- Diaphragmatic rupture
-
Diaphragmatic rupture Classification and external resources 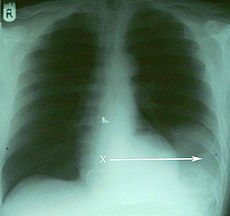
An X-ray showing the spleen in the left lower portion of the chest cavity (X and arrow) after a diaphragmatic tear[1]ICD-10 S27.8 ICD-9 862.1 ICD-O: S27.8 eMedicine med/3487 emerg/136 Diaphragmatic rupture (also called diaphragmatic injury or tear) is a tear of the diaphragm, the muscle across the bottom of the ribcage that plays a crucial role in respiration. Most commonly, acquired diaphragmatic tears result from physical trauma. Diaphragmatic rupture can result from blunt or penetrating trauma[2] and occurs in about 5% of cases of severe blunt trauma to the trunk.[3]
Diagnostic techniques include X-ray, computed tomography, and surgical techniques such as laparotomy. Diagnosis is often difficult because signs may not show up on X-ray, or signs that do show up appear similar to other conditions. Signs and symptoms included chest and abdominal pain, difficulty breathing, and decreased lung sounds. When a tear is discovered, surgery is needed to repair it.
Injuries to the diaphragm are usually accompanied by other injuries, and they indicate that more severe injury may have occurred. The outcome often depends more on associated injuries than on the diaphragmatic injury itself.[4] Since the pressure is higher in the abdominal cavity than the chest cavity, rupture of the diaphragm is almost always associated with herniation of abdominal organs into the chest cavity, called traumatic diaphragmatic hernia.[5] This herniation can interfere with breathing, and blood supply can be cut off to organs that herniate through the diaphragm, damaging them.
Contents
Signs and symptoms
Breath sounds on the side of the rupture may be diminished, respiratory distress may be present, and the chest or abdomen may be painful.[3] Orthopnea, dyspnea which occurs when lying flat, may also occur,[6] and coughing is another sign.[5] In people with herniation of abdominal organs, signs of intestinal blockage or sepsis in the abdomen may be present.[5] Bowel sounds may be heard in the chest, and shoulder or epigastric pain may be present.[4] When the injury is not noticed right away, the main symptoms are those that indicate bowel obstruction.[4]
Causes
The injury may be caused by blunt trauma, penetrating trauma, and by iatrogenic causes (as a result of medical intervention), for example during surgery to the abdomen or chest.[4] Injury to the diaphragm is reported to be present in 8% of cases of blunt chest trauma.[7] In cases of blunt trauma, vehicle accidents and falls are the most common causes.[4] Penetrating trauma has been reported to cause 12.3–20% of cases, but it has also been proposed as a more common cause than blunt trauma; discrepancies could be due to varying regional, social, and economic factors in the areas studied.[2] Stab and gunshot wounds can cause diaphragmatic injuries.[4] Clinicians are trained to suspect diaphragmatic rupture particularly if penetrating trauma has occurred to the lower chest or upper abdomen.[8] With penetrating trauma, the contents of the abdomen may not herniate into the chest cavity right away, but they may do so later, causing the presentation to be delayed.[4] Since the diaphragm moves up and down during breathing, penetrating trauma to various parts of the torso may injure the diaphragm; penetrating injuries as high as the third rib and as low as the twelfth have been found to injure the diaphragm.[9]
Mechanism
Although the mechanism is unknown, it is proposed that a blow to the abdomen may raise the pressure within the abdomen so high that the diaphragm bursts.[4] Blunt trauma creates a large pressure gradient between the abdominal and thoracic cavities; this gradient, in addition to causing the rupture, can also cause abdominal contents to herniate into the thoracic cavity.[6] Abdominal contents in the pleural space interfere with breathing and cardiac activity.[6] They can interfere with the return of blood to the heart and prevent the heart from filling effectively, reducing cardiac output.[6] If ventilation of the lung on the side of the tear is severely inhibited, hypoxemia (low blood oxygen) results.[6]
Usually the rupture is on the same side as an impact.[9] A blow to the side is three times more likely to cause diaphragmatic rupture than a blow to the front.[9]
Diagnosis
