- Mycobacterium leprae
-
Mycobacterium leprae 
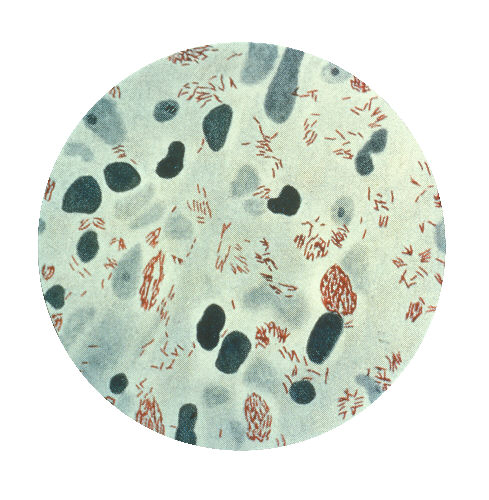
Microphotograph of Mycobacterium leprae taken from a skin lesion. Source: CDC Scientific classification Kingdom: Bacteria Phylum: Actinobacteria Order: Actinomycetales Suborder: Corynebacterineae Family: Mycobacteriaceae Genus: Mycobacterium Species: M. leprae Binomial name Mycobacterium leprae
Hansen, 1874Mycobacterium leprae, also known as Hansen’s coccus spirilly, mostly found in warm tropical countries, is a bacterium that causes leprosy (Hansen's disease).[1] It is an intracellular, pleomorphic, acid-fast bacterium.[2] M. leprae is an aerobic bacillus (rod-shaped) surrounded by the characteristic waxy coating unique to mycobacteria. In size and shape, it closely resembles Mycobacterium tuberculosis. Due to its thick waxy coating, M. leprae stains with a carbol fuscin rather than with the traditional Gram stain. The culture takes several weeks to mature.
Optical microscopy shows M. leprae in clumps, rounded masses, or in groups of bacilli side by side, and ranging from 1-8 μm in length and 0.2-0.5 μm in diameter.[3]
It was discovered in 1873 by the Norwegian physician Gerhard Armauer Hansen, who was searching for the bacteria in the skin nodules of patients with leprosy. It was the first bacterium to be identified as causing disease in humans.[4][5][verification needed] The organism has never been successfully grown on an artificial cell culture media.[2] Instead, it has been grown in mouse foot pads and more recently in nine-banded armadillos because they, like humans, are susceptible to leprosy. This can be used as a diagnostic test for the presence of bacilli in body lesions of suspected leprosy patients. The difficulty in culturing the organism appears to be because it is an obligate intracellular parasite that lacks many necessary genes for independent survival. The complex and unique cell wall that makes members of the Mycobacterium genus difficult to destroy is apparently also the reason for the extremely slow replication rate.
Virulence factors include a waxy exterior coating, formed by the production of mycolic acids unique to Mycobacterium.
M. leprae was sensitive to dapsone (diaminodiphenylsulfone, the first effective treatment which was discovered for leprosy in the 1940s), but resistance against this antibiotic has developed over time. Therapy with dapsone alone is now strongly contraindicated. Currently, a multidrug treatment (MDT) is recommended by the World Health Organization, including dapsone, rifampicin and clofazimine. In patients receiving the MDT, a high proportion of the bacilli die within a short amount of time without immediate relief of symptoms. This suggests many symptoms of leprosy must be due in part to the presence of dead cells.
Contents
Mycobacterium leprae genome
Mycobacterium leprae has the longest doubling time of all known bacteria, and has thwarted every effort at culture in the laboratory.[6] Comparing the genome sequence of M. leprae with that of Mycobacterium tuberculosis provides clear explanations for these properties, and reveals an extreme case of reductive evolution. Less than half of the genome contains functional genes. Gene deletion and decay appear to have eliminated many important metabolic activities, including siderophore production, part of the oxidative and most of the microaerophilic and anaerobic respiratory chains, and numerous catabolic systems and their regulatory circuits. [7]
The genome sequence of a strain of M. leprae, originally isolated in Tamil Nadu and designated TN, has been completed recently. The sequence was obtained by a combined approach, employing automated DNA sequence analysis of selected cosmids and whole-genome 'shotgun' clones. After the finishing process, the genome sequence was found to contain 3,268,203 base pairs (bp), and to have an average G+C content of 57.8%, values much lower than the corresponding values for M. tuberculosis, which are 4, 441,529 bp and 65.6% G+C,. About 1500 genes are common to both M. leprae and M. tuberculosis. The comparative analysis suggests both mycobacteria derived from a common ancestor and, at one stage, had gene pools of similar size. Downsizing from a genome of 4.42 Mbp, such as that of M. tuberculosis, to one of 3.27 Mbp would account for the loss of some 1200 protein-coding sequences. There is evidence that many of the genes that were present in the genome of the common ancestor of M. leprae and M. tuberculosis have been lost by recombination in the M.leprae genome. [8]
Information from the completed genome can be useful to develop diagnostic skin tests, to understand the mechanisms of nerve damage and drug resistance and to identify novel drug targets for rational design of new therapeutic regimens and drugs to treat leprosy and its complications.
