- Chronic lymphocytic leukemia
Infobox_Disease
Name = Chronic lymphocytic leukemia
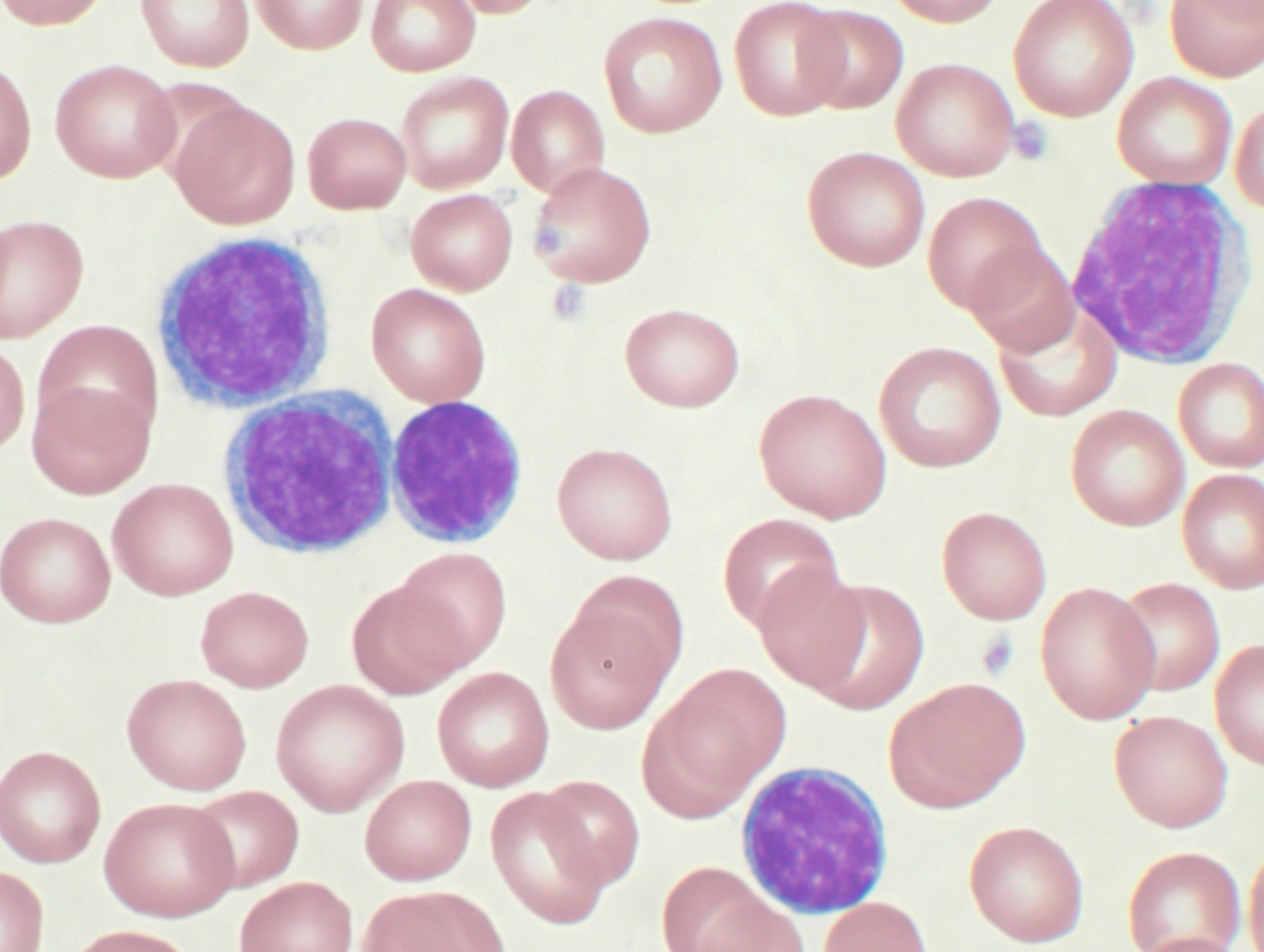
Caption = Peripheral blood smear showing CLL cells
DiseasesDB = 2641
ICD10 = ICD10|C|91|1|c|81
ICD9 = ICD9|204.9
ICDO = 9823/3 | OMIM =
MedlinePlus = 000532
eMedicineSubj = med
eMedicineTopic = 370
MeshID = D015451Chronic lymphocytic leukemia (also known as "chronic lymphoid leukemia" or "CLL"), is a type of
leukemia , or cancer of the white blood cells (lymphocytes ). CLL affects a particular lymphocyte, theB cell , which originates in the bone marrow, develops in the lymph nodes, and normally fights infection. In CLL, the DNA of a B cell is damaged, so that it can't fight infection, but it grows out of control and crowds out the healthy blood cells that can fight infection.CLL is an abnormal neoplastic proliferation of
B cells . The cells accumulate mainly in the bone marrow and blood. Although not originally appreciated, CLL is now felt to be identical to a disease calledsmall lymphocytic lymphoma (SLL), a type ofnon-Hodgkin's lymphoma which presents primarily in thelymph nodes . TheWorld Health Organization considers CLL and SLL to be "one disease at different stages, not two separate entities".cite journal |author=Harris NL, Jaffe ES, Diebold J, "et al" |title=World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November 1997 |journal=J. Clin. Oncol. |volume=17 |issue=12 |pages=3835–49 |year=1999 |pmid=10577857 |doi=]CLL is a disease of adults. Most (>75%) people newly diagnosed with CLL are over the age 50, and the majority are men. In the
