- Targeted drug delivery
-
Targeted drug delivery, sometimes called smart drug delivery,[1] is a method of delivering medication to a patient in a manner that increases the concentration of the medication in some parts of the body relative to others. The goal of a targeted drug delivery system is to prolong, localize, target and have a protected drug interaction with the diseased tissue. The conventional drug delivery system is the absorption of the drug across a biological membrane, whereas the targeted release system is when the drug is released in a dosage form. The advantages to the targeted release system is the reduction in the frequency of the dosages taken by the patient, having a more uniform effect of the drug, reduction of drug side effects, and reduced fluctuation in circulating drug levels. The disadvantage of the system is high cost which makes productivity more difficult and the reduced ability to adjust the dosages.
Targeted drug delivery systems have been developed to optimize regenerative techniques. The system is based on a method that delivers a certain amount of a therapeutic agent for a prolonged period of time to a targeted diseased area within the body. This helps maintain the required plasma and tissue drug levels in the body. Therefore, avoiding any damage to the healthy tissue via the drug. The drug delivery system is highly integrated and requires various disciplines, such as chemists, biologist and engineers, to join forces to optimize this system.[2]
Contents
Background
In traditional drug delivery systems such as oral ingestion or intravascular injection, the medication is distributed throughout the body through the systemic blood circulation. For most therapeutic agents, only a small portion of the medication reaches the organ to be affected. Targeted drug delivery seeks to concentrate the medication in the tissues of interest while reducing the relative concentration of the medication in the remaining tissues. For example, by avoiding the host's defense mechanisms and inhibiting non-specific distribution in the liver and spleen [3], a system can reach the intended site of action in higher concentrations. Targeted delivery is believed to improve efficacy while reducing side effects.
When implementing a targeted release system, the following design criteria for the system need to taken into account: the drug properties, side effects of the drugs, the route taken for the delivery of the drug, the targeted site, and the disease.
Increasing developments to novel treatments requires a controlled microenvironment that is only accomplished through the implementation of therapeutic agents whose side effects can be avoided with targeted drug delivery. Advances in the field of targeted drug delivery to cardiac tissue will be an integral component to regenerate cardiac tissue.[4]
There are two kinds of targeted drug delivery, active targeted drug delivery, such as some antibody medications; and passive targeted drug delivery, such as the enhanced permeability and retention effect (EPR-effect).
Delivery vehicles