Diagnostic criteria for leprosy
Diagnostic criteria for leprosy: The diagnosis of leprosy is primarily a clinical one. In one Ethiopian study, the following criteria had a sensitivity of 97% with a positive predictive value of 98% in diagnosing leprosy. Diagnosis was based on one or more of three signs: 1) Hypopigmented or reddish skin patches with definite loss of sensation 2) Thickened peripheral nerves 3) Acid-fast bacilli on skin smears or biopsy material
External links
References
- ^ Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 451–3. ISBN 0838585299.
- ^ a b McMurray DN (1996). "Mycobacteria and Nocardia.". In Baron S. et al., eds.. Baron's Medical Microbiology (4th ed.). University of Texas Medical Branch. ISBN 0-9631172-1-1. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=mmed.section.1833.
- ^ Thomas Shinnick, The Prokaryotes 2006, PART B, 1, 934-944, DOI: 10.1007/0-387-30743-5_35
- ^ Hansen GHA (1874). "Undersøgelser Angående Spedalskhedens Årsager (Investigations concerning the etiology of leprosy)" (in Norwegian). Norsk Mag. Laegervidenskaben 4: 1–88.
- ^ Irgens L (2002). "The discovery of the leprosy bacillus". Tidsskr nor Laegeforen 122 (7): 708–9. PMID 11998735.
- ^ Truman RW, Krahenbuhl JL (2001). "Viable M. leprae as a research reagent". Int. J. Lepr. Other Mycobact. Dis. 69 (1): 1–12. PMID 11480310.
- ^ Cole ST, Brosch R, Parkhill J, et al. (1998). "Deciphering the biology of Mycobacterium tuberculosis from the complete genome sequence". Nature 393 (6685): 537–44. doi:10.1038/31159. PMID 9634230.
- ^ Cole ST, Eiglmeier K, Parkhill J, et al. (2001). "Massive gene decay in the leprosy bacillus". Nature 409 (6823): 1007–11. doi:10.1038/35059006. PMID 11234002.
Actinobacteria (high-G+C) Infectious diseases · Bacterial diseases: G+ (primarily A00–A79, 001–041, 080–109) Actinomycineae Actinomyces israelii (Actinomycosis, Cutaneous actinomycosis) · Tropheryma whipplei (Whipple's disease) · Arcanobacterium haemolyticum (Arcanobacterium haemolyticum infection)Corynebacterineae Tuberculosis: Ghon focus/Ghon's complex · Pott disease · brain (Meningitis, Rich focus) · Tuberculous lymphadenitis (Tuberculous cervical lymphadenitis) · cutaneous (Scrofuloderma, Erythema induratum, Lupus vulgaris, Prosector's wart, Tuberculosis cutis orificialis, Tuberculous cellulitis, Tuberculous gumma) · Lichen scrofulosorum · Tuberculid (Papulonecrotic tuberculid) · Primary inoculation tuberculosis · Miliary · Tuberculous pericarditis · Urogenital tuberculosis · Multi-drug-resistant tuberculosis · Extensively drug-resistant tuberculosisM. lepraeLeprosy: Tuberculoid leprosy · Borderline tuberculoid leprosy · Borderline leprosy · Borderline lepromatous leprosy · Lepromatous leprosy · Histoid leprosyR3: M. avium complex/Mycobacterium avium/Mycobacterium intracellulare/MAP (MAI infection) · M. ulcerans (Buruli ulcer) · M. haemophilumCorynebacterium diphtheriae (Diphtheria) · Corynebacterium minutissimum (Erythrasma) · Corynebacterium jeikeium (Group JK corynebacterium sepsis)Bifidobacteriaceae Gardnerella vaginalisCategories:- Acid fast bacilli
- Corynebacterineae
- Leprosy
Wikimedia Foundation. 2010.