- Posterior urethral valve
-
Posterior urethral valve Classification and external resources 
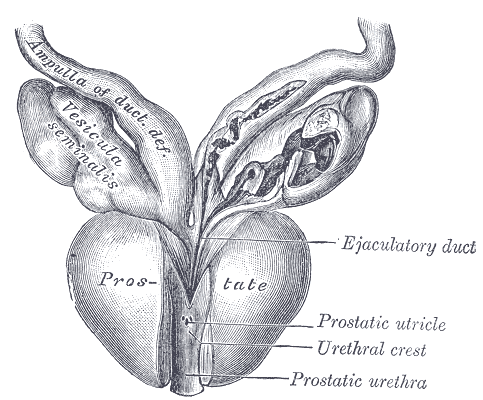
Vesiculæ seminales and ampullæ of ductus deferentes, seen from the front. Posterior urethral valves are at the dorsal aspect (back) of the prostatic urethra.DiseasesDB 34137 eMedicine ped/2357 radio/572 Posterior urethral valve (PUV) disorder is an obstructive developmental anomaly in the urethra and genitourinary system of male newborns.[1] A posterior urethral valve is an obstructing membrane in the posterior male urethra as a result of abnormal in utero development. It is the most common cause of bladder outlet obstruction in male newborns. The disorder varies in degree, with mild cases followed conservatively. More severe cases can have renal failure and even respiratory failure from lung underdevelopment as result of low amniotic fluid volumes, requiring intensive care and close monitoring.[2]
Contents
Classification
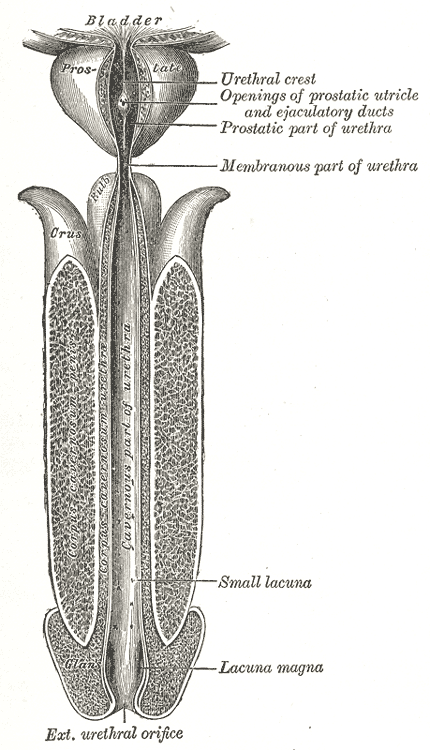
 The male urethra laid open on its anterior (upper) surface. Posterior valves are usually fusion of the plicae colliculi between the entrance of the seminal vesicles at the veromontanum, and extend to the membranous urethra.
The male urethra laid open on its anterior (upper) surface. Posterior valves are usually fusion of the plicae colliculi between the entrance of the seminal vesicles at the veromontanum, and extend to the membranous urethra.
