- Classification of obesity
-
 An obese male with a body mass index of 46 kg/m²: weight 146 kg (322 lb), height 177 cm (5 ft 10 in)
An obese male with a body mass index of 46 kg/m²: weight 146 kg (322 lb), height 177 cm (5 ft 10 in)
Obesity is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health.[1] Relative weight and body mass index (BMI) are nearly identical and are reasonable estimates of body fatness as measured by percentage body fat.[2] However, BMI does not account for the wide variation in body fat distribution, and may not correspond to the same degree of fatness or associated health risk in different individuals and populations.[3][4][5] Other measurements of fat distribution include the waist–hip ratio and body fat percentage. Normal weight obesity is a condition of having normal body weight, but high body fat percentages with the same health risks of obesity.[6][7]
Contents
BMI
Main article: Body mass indexBody mass index or BMI is a simple and widely used method for estimating body fat mass.[8] BMI was developed in the 19th century by the Belgian statistician and anthropometrist Adolphe Quetelet.[9] BMI is an accurate reflection of body fat percentage in the majority of the adult population. It however is less accurate in people such as body builders and pregnant women.[10] A formula combining BMI, age and gender can be used to estimate a person's body fat percentage to an accuracy of 4%.[11] An alternative method, body volume index (BVI), is being developed in an effort to better take into account different body shapes.[12]
BMI Classification < 18.5 underweight 18.5–24.9 normal weight 25.0–29.9 overweight 30.0–34.9 class I obesity 35.0–39.9 class II obesity ≥ 40.0 class III obesity BMI is calculated by dividing the subject's mass by the square of his or her height, typically expressed either in metric or US "Customary" units:
- Metric: BMI = kilograms / meters2
- US/Customary and imperial: BMI = lbx703 / in2
where lb is the subject's weight in pounds and in is the subject's height in inches.
The most commonly used definitions, established by the World Health Organization (WHO) in 1997 and published in 2000, provide the values listed in the table at right.[13]
Some modifications to the WHO definitions have been made by particular bodies. The surgical literature breaks down class III obesity into further categories, though the exact values are still disputed.[14]
- Any BMI ≥ 35 or 40 is severe obesity
- A BMI of ≥ 35 or 40–44.9 or 49.9 is morbid obesity
- A BMI of ≥ 45 or 50 is super obese
As Asian populations develop negative health consequences at a lower BMI than Caucasians, some nations have redefined obesity. The Japanese have defined obesity as any BMI greater than 25[15] while China uses a BMI of greater than 28.[16]
Waist circumference and waist–hip ratio
Main article: Abdominal obesityIn the United States a waist circumference of >102 cm in men and >88 cm in women[17] or the waist–hip ratio (the circumference of the waist divided by that of the hips of >0.9 for men and >0.85 for women) are used to define central obesity.[18]
In the European Union waist circumference of ≥ 94 cm in men and ≥ 80 cm in non pregnant women are used as cut offs for central obesity.[19]
A lower cut off of 90 cm has been recommended for South Asian and Chinese men, while a cut off of 85 cm has been recommended for Japanese men.[19]
In those with a BMI under 35, intra-abdominal body fat is related to negative health outcomes independent of total body fat.[20] Intra-abdominal or visceral fat has a particularly strong correlation with cardiovascular disease.[18] In a study of 15,000 people, waist circumference also correlated better with metabolic syndrome than BMI.[21] Women with abdominal obesity have a cardiovascular risk similar to that of men.[22] In people with a BMI over 35, measurement of waist circumference however adds little to the predictive power of BMI as most individuals with this BMI have an abnormal waist circumferences.[23]
Body fat percentage
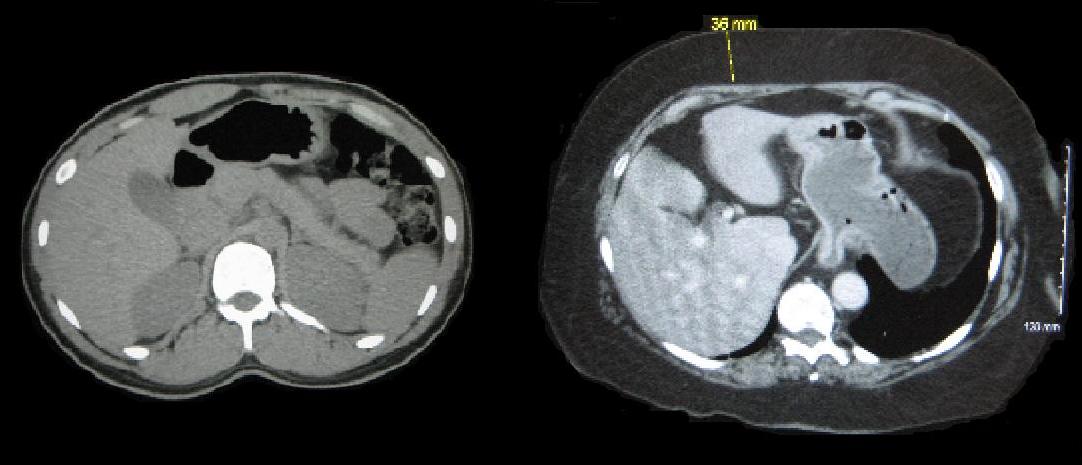
Main article: Body fat percentage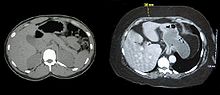 Cross-sections of the torso of a person of normal weight (left) and an obese person (right), taken by CT scan. Note the 3.6 cm (1.4 inches) of subcutaneous fat on the obese person.