Initially, diagnosis can be difficult, especially when other severe injuries are present; thus the condition is commonly diagnosed late.[3] Chest X-ray is known to be unreliable in diagnosing diaphragmatic rupture;[6] it has low sensitivity and specificity for the injury.[5] Often another injury such as pulmonary contusion masks the injury on the X-ray film.[4] Half the time, initial X-rays are normal; in most of those that are not, hemothorax or pneumothorax is present.[6] However, there are signs detectable on X-ray films that indicate the injury. On an X-ray, the diaphragm may appear higher than normal.[3] Gas bubbles may appear in the chest, and the mediastinum may appear shifted to the side.[3] A nasogastric tube from the stomach may appear on the film in the chest cavity; this sign is pathognomonic for diaphragmatic rupture, but it is rare.[6] A contrast medium that shows up on X-ray can be inserted through the nasogastric tube to make a diagnosis.[3] The X-ray is better able to detect the injury when taken from the back with the patient upright, but this is not usually possible because the patient is usually not stable enough; thus it is usually taken from the front with the patient lying supine.[5] Positive pressure ventilation helps keep the abdominal organs from herniating into the chest cavity, but this also can prevent the injury from being discovered on an X-ray.[6]
Computed tomography has an increased accuracy of diagnosis over X-ray,[7] but no specific findings on a CT scan exist to establish a diagnosis.[8] Although CT scanning increases chances that diaphragmatic rupture will be diagnosed before surgery, the rate of diagnosis before surgery is still only 31–43.5%.[7] Another diagnostic method is laparotomy, but this misses diaphragmatic ruptures up to 15% of the time.[6] Often diaphragmatic injury is discovered during a laparotomy that was undertaken because of another abdominal injury.[6] Thoracoscopy is more reliable in detecting diaphragmatic tears than laparotomy and is especially useful when chronic diaphragmatic hernia is suspected.[6]
Location
Between 50 and 80% of diaphragmatic ruptures occur on the left side.[5] It is possible that the liver, which is situated in the right upper quadrant of the abdomen, cushions the diaphragm.[4] However, injuries occurring on the left side are also easier to detect in X-ray films.[6] Half of diaphragmatic ruptures that occur on the right side are associated with liver injury.[5] Injuries occurring on the right are associated with a higher rate of death and more numerous and serious accompanying injuries.[9] Bilateral diaphragmatic rupture, which occurs in 1–2% of ruptures, is associated with a much higher death rate (mortality) than injury that occurs on just one side.[5]
Treatment
Since the diaphragm is in constant motion with respiration, and because it is under tension, lacerations will not heal on their own.[9] Surgery is needed to repair a torn diaphragm.[3] Most of the time, the injury is repaired during laparotomy.[8] Other injuries, such as hemothorax, may present a more immediate threat and may need to be treated first if they accompany diaphragmatic rupture.[4] Video-assisted thoracoscopy may be used.[6]
Prognosis
In most cases, isolated diaphragmatic rupture is associated with good outcome if it is surgically repaired.[4] The death rate (mortality) for diaphragmatic rupture after blunt and penetrating trauma is estimated to be 15–40% and 10–30% respectively, but other injuries play a large role in determining outcome.[4]
Complications
A significant complication of diaphragmatic rupture is traumatic diaphragmatic herniation: organs such as the stomach that herniate into the chest cavity and may be strangulated, losing their blood supply.[3] Herniation of abdominal organs is present in 3–4% of people with abdominal trauma who present to a trauma center.[8]
Epidemiology
Diaphragmatic injuries are present in 1–7% of people with significant blunt trauma[4] and an average of 3% of abdominal injuries.[8] A high body mass index may be associated with a higher risk of diaphragmatic rupture in people involved in vehicle accidents.[4] It is rare for the diaphragm alone to be injured, especially in blunt trauma; other injuries are associated in as many as 80–100% of cases.[6][7] In fact, if the diaphragm is injured, it is an indication that more severe injuries to organs may have occurred.[7] Thus, the mortality after a diagnosis of diaphragmatic rupture is 17%, with most deaths due to lung complications.[7] Common associated injuries include head injury, injuries to the aorta, fractures of the pelvis and long bones, and lacerations of the liver and spleen.[6] Associated injuries occur in over three quarters of cases.[9]
History
 Ambroise Paré
Ambroise Paré
In 1579, Ambroise Paré made the first description of diaphragmatic rupture, in a French artillery captain who had been shot eight months before his death from complications of the rupture.[8] Using autopsies, Paré also described diaphragmatic rupture in people who had suffered blunt and penetrating trauma.[8] Reports of diaphragmatic herniation due to injury date back at least as far as the 17th century.[8] Petit was the first to establish the difference between acquired and congenital diaphragmatic hernia, which results from a congenital malformation of the diaphragm. In 1888, Naumann repaired a hernia of the stomach into the left chest that was caused by trauma.[8]
References
- ^ Hariharan D, Singhal R, Kinra S, Chilton A (2006). "Post traumatic intra thoracic spleen presenting with upper GI bleed! A case report". BMC Gastroenterol 6: 38. doi:10.1186/1471-230X-6-38. PMC 1687187. PMID 17132174. http://www.biomedcentral.com/1471-230X/6/38.