United States during 2007, it is estimated there will be 15,340 new cases diagnosed and 4,500 deathscite web |url=http://www.cancer.gov/cancertopics/pdq/treatment/CLL/HealthProfessional/page1 |title=Chronic Lymphocytic Leukemia (PDQ) Treatment: General Information |author=National Cancer Institute |accessdate=2007-09-04 |format= |work=] , but because of prolonged survival, many more people are living with CLL.Fact|date=September 2007Most people are diagnosed without symptoms as the result of a routine blood test that returns a high white blood cell count, but as it advances CLL results in
swollen lymph nodes , spleen, and liver, and eventuallyanemia and infections. Early CLL is not treated, and late CLL is treated with chemotherapy and monoclonal antibodies. Survival varies from 5 years to more than 25 years. It is now possible to diagnose patients with short and long survival more precisely by examining the DNA mutations, and patients with slowly-progressing disease can be reassured and may not need any treatment in their lifetimes.cite journal |author=Chiorazzi N, Rai KR, Ferrarini M |title=Chronic lymphocytic leukemia |journal=N. Engl. J. Med. |volume=352 |issue=8 |pages=804–15 |year=2005 |pmid=15728813 |doi=10.1056/NEJMra041720]Classification and prognosis
Clinical staging
Staging, determining the extent of the disease, is done with the Rai staging system or the Binet classification (see detailscite web |url=http://www.cancer.gov/cancertopics/pdq/treatment/CLL/HealthProfessional/page2 |title=Chronic Lymphocytic Leukemia (PDQ) Treatment: Stage Information |author=National Cancer Institute |accessdate=2007-09-04 |format= |work=] ) and is based primarily on the presence, or not, of a low platelet or red cell count. Early stage disease does not need to be treated.