Cross-sections of the torso of a person of normal weight (left) and an obese person (right), taken by CT scan. Note the 3.6 cm (1.4 inches) of subcutaneous fat on the obese person.Body fat percentage is total body fat expressed as a percentage of total body weight. There is no generally accepted definition of obesity based on total body fat. Most researchers have used >25% in men, and >30% in women, as cut-points to define obesity.[24] However, the finding that metabolic disturbance increases with increasing body fat percentage[25] suggests that focusing exclusively on cut-points of body fat percent may be of limited value.
Body fat percentage can be estimated from a person's BMI by the following formula:
- Bodyfat% = (1.2 * BMI) + (0.23 * age) − 5.4 − (10.8 * gender)
- where gender is 0 if female and 1 if male
This formula takes into account the fact that body fat percentage tends to be 10 percentage points greater in women than in men for a given BMI. It recognizes that a person's percentage body fat tends to increase as they age, even if their weight and BMI remain constant. The results of this formula have been shown to have an accuracy of 4% in one group of individuals.[26]
There are many other methods used to determine body fat percentage. Hydrostatic weighing, one of the most accurate methods of body fat calculation, involves weighting a person underwater. Two other simpler and less accurate methods have been used historically but are now not recommended.[27] The first is the skinfold test, in which a pinch of skin is precisely measured to determine the thickness of the subcutaneous fat layer.[28] The other is bioelectrical impedance analysis which uses electrical resistance. Bioelectrical impedance has not been shown to provide an advantage over BMI.[29]
Body fat percentage measurement techniques used mainly for research include computed tomography (CT scan), magnetic resonance imaging (MRI), and dual energy X-ray absorptiometry (DEXA).[20] These techniques provide very accurate measurements, but it can be difficult to obtain in the severely obese due to weight limits of most equipment and insufficient diameter of many CT or MRI scanners.[30]
Childhood obesity
Main article: Childhood obesity Variations in apparent body fat among children
Variations in apparent body fat among childrenThe healthy BMI range varies with the age and sex of the child. Obesity in children and adolescents is defined as a BMI greater than the 95th percentile.[31] The reference data that these percentiles are based on is from 1963 to 1994 and thus has not been affected by the recent increases in rates of obesity.[32]
Childhood obesity has reached epidemic proportions in 21st century with rising rates in both the developed and developing world.[citation needed] Rates of obesity in Canadian boys have increased from 11% in 1980s to over 30% in 1990s, while during this same time period rates increased from 4 to 14% in Brazilian children.[33]
As with obesity in adults many different factors contribute to the rising rates of childhood obesity. Changing diet and decreasing physical activity are believed to be the two most important in causing the recent increase in the rate of obesity. Activities from self propelled transport, to school physical education, and organized sports has been declining in many countries.[34]
Because childhood obesity often persists into adulthood, and is associated with numerous chronic illnesses, it is important that children who are obese be tested for hypertension, diabetes, hyperlipidemia, and fatty liver.[35]
Treatments used in children are primarily lifestyle interventions and behavioral techniques. Medications are not FDA approved for use in this age group.[33]
References
- ^ WHO 2000 p. 6
- ^ Gray DS, Fujioka K (1991). "Use of relative weight and Body Mass Index for the determination of adiposity". J Clin Epidemiol 44 (6): 545–50. doi:10.1016/0895-4356(91)90218-X. PMID 2037859.