Posterior urethral obstruction was first classified by H. H. Young in 1919. The verumontanum, or mountain ridge, is a distinctive landmark in the prostatic urethra, important in the systemic division of posterior valve disorders:
- Type I - Most common type; due to anterior fusing of the plicae colliculi, mucosal fins extending from the bottom of the verumontanum distally along the prostatic and membranous urethra[3]
- Type II - Least common variant; vertical or longitudinal folds between the verumontanum and proximal prostatic urethra and bladder neck
- Type III - Less common variant; a disc of tissue distal to verumontanum, also theorized to be a developmental anomaly of congenital urogenital remnants in the bulbar urethra
Researchers have suggested that obstructions in the posterior urethra are more appropriately termed congenital obstructions of the posterior urethral membrane (COPUMs). The congenital urothelial remnants of type III posterior urethral valves have been eponymously referred to as Cobb's collar or Moorman's ring.[4]
Diagnosis
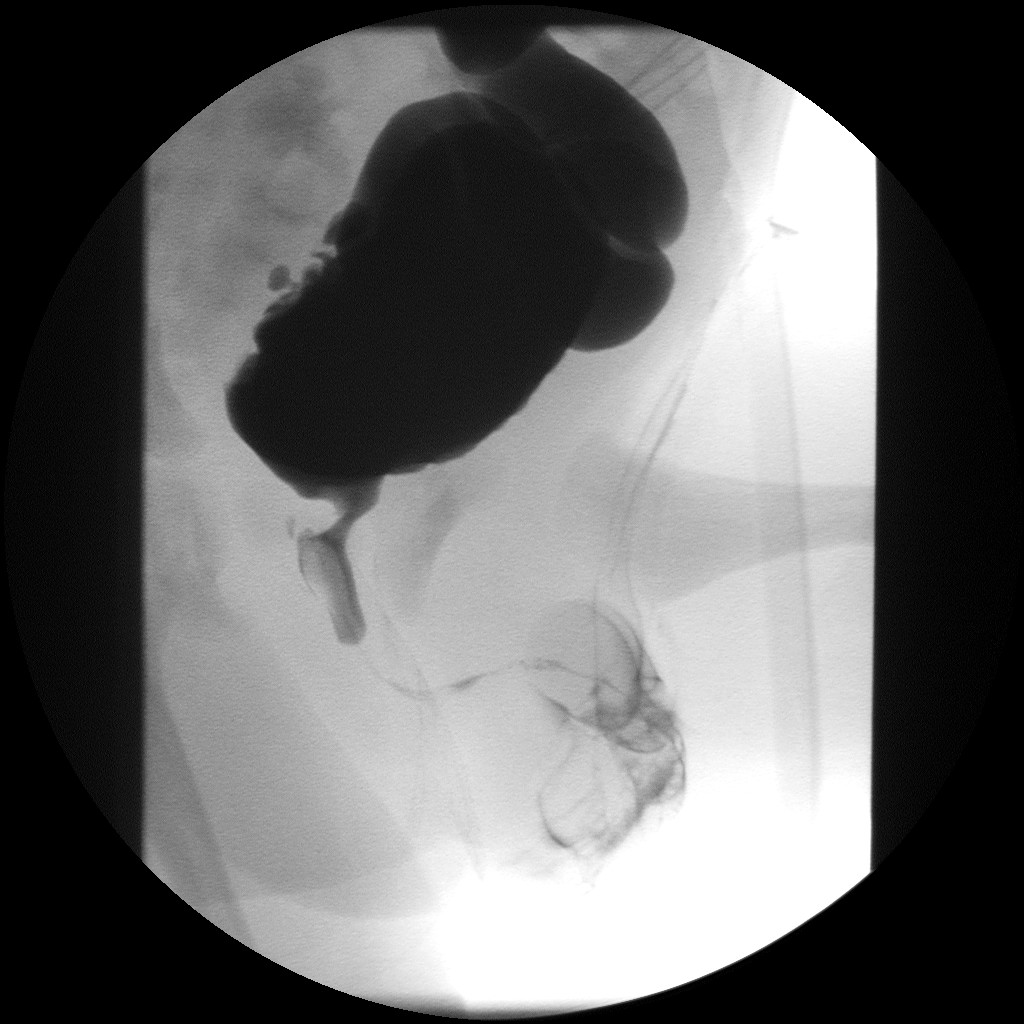
 Postvesicular obstruction due to urethral valves.
Postvesicular obstruction due to urethral valves.Abdominal ultrasound is of some benefit, but not diagnostic. Features that suggest posterior urethral valves are bilateral hydronephrosis, a thickened bladder wall with thickened smooth muscle trabeculations, and bladder diverticula.
Voiding cystourethrogram (VCUG) is more specific for the diagnosis. Normal plicae circularis are variable in appearance and often not seen on normal VCUGs. PUV on voiding cystourethrogram is characterized by an abrupt tapering of urethral caliber near the verumontanum, with the specific level depending on the developmental variant. Vesicoureteral reflux is also seen in over 50% of cases.