Gene mutation status
Recent publications suggest that twocite journal |author=Rosenwald A, Alizadeh AA, Widhopf G, "et al" |title=Relation of gene expression phenotype to immunoglobulin mutation genotype in B cell chronic lymphocytic leukemia |journal=J. Exp. Med. |volume=194 |issue=11 |pages=1639–47 |year=2001 |pmid=11733578|doi=10.1084/jem.194.11.1639] or threecite journal |author=Ghia P, Guida G, Stella S, "et al" |title=The pattern of CD38 expression defines a distinct subset of chronic lymphocytic leukemia (CLL) patients at risk of disease progression |journal=Blood |volume=101 |issue=4 |pages=1262–9 |year=2003 |pmid=12406914 |doi=10.1182/blood-2002-06-1801] prognostic groups of CLL exist based on the maturational state of the cell. This distinction is based on the maturity of the lymphocytes as discerned by the immunoglobulin variable-region
heavy chain (IgVH) gene mutation status.cite journal |author=Shanafelt TD, Byrd JC, Call TG, Zent CS, Kay NE |title=Narrative review: initial management of newly diagnosed, early-stage chronic lymphocytic leukemia |journal=Ann. Intern. Med. |volume=145 |issue=6 |pages=435–47 |year=2006 |pmid=16983131 |doi=|url=http://www.annals.org/cgi/content/full/145/6/435] High risk patients have an immature cell pattern with few mutations in the DNA in the IgVH antibody gene region whereas low risk patients show considerable mutations of the DNA in the antibody gene region indicating mature lymphocytes.Since assessment of the IgVH antibody DNA changes is difficult to perform, the presence of either
cluster of differentiation 38 (CD38 ) or Z-chain–associated protein kinase-70 (ZAP-70 ) may be surrogate markers of high risk subtype of CLL. Their expression correlates with a more immature cellular state and a more rapid disease course.Fluorescence in situ hybridization (FISH)
In addition to the maturational state, the prognosis of patients with CLL is dependent on the genetic changes within the neoplastic cell population. These genetic changes can be identified by fluorescent probes to chromosomal parts using a technique referred to as
fluorescent in situ hybridization (FISH). Four main genetic aberrations are recognized in CLL cells that have a major impact on disease behavior.
# Deletions of part of the short arm of chromosome 17 (del 17p) which target the cell cycle regulating protein p53 are particularly deleterious. Patients with this abnormality have significantly short interval before they require therapy and a shorter survival. This abnormality is found in 5-10% of patients with CLL.
# Deletions of the long arm on chromosome 11 (del 11q) are also unfavorable although not to the degree seen with del 17p. The abnormality targets the ATM gene and occurs infrequently in CLL (5-10%).
# Trisomy 12, an additional chromosome 12, is a relatively frequent finding occurring in 20-25% of patients and imparts an intermediate prognosis.
# Deletion of the long arm of chromosome 13 (del 13q) is the most common abnormality in CLL with roughly 50% of patients with cells containing this defect. These patients have the best prognosis and most will live many years, even decades, without the need for therapy. The gene targeted by this deletion is a segment that likely produces small inhibitory RNA molecules that affect expression of important death inhibiting gene products.Related diseases
In the past, cases with similar microscopic appearance in the blood but with a T cell phenotype were referred to as T-cell CLL. However, it is now recognized that these so-called T-cell CLLs are in fact a separate disease group and are currently classified as
T-cell prolymphocytic leukemia s.CLL should not be confused with
acute lymphoblastic leukemia , (ALL) a highly aggressive and highly treatable leukemia most commonly diagnosed in children.ymptoms and signs
Most people are diagnosed without symptoms as the result of a routine blood test that returns a high white blood cell count. Uncommonly, CLL presents as enlargement of the lymph nodes without a high white blood cell count or no evidence of the disease in the blood. This is referred to as
small lymphocytic lymphoma . In some individuals the disease comes to light only after the neoplastic cells overwhelm the bone marrow resulting in anemia producing tiredness or weakness.Diagnosis
The disease is easily diagnosed. CLL is usually first suspected by the presence of a
lymphocytosis , an increase in one type of the white blood cell, on a complete blood count (CBC) test. This frequently is an incidental finding on a routine physician visit. Most often the lymphocyte count is greater than 4000 cells per mm3 (microliter) of blood but can be much higher. The presence of a lymphocytosis in an elderly individual should raise strong suspicion for CLL and a confirmatory diagnostic test, in particular flow cytometry, should be performed unless clinically unnecessary.The diagnosis of CLL is based on the demonstration of an abnormal population of B lymphocytes in the blood, bone marrow, or tissues that display an unusual but characteristic pattern of molecules on the cell surface. This atypical molecular pattern includes the co-expression of cells surface markers