There are different types of drug delivery vehicles, such as, polymeric micelles, liposomes, lipoprotein-based drug carriers, nano-particle drug carriers, dendrimers etc. An ideal drug delivery vehicle must be non-toxic, biocompatible, non-immunogenic, biodegradable [4] and avoid recognition by the host's defense mechanisms[3].
Liposomes
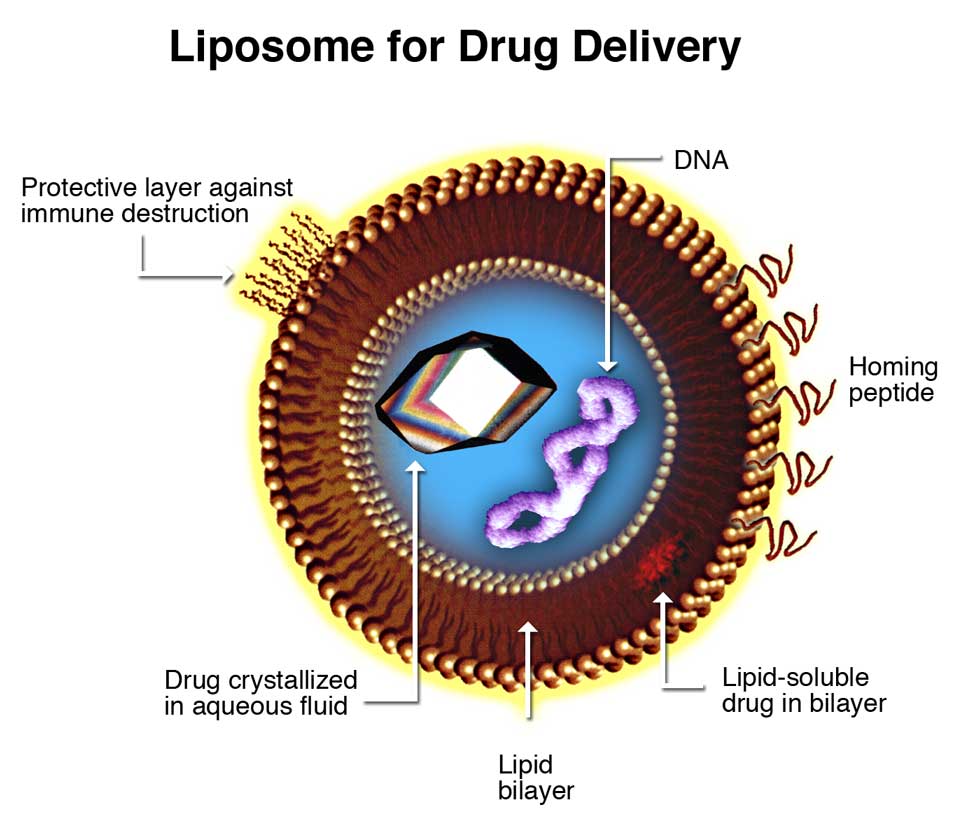
 Liposomes are composite structures made of phospholipids and may contain small amounts of other molecules. Though liposomes can vary in size from low micrometer range to tens of micrometers, unilamellar liposomes, as pictured here, are typically in the lower size range with various targeting ligands attached to their surface allowing for their surface-attachment and accumulation in pathological areas for treatment of disease.[5]
Liposomes are composite structures made of phospholipids and may contain small amounts of other molecules. Though liposomes can vary in size from low micrometer range to tens of micrometers, unilamellar liposomes, as pictured here, are typically in the lower size range with various targeting ligands attached to their surface allowing for their surface-attachment and accumulation in pathological areas for treatment of disease.[5]
The most common vehicle currently used for targeted drug delivery is the liposome.[6] Liposomes are non-toxic, non-hemolytic and non-immunogenic even upon repeated injections; they are biocompatible and biodegradable and can be designed to avoid clearance mechanisms (reticuloendothelial system (RES), renal clearance, chemical or enzymatic inactivation, etc.)[7][8]Lipid based, ligand coated nanocarriers can store their payload in the hydrophobic shell or the hydrophilic interior depending on the nature of the drug/contrast agent being carried.[4]
The only problem to using liposomes in vivo is their immediate uptake and clearance by the RES system and their relatively low stability in vitro. To combat this, polyethylene glycol (PEG) can be added to the surface of the liposomes. Increasing the mole percent of PEG on the surface of the liposomes by 4-10% significantly increased circulation time in vivo from 200 to 1000 minutes.[4]
Micelles and dendrimers
Another type of drug delivery vehicle used is polymeric micelles. They are prepared from certain amphiphilic co-polymers consisting of both hydrophilic and hydrophobic monomer units.[2] They can be used to carry drugs that have poor solubility. This method offers little in the terms of size control or function malleability. Techniques have been developed that utilize reactive polymers along with a hydrophobic additive to produce a larger micelle which create a range of sizes[9] .
Dendrimers are also polymer-based delivery vehicles. They have a core that branches out in regular intervals to form a small, spherical and very dense nanocarrier.[10]
Biodegradable particles
Biodegradable particles have the ability to target diseased tissue as well as deliver their payload as a controlled release therapy.[11] Biodegradable particles bearing ligands to P-selectin, endothelial selectin (E-selectin) and ICAM-1 have been found to adhere to inflamed endothelium.[12] Therefore the use of biodegradable particles can be also be used for cardiac tissue.