Diagnosis can also be made by cystoscopy, where a small camera is inserted into the urethra for direct visualization of the posteriorly positioned valve. A limitation of this technique is that posterior valve tissue is translucent and can be pushed against the wall of the ureter by inflowing irrigation fluid, making it difficult to visualize.
Centers in Europe and Japan have also had excellent results with cystosonography, although it has not been approved for use in the United States yet.[5]
Treatment
Treatment is by endoscopic valve ablation. Fetal surgery is a high risk procedure reserved for cases with severe oligohydramnios, to try to limit the associated lung underdevelopment, or pulmonary hypoplasia, that is seen at birth in these patients. The risks of fetal surgery are significant and include limb entrapment, abdominal injury, and fetal or maternal death. Specific procedures for in utero intervention include infusions of amniotic fluid, serial bladder aspiration, and creating a connection between the amniotic sac and the fetal bladder, or vesicoamniotic shunt.[5]
There are three specific endoscopic treatments of posterior urethral valves:
- Vesicostomy followed by valve ablation - a stoma, or hole, is made in the urinary bladder, also known as high diversion, after which the valve is ablated and the stoma is closed.
- Pyelostomy followed by valve ablation - stoma is made in the pelvis of the kidney as a slightly lower high diversion, after which the valve is ablated and the stoma is closed
- Primary (transurethral) valve ablation - the valve is removed through the urethra without creation of a stoma
The standard treatment is primary (transurethral) ablation of the valves.[6] Urinary diversion is used in selected cases,[6] and its benefit is disputed.[7][8]
Following surgery, the follow-up in patients with posterior urethral valve syndrome is long term, and often requires a multidisicplinary effort between general pediatricians, pulmonologists, neonatologists, radiologists and the family of the patient. Care must be taken to promote proper bladder compliance and renal function, as well as to monitor and treat the significant lung underdevelopment that can accompany the disorder.
Complications
Female homolog
The female homolog to the male verumontanum from which the valves originate is the hymen.
References
- ^ Manzoni C, Valentini A (2002). "Posterior urethral valves.". Rays 27 (2): 131–4. PMID 12696266.
- ^ "Emedicine - Posterior urethral valves - overview and treatment.". Emedicine. http://emedicine.medscape.com/article/412226-overview. Retrieved July 26, 2010.
- ^ "Nationwide Childrens Hospital, Radiology - Posterior urethral valves". Nationwide Childrens Hospital. http://www.nationwidechildrens.org/gd/applications/radiology/atlas/Urethra%20Atlas/Plicae%20colliculi.html. Retrieved July 26, 2010.
- ^ "Nationwide Childrens Hospital, Radiology - Cobb's Collar". Nationwide Childrens Hospital. http://www.nationwidechildrens.org/gd/applications/radiology/atlas/Urethra%20Atlas/Plicae%20colliculi.html. Retrieved July 26, 2010.
- ^ a b "Emedicine - Posterior Urethral Valves - Diagnosis and Treatment". Emedicine. http://emedicine.medscape.com/article/412226. Retrieved July 18, 2010.[dead link]
- ^ a b Warren J, Pike JG, Leonard MP. Posterior urethral valves in Eastern Ontario - a 30 year perspective. Can J Urol. 2004 Apr;11(2):2210-5. PMID 15182412.
- ^ Kim YH, Horowitz M, Combs A, Nitti VW, Libretti D, Glassberg KI. Comparative urodynamic findings after primary valve ablation, vesicostomy or proximal diversion. J Urol. 1996 Aug;156(2 Pt 2):673-6. PMID 8683757.
- ^ Smith GH, Canning DA, Schulman SL, Snyder HM 3rd, Duckett JW. The long-term outcome of posterior urethral valves treated with primary valve ablation and observation. J Urol. 1996 May;155(5):1730-4. PMID 8627873.
Congenital malformations and deformations of urinary system (Q60–Q64, 753) Abdominal KidneyPelvic Vestigial Categories:- Congenital disorders of urinary system
- Pediatrics
Wikimedia Foundation. 2010.