cluster of differentiation 5 (CD5) andcluster of differentiation 23 (CD23 ). In addition, all the CLL cells within one individual are clonal, that is genetically identical. In practice, this is inferred by the detection of only one of the mutually exclusive antibody light chains, kappa or lambda, on the entire population of the abnormal B cells. Normal B lymphocytes consist of a stew of different antibody producing cells resulting in a mixture of both kappa and lambda expressing cells. The lack of the normal distribution of kappa and lambda producing B cells is one basis for demonstrating clonality, the key element for establishing a diagnosis of any B cell malignancy (B cell Non-Hodgkin lymphoma).The combination of the microscopic examination of the peripheral blood and analysis of the lymphocytes by
flow cytometry to confirm clonality and marker molecule expression is needed to establish the diagnosis of CLL. Both are easily accomplished on a small amount of blood. Aflow cytometer is an instrument that can examine the expression of molecules on individual cells in fluids. This requires the use of specific antibodies to marker molecules with fluorescent tags recognized by the instrument. In CLL, the lymphocytes are genetically clonal, of the B cell lineage (express marker moleculescluster of differentiation 19 (CD19 ) andCD20 ), and characteristically express the marker molecules CD5 andCD23 . Morphologically, the cells resemble normal lymphocytes under the microscope, although slightly larger, and are fragile when smeared onto a glass slide giving rise to many broken cells (smudge cells).Differential diagnosis
Hematologic disorders that may resemble CLL in their clinical presentation, behavior, and microscopic appearance include mantle cell lymphoma, marginal zone lymphoma, B cell prolymphocytic leukemia, and lymphoplasmacytic lymphoma.
*B cell prolymphocytic leukemia (B PLL), is a related but more aggressive disorder, has cells with similar phenotype but that are significantly larger than normal lymphocytes and have a prominent nucleolus. The distinction is important as the prognosis and therapy differs from CLL.
*Hairy cell leukemia is also a neoplasm of B lymphocytes but the neoplastic cells have a distinct morphology under the microscope (hairy cell leukemia cells have delicate, hair-like projections on their surface) and unique marker molecule expression.All the B cell malignancies of the blood and bone marrow can be differentiated from one another by the combination of cellular microscopic morphology, marker molecule expression, and specific tumor-associated gene defects. This is best accomplished by evaluation of the patient's blood, bone marrow and occasionally lymph node cells by a
pathologist with specific training in blood disorders. Aflow cytometer is necessary for cell marker analysis and the detection of genetic problems in the cells may require visualizing the DNA changes with fluorescent probes byfluorescent in situ hybridization (FISH).Treatment
While generally considered incurable, CLL progresses slowly in most cases. Many people with CLL lead normal and active lives for many years - in some cases for decades. Because of its slow onset, early-stage CLL is generally not treated since it is believed that early CLL intervention does not improve survival time or quality of life. Instead, the condition is monitored over time to detect any change in the disease pattern. Chronic Lymphocytic Leukemia may transform into Richter's Syndrome _ a term used to describe the development of high-grade non-Hodgkin lymphoma, prolymphocytic leukemia, Hodgkin disease, or acute leukemia in a patient who has chronic lymphocytic leukemia. Its incidence is estimated to be around 5%. [Tsimberidou AM, Keating MJ. Cancer. 2005 Jan 15;103(2):216-28. "Richter syndrome: biology, incidence, and therapeutic strategies. PMID 15578683 "]
The decision to start CLL treatment is taken when the patient's clinical symptoms or blood counts indicate that the disease has progressed to a point where it may affect the patient's quality of life.
CLL treatment focuses on controlling the disease and its symptoms rather than on an outright cure. CLL is treated by
chemotherapy ,radiation therapy ,biological therapy , orbone marrow transplantation . Symptoms are sometimes treated surgically (splenectomy removal of enlarged spleen) or byradiation therapy ("de-bulking" swollen lymph nodes).Clinical "staging systems" such as the Rai 4-stage system and the Binet classification can help to determine when and how to treat the patient.