Artificial DNA nanostructures
The success of DNA nanotechnology in constructing artificially designed nanostructures out of nucleic acids such as DNA, combined with the demonstration of systems for DNA computing, has led to speculation that artificial nucleic acid nanodevices can be used to target drug delivery based upon directly sensing its environment. These methods make use of DNA solely as a structural material and a chemical, and do not make use of its biological role as the carrier of genetic information. Nucleic acid logic circuits have been demonstrated that could potentially be used as the core a system which releases a drug only in response to a stimulus such as a specific mRNA.[13] Additionally, a DNA "box" with a controllable lid has been synthesized using the DNA origami method. This structure could encapsulate a drug in its close state, and open to release it only in response to a desired stimulus.[14]
Applications
Targeted drug delivery can be used to treat many diseases, such as the cardiovascular diseases and diabetes. However, the most important application of targeted drug delivery is to treat cancerous tumors.
The American Heart Association rates cardiovascular disease as the number one cause of death in the United States. Each year 1.5 million myocardial infarctions (MI) also known as heart attacks occur in the United States with 500,000 leading to deaths. The costs related to heart attacks exceed $60 billion per year. Therefore, there is a need to come up with an optimum recovery system. The key to solving this problem lies in the effective use of pharmaceutical drugs that can be targeted directly to the diseased tissue. This technique can help develop many more regenerative techniques to cure various diseases. The development of a number of regenerative strategies in recent years for curing heart disease represents a paradigm shift away from conventional approaches which aim to manage heart disease.[4]
Stem cell therapy can be used to help regenerate myocardium tissue and return the contractile function of the heart be creating/supporting a microenvironment before the MI. Developments in targeted drug delivery to tumors have provided the groundwork for the burgeoning field of targeted drug delivery to cardiac tissue.[4] Recent developments have shown that there are different endothelial surfaces in tumors which has led to the concept of endothelial cell adhesion molecule mediated targeted drug delivery to tumors.
References
- ^ Muller, R; Keck, C (2004). "Challenges and solutions for the delivery of biotech drugs – a review of drug nanocrystal technology and lipid nanoparticles". Journal of Biotechnology 113 (1–3): 151–170. doi:10.1016/j.jbiotec.2004.06.007. PMID 15380654.
- ^ a b Saltzman, W. Mark; Torchilin, Vladimir P. (2008). "Drug delivery systems". AccessScience. McGraw-Hill Companies. http://accessscience.com/content/Drug%20delivery%20systems/757275.
- ^ Bertrand N, Leroux JC. (2011). "The journey of a drug carrier in the body: an anatomo-physiological perspective". Journal of Controlled Release. doi:10.1016/j.jconrel.2011.09.098. http://www.sciencedirect.com/science/article/pii/S0168365911009527.
- ^ a b c d e f Scott, Robert C; Crabbe, Deborah; Krynska, Barbara; Ansari, Ramin; Kiani, Mohammad F (2008). "Aiming for the heart: targeted delivery of drugs to diseased cardiac tissue". Expert Opinion on Drug Delivery 5 (4): 459–70. doi:10.1517/17425247.5.4.459. PMID 18426386.
- ^ Torchilin VP. (2006)Adv Drug Deliv Rev. 2006 Dec 1;58(14):1532-55
- ^ Cobleigh, M; Langmuir, VK; Sledge, GW; Miller, KD; Haney, L; Novotny, WF; Reimann, JD; Vassel, A (2003). "A phase I/II dose-escalation trial of bevacizumab in previously treated metastatic breast cancer". Seminars in Oncology 30 (5 Suppl 16): 117–24. doi:10.1053/j.seminoncol.2003.08.013. PMID 14613032.
- ^ Seidman, A.; Hudis, C; Pierri, MK; Shak, S; Paton, V; Ashby, M; Murphy, M; Stewart, SJ et al. (2002). "Cardiac Dysfunction in the Trastuzumab Clinical Trials Experience". Journal of Clinical Oncology 20 (5): 1215–21. doi:10.1200/JCO.20.5.1215. PMID 11870163.