- ^ WHO 2000, p. 7
- ^ Sweeting HN (2007). "Measurement and definitions of obesity in childhood and adolescence: A field guide for the uninitiated". Nutr J 6 (1): 32. doi:10.1186/1475-2891-6-32. PMC 2164947. PMID 17963490. http://www.nutritionj.com/content/6/1/32.
- ^ NHLBI p.xiv
- ^ Normal Weight Obesity: An Emerging Risk Factor for Heart and Metabolic Problems. Mayo Clinic. March 27, 2008.
- ^ Katherine Zeratsky, R.D., L.D.. Normal weight obesity: A hidden health risk?: Can you be considered obese if you have a normal body weight? Mayo Clinic - Obesity Expert Answers. Aug. 5, 2009. Retrieved 2010-1-25.
- ^ Mei Z, Grummer-Strawn LM, Pietrobelli A, Goulding A, Goran MI, Dietz WH (1 June 2002). "Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents". Am J Clin Nutr 75 (6): 978–85. PMID 12036802. http://www.ajcn.org/cgi/content/full/75/6/978.
- ^ Quetelet LAJ (1871). Antropométrie ou Mesure des Différences Facultés de l'Homme. Brussels: Musquardt.
- ^ NHLBI p.60
- ^ Seidell 2005 p.3
- ^ Romero-Corral, A. Somers, V. Lopez-Jimenez, F. Korenfeld, Y. Palin, S. Boelaert, K. Boarin, S. Sierra-Johnson, J. Rahim, A. (2008) 3-D Body Scanner, Body Volume Index: A Novel, Reproducible and Automated Anthropometric Tool Associated with Cardiometabolic Biomarkers Obesity A Research Journal 16 (1) 266-P
- ^ WHO 2000 p.9
- ^ Sturm R (July 2007). "Increases in morbid obesity in the USA: 2000-2005". Public Health 121 (7): 492–6. doi:10.1016/j.puhe.2007.01.006. PMC 2864630. PMID 17399752. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2864630.
- ^ Kanazawa M, Yoshiike N, Osaka T, Numba Y, Zimmet P, Inoue S (December 2002). "Criteria and classification of obesity in Japan and Asia-Oceania". Asia Pac J Clin Nutr 11 Suppl 8: S732–S737. doi:10.1046/j.1440-6047.11.s8.19.x. PMID 12534701. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0964-7058&date=2002&volume=11&issue=&spage=S732.
- ^ Bei-Fan Z; Cooperative Meta-Analysis Group of Working Group on Obesity in China (December 2002). "Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults: study on optimal cut-off points of body mass index and waist circumference in Chinese adults". Asia Pac J Clin Nutr 11 Suppl 8: S685–93. doi:10.1046/j.1440-6047.11.s8.9.x. PMID 12534691. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0964-7058&date=2002&volume=11&issue=&spage=S685.
- ^ Janssen I, Katzmarzyk PT, Ross R (October 2002). "Body mass index, waist circumference, and health risk: evidence in support of current National Institutes of Health guidelines". Arch. Intern. Med. 162 (18): 2074–9. doi:10.1001/archinte.162.18.2074. PMID 12374515.
- ^ a b Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L, INTERHEART Study Investigators. (2004). "Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study". Lancet 364 (9438): 937–52. doi:10.1016/S0140-6736(04)17018-9. PMID 15364185.
- ^ a b Tsigosa Constantine; Hainer, V; Basdevant, A; Finer, N; Fried, M; Mathus-Vliegen, E; Micic, D; Maislos, M et al. (April 2008). "Management of Obesity in Adults: European Clinical Practice Guidelines". The European Journal of Obesity 1 (2): 106–16. doi:10.1159/000126822. PMID 20054170.
- ^ a b U.S. Preventive Services Task Force Evidence Syntheses (2000). HSTAT: Guide to Clinical Preventive Services, 3rd Edition: Recommendations and Systematic Evidence Reviews, Guide to Community Preventive Services. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat3.section.36199.