- ^ a b Sliker CW (March 2006). "Imaging of diaphragm injuries". Radiol Clin North Am 44 (2): 199–211, vii. doi:10.1016/j.rcl.2005.10.003. PMID 16500203.
- ^ a b c d e f g h Nolan JP (2002). "Major trauma". In Adams AP, Cashman JN, Grounds RM. Recent Advances in Anaesthesia and Intensive Care: Volume 22. London: Greenwich Medical Media. pp. 182. ISBN 1-84110-117-6.
- ^ a b c d e f g h i j k l m n o Scharff JR, Naunheim KS (February 2007). "Traumatic diaphragmatic injuries". Thorac Surg Clin 17 (1): 81–5. doi:10.1016/j.thorsurg.2007.03.006. PMID 17650700.
- ^ a b c d e f g h McGillicuddy D, Rosen P (August 2007). "Diagnostic dilemmas and current controversies in blunt chest trauma". Emerg Med Clin North Am 25 (3): 695–711, viii–ix. doi:10.1016/j.emc.2007.06.004. PMID 17826213.
- ^ a b c d e f g h i j k l m n o p Karmy-Jones R, Jurkovich GJ (March 2004). "Blunt chest trauma". Current Problems in Surgery 41 (3): 211–380. doi:10.1016/j.cpsurg.2003.12.004. PMID 15097979. "A sudden increase in the pressure gradient between the pleural and peritoneal cavities that occurs with high-speed blunt trauma will lead to disruptions of the diaphragm... This same pleuroperitoneal pressure gradient will also promote migration of intraperitoneal structures into the pleural space after disruption has occurred. Once the viscera have been displaced into the pleural space, both cardiovascular and respiratory functions are compromised."
- ^ a b c d e f Weyant MJ, Fullerton DA (2008). "Blunt thoracic trauma". Seminars in Thoracic and Cardiovascular Surgery 20 (1): 26–30. doi:10.1053/j.semtcvs.2008.01.002. PMID 18420123.
- ^ a b c d e f g h i Asensio JA, Petrone P, Demitriades D, commentary by Davis JW (2003). "Injury to the diaphragm". In Moore EE, Feliciano DV, Mattox KL. Trauma. Fifth Edition. McGraw-Hill Professional. pp. 613–616. ISBN 0071370692.
- ^ a b c d e f Fleisher GR, Ludwig S, Henretig FM, Ruddy RM, Silverman BK, ed (2006). "Thoracic trauma". Textbook of Pediatric Emergency Medicine. Hagerstown, MD: Lippincott Williams & Wilkins. pp. 1446–7. ISBN 0-7817-5074-1.
Chest trauma, excluding fractures (S20–S29, 860–862) Cardiac and
circulatory system injuriesvascular: Traumatic aortic rupture (Thoracic aorta injury)heart: Myocardial contusion/Commotio cordis · Cardiac tamponade · Hemopericardium · Myocardial ruptureLung and
lower respiratory tract injuriesPneumothorax (Tension) · Hemothorax · Hemopneumothorax · Pulmonary contusion · Pulmonary laceration · Tracheobronchial injury · Diaphragmatic rupture (Diaphragmatic hernia)Categories:


Wikimedia Foundation. 2010.