- ^ Brufsky, Adam (2009). "Trastuzumab-Based Therapy for Patients With HER2-Positive Breast Cancer". American Journal of Clinical Oncology 33 (2): 186–95. doi:10.1097/COC.0b013e318191bfb0. PMID 19675448.
- ^ "Nanodelivery". http://www.license.umn.edu/Products/Polymer-Nanoparticles-Improve-Delivery-of-Compounds__Z05052.aspx.
- ^ Pili, R.; Rosenthal, M. A.; Mainwaring, P. N.; Van Hazel, G.; Srinivas, S.; Dreicer, R.; Goel, S.; Leach, J. et al. (2010). "Phase II Study on the Addition of ASA404 (Vadimezan; 5,6-Dimethylxanthenone-4-Acetic Acid) to Docetaxel in CRMPC". Clinical Cancer Research 16 (10): 2906–14. doi:10.1158/1078-0432.CCR-09-3026. PMID 20460477.
- ^ Homsi, J.; Simon, G. R.; Garrett, C. R.; Springett, G.; De Conti, R.; Chiappori, A. A.; Munster, P. N.; Burton, M. K. et al. (2007). "Phase I Trial of Poly-L-Glutamate Camptothecin (CT-2106) Administered Weekly in Patients with Advanced Solid Malignancies". Clinical Cancer Research 13 (19): 5855–61. doi:10.1158/1078-0432.CCR-06-2821. PMID 17908979.
- ^ Vogel, V. G.; Costantino, JP; Wickerham, DL; Cronin, WM; Cecchini, RS; Atkins, JN; Bevers, TB; Fehrenbacher, L et al. (2006). "Effects of Tamoxifen vs Raloxifene on the Risk of Developing Invasive Breast Cancer and Other Disease Outcomes: The NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 Trial". JAMA 295 (23): 2727–41. doi:10.1001/jama.295.23.joc60074. PMID 16754727.
- ^ Kahan, M; Gil, B; Adar, R; Shapiro, E (2008). "Towards Molecular Computers that Operate in a Biological Environment". Physica D: Nonlinear Phenomena 237 (9): 1165–1172. doi:10.1016/j.physd.2008.01.027.
- ^ Andersen, Ebbe S.; Dong, Mingdong; Nielsen, Morten M.; Jahn, Kasper; Subramani, Ramesh; Mamdouh, Wael; Golas, Monika M.; Sander, Bjoern et al. (2009). "Self-assembly of a nanoscale DNA box with a controllable lid". Nature 459 (7243): 73–6. doi:10.1038/nature07971. PMID 19424153.
Further reading
- Schroeder, Avi; Honen, Reuma; Turjeman, Keren; Gabizon, Alberto; Kost, Joseph; Barenholz, Yechezkel (2009). "Ultrasound triggered release of cisplatin from liposomes in murine tumors". Journal of Controlled Release 137 (1): 63–8. doi:10.1016/j.jconrel.2009.03.007. PMID 19303426.
- Scott, Robert C.; Wang, Bin; Nallamothu, Ramakrishna; Pattillo, Christopher B.; Perez-Liz, Georgina; Issekutz, Andrew; Valle, Luis Del; Wood, George C. et al. (2007). "Targeted delivery of antibody conjugated liposomal drug carriers to rat myocardial infarction". Biotechnology and Bioengineering 96 (4): 795–802. doi:10.1002/bit.21233. PMID 17051598.
- Scott, Robert C; Crabbe, Deborah; Krynska, Barbara; Ansari, Ramin; Kiani, Mohammad F (2008). "Aiming for the heart: targeted delivery of drugs to diseased cardiac tissue". Expert Opinion on Drug Delivery 5 (4): 459–70. doi:10.1517/17425247.5.4.459. PMID 18426386.
- Wang, Bin; Rosano, Jenna M; Cheheltani, Rabe'e; Achary, Mohan P; Kiani, Mohammad F (2010). "Towards a targeted multi-drug delivery