- ^ Janssen I, Katzmarzyk PT, Ross R (2004). "Waist circumference and not body mass index explains obesity-related health risk". Am. J. Clin. Nutr. 79 (3): 379–84. doi:10.1185/030079906X159489. PMID 14985210. http://www.ajcn.org/cgi/content/abstract/79/3/379.
- ^ Larsson B, Bengtsson C, Björntorp P et al. (February 1992). "Is abdominal body fat distribution a major explanation for the sex difference in the incidence of myocardial infarction? The study of men born in 1913 and the study of women, Göteborg, Sweden". Am J Epidemiol 135 (3): 266–73. PMID 1546702.
- ^ NHLBI p.61
- ^ Okorodudu et al, 2010. International Journal of Obesity (2010) 34, 791–799
- ^ Romero-Corral et al, 2010. European Heart Journal (2010) 31, 737–746.
- ^ Seidell 2005:3.
- ^ NICE 2006 p.36
- ^ Jebb and Wells 2005 p. 16.
- ^ NICE 2006:36.
- ^ Jebb and Wells 2005 p.20
- ^ "Healthy Weight: Assessing Your Weight: BMI: About BMI for Children and Teens". Center for disease control and prevention. http://www.cdc.gov/nccdphp/dnpa/healthyweight/assessing/bmi/childrens_BMI/about_childrens_BMI.htm. Retrieved April 6, 2009.
- ^ Flegal KM, Ogden CL, Wei R, Kuczmarski RL, Johnson CL (June 2001). "Prevalence of overweight in US children: comparison of US growth charts from the Centers for Disease Control and Prevention with other reference values for body mass index". Am. J. Clin. Nutr. 73 (6): 1086–93. PMID 11382664. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=11382664.
- ^ a b Flynn MA, McNeil DA, Maloff B, et al. (February 2006). "Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with 'best practice' recommendations". Obes Rev 7 Suppl 1: 7–66. doi:10.1111/j.1467-789X.2006.00242.x. PMID 16371076.
- ^ Dollman J, Norton K, Norton L (December 2005). "Evidence for secular trends in children's physical activity behaviour". Br J Sports Med 39 (12): 892–7; discussion 897. doi:10.1136/bjsm.2004.016675. PMC 1725088. PMID 16306494. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1725088.
- ^ Fennoy I (October 1, 2008). "Childhood Obesity, Part 1: Weight Evaluation and Comorbidity Screening". Consultant for Pediatricians. http://www.consultantlive.com/cholesterol/article/1145470/1403931.
- Bibliography
- National Heart, Lung, and Blood Institute (NHLBI) (1998) (PDF). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. International Medical Publishing, Inc. ISBN 1-58808-002-1. http://www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf.
- "Obesity: guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children" (pdf). National Institute for Health and Clinical Excellence(NICE). National Health Services (NHS). 2006. http://www.nice.org.uk/nicemedia/pdf/CG43NICEGuideline.pdf. Retrieved April 8,2009.
- Puhl R., Henderson K., and Brownell K. Social consequences of obesity In:Peter G. Kopelman, Ian D. Caterson, Michael J. Stock, William H. Dietz (2005). Clinical obesity in adults and children: In Adults and Children. Blackwell Publishing. pp. 29–45. ISBN 140-511672-2.
- Jebb S. and Wells J. Measuring body composition in adults and children In:Peter G. Kopelman, Ian D. Caterson, Michael J. Stock, William H. Dietz (2005). Clinical obesity in adults and children: In Adults and Children. Blackwell Publishing. pp. 12–28. ISBN 140-511672-2.
- Kopelman P., Caterson I. An overview of obesity management In:Peter G. Kopelman, Ian D. Caterson, Michael J. Stock, William H. Dietz (2005). Clinical obesity in adults and children: In Adults and Children. Blackwell Publishing. pp. 319–326. ISBN 140-511672-2.
- Seidell JC. Epidemiology — definition and classification of obesity In:Peter G. Kopelman, Ian D. Caterson, Michael J. Stock, William H. Dietz (2005). Clinical obesity in adults and children: In Adults and Children. Blackwell Publishing. pp. 3–11. ISBN 140-511672-2.
- World Health Organization (WHO) (2000) (PDF). Technical report series 894: Obesity: Preventing and managing the global epidemic.. Geneva: World Health Organization. ISBN 92-4-120894-5. http://whqlibdoc.who.int/trs/WHO_TRS_894_(part1).pdf.
Categories:


Wikimedia Foundation. 2010.