Determining when to start treatment and by what means is often difficult; studies have shown there is no survival advantage to treating the disease too early. The National Cancer Institute Working Group has issued guidelines for treatment, with specific markers that should be met before it is initiated.cite journal |author=Cheson BD, Bennett JM, Grever M, "et al" |title=National Cancer Institute-sponsored Working Group guidelines for chronic lymphocytic leukemia: revised guidelines for diagnosis and treatment |journal=Blood |volume=87 |issue=12 |pages=4990–7 |year=1996 |pmid=8652811 |doi=]
Initial CLL treatments vary depending on the exact diagnosis and the progression of the disease, and even with the preference and experience of the health care practitioner. There are dozens of agents used for CLL therapy, and there is considerable research activity studying them individually or in combination with each other. [cite web |url=http://www.cancer.gov/cancertopics/pdq/treatment/CLL/HealthProfessional/page5 |title=Chronic Lymphocytic Leukemia (PDQ) Treatment: Stage I, II, III, and IV Chronic Lymphocytic Leukemia|author=National Cancer Institute |accessdate=2007-09-04 |format= |work=]
Purine analogues
Although the purine analogue
fludarabine was shown to give superior response rates thanchlorambucil as primary therapy,cite journal |author=Rai KR, Peterson BL, Appelbaum FR, "et al" |title=Fludarabine compared with chlorambucil as primary therapy for chronic lymphocytic leukemia |journal=N. Engl. J. Med. |volume=343 |issue=24 |pages=1750–7 |year=2000 |pmid=11114313|doi=10.1056/NEJM200012143432402] cite journal |author=Steurer M, Pall G, Richards S, Schwarzer G, Bohlius J, Greil R |title=Purine antagonists for chronic lymphocytic leukaemia |journal=Cochrane database of systematic reviews (Online) |volume=3 |issue= |pages=CD004270 |year=2006 |pmid=16856041 |doi=10.1002/14651858.CD004270.pub2] there is no evidence that early use of fludarabine improves overall survival, and some clinicians prefer to reserve fludarabine for relapsed disease.Monoclonal antibodies
Monoclonal antibodies arealemtuzumab (directed againstCD52 ) andrituximab (directed againstCD20 ).Combination chemotherapy
Combination chemotherapy options are effective in both newly-diagnosed and relapsed CLL. Recently, randomized trials have shown that combinations of purine analogues (fludarabine) with alkylating agents (cyclophosphamide) produce higher response rates and a longer progression-free survival than single agents:
*
fludarabine withcyclophosphamide cite journal |author=Eichhorst BF, Busch R, Hopfinger G, Pasold R, Hensel M, Steinbrecher C, Siehl S, Jäger U, Bergmann M, Stilgenbauer S, Schweighofer C, Wendtner CM, Döhner H, Brittinger G, Emmerich B, Hallek M, German CLL Study Group. |title=Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia |journal=Blood |year=2006 |volume=107 |pages=885–91. |doi=10.1182/blood-2005-06-2395 |pmid=16219797 |unused_data=|pmid16219797 ]
*fludarabine withrituximab cite journal |author=Byrd JC, Peterson BL, Morrison VA, "et al" |title=Randomized phase 2 study of fludarabine with concurrent versus sequential treatment with rituximab in symptomatic, untreated patients with B-cell chronic lymphocytic leukemia: results from Cancer and Leukemia Group B 9712 (CALGB 9712) |journal=Blood |volume=101 |issue=1 |pages=6–14 |year=2003 |pmid=12393429 |doi=10.1182/blood-2002-04-1258]
* FCR (fludarabine ,cyclophosphamide , andrituximab )cite journal |author=Keating MJ, O'Brien S, Albitar M, "et al" |title=Early results of a chemoimmunotherapy regimen of fludarabine, cyclophosphamide, and rituximab as initial therapy for chronic lymphocytic leukemia |journal=J. Clin. Oncol. |volume=23 |issue=18 |pages=4079–88 |year=2005 |pmid=15767648 |doi=10.1200/JCO.2005.12.051]
