring, hyphema, iridodialysis, post-traumatic glaucoma, uveitis cataract, vitreous hemorrhage and retinal detachment. The complications risk is high with retinal tears, penetrating injuries and severe blunt trauma.
Also see
- Chemical eye injury
- Wilderness medical emergencies
References
- ^ Feist RM, Lim JI, Joondeph BC, Pflugfelder SC, Mieler WF, Ticho BH, Resnick K. "Penetrating ocular injury from contaminated eating utensils." Archives of Ophthalmology. 1991 Jan;109(1):23-30. PMID 1987951.
- ^ a b Sinclair SA, Smith GA, Xiang H. "Eyeglasses-related injuries treated in U.S. emergency departments in 2002-2003." Ophthalmic Epidemiol. 2006 Feb;13(1):23-30. PMID 16510343.
- ^ May DR, Kuhn FP, Morris RE, Witherspoon CD, Danis RP, Matthews GP, Mann L. "The epidemiology of serious eye injuries from the United States Eye Injury Registry." Graefes Arch Clin Exp Ophthalmol. 2000 Feb;238(2):153-7. PMID 10766285.
- ^ "BestBets: Proxymetacaine is the local anaesthetic of choice for removal of corneal foreign bodies". http://www.bestbets.org/bets/bet.php?id=892.
See also
- List of eye diseases and disorders
- Facial trauma
- Black eye
- United States Eye Injury Registry, which compiles statistics regarding eye injuries in the United States.
Nonmusculoskeletal injuries of head (head injury) and neck (S00–S19, 850–854) Intracranial see neurotraumaExtracranial/
facial traumaEither/both M: EYE
anat(g/a/p)/phys/devp/prot
noco/cong/tumr, epon
proc, drug(S1A/1E/1F/1L)
M: EAR
anat(e/p)/phys/devp
noco/cong, epon
proc, drug(S2)
Categories:- Injuries of head
- Diseases of the eye and adnexa

Wikimedia Foundation. 2010.