* CHOP (cyclophosphamide ,doxorubicin ,vincristine andprednisolone )tem cell transplantion
Allogeneic bone marrow (stem cell) transplantation is rarely used as a first-line treatment for CLL due to its risk. There is increasing interest in the use of reduced intensity allogeneic stem cell transplantation, which offers the prospect of cure for selected patients with a suitable donor.cite journal | author=Dreger P, Brand R, Hansz J, Milligan D, Corradini P, Finke J, Deliliers GL, Martino R, Russell N, Van Biezen A, Michallet M, Niederwieser D; Chronic Leukemia Working Party of the EBMT | title=Treatment-related mortality and graft-versus-leukemia activity after allogeneic stem cell transplantation for chronic lymphocytic leukemia using intensity-reduced conditioning | journal=Leukemia | year=2003 | pages=841–8 | volume=17 | issue=5 | pmid=12750695 | doi=10.1038/sj.leu.2402905]
Refractory CLL
"Refractory" CLL is a disease that no longer responds favorably to treatment. In this case more aggressive therapies, including
lenalidomide ,flavopiridol , and bone marrow (stem cell) transplantation, are considered. [cite web |url=http://www.cancer.gov/cancertopics/pdq/treatment/CLL/HealthProfessional/page6 |title=Chronic Lymphocytic Leukemia (PDQ) Treatment: Refractory Chronic Lymphocytic Leukemia|author=National Cancer Institute|accessdate=2007-09-04 |format= |work=] The monoclonal antibody,alemtuzumab (directed againstCD52 ), may be used in patients with refractory, bone marrow-based disease. cite journal | author=Keating MJ, Flinn I, Jain V, Binet JL, Hillmen P, Byrd J, Albitar M, Brettman L, Santabarbara P, Wacker B, Rai KR | title=Therapeutic role of alemtuzumab (Campath-1H) in patients who have failed fludarabine: results of a large international study | journal=Blood | year=2002 | pages=3554–61 | volume=99 | issue=10 | pmid=11986207 | doi=10.1182/blood.V99.10.3554]Epidemiology
CLL is a disease of older adults and is rarely encountered in individuals under the age of 40. Thereafter the disease incidence increases with age. Subclinical "disease" can be identified in 3.5% of normal adults [ [http://bloodjournal.hematologylibrary.org/cgi/content/abstract/100/2/635 Monoclonal B lymphocytes with the characteristics of "indolent" chronic lymphocytic leukemia are present in 3.5% of adults with normal blood counts,] Rawstron AC, Green MJ, Kuzmicki A, et al. Blood, 15 July 2002, Vol. 100, No. 2, pp. 635-639] , and in up to 8% of individuals over the age of 70Fact|date=July 2008. That is, small clones of B cells with the characteristic CLL phenotype can be identified in many healthy elderly persons. The clinical significance of these cells is unknown.
Of all cancers involving the same class of blood cell, 7% of cases are CLL/SLL.cite book
author=Turgeon, Mary Louise
title=Clinical hematology: theory and procedures
publisher=Lippincott Williams & Wilkins
location=Hagerstown, MD
year=2005
pages=283
isbn=0-7817-5007-5
quote=Frequency of lymphoid neoplasms. (Source: Modified from WHO Blue Book on Tumour of Hematopoietic and Lymphoid Tissues. 2001, p. 2001.)]Complications: hypogammaglobulinemia leading to recurrent infection, warm auto imune haemolytic anaemia in 10-15% of patients, transformation to high grade lymphoma, Richter's transformation.
References
External links
Information
* [http://www.clltopics.org CLL Topics] - Non-profit educational and patient-advocacy organization
* [http://cll.ucsd.edu CLL Research Consortium] - NCI funded program project of leading clinician and scientists trying to cure CLL.
* [http://www.leukemia-lymphoma.org/all_mat_toc.adp?item_id=3221&cat_id=1209 Leukemia & Lymphoma Society] - General CLL information.
* [http://www.cancer.gov/cancerinfo/pdq/treatment/CLL/patient/ US National Cancer Institute] - General information about CLL.
Wikimedia Foundation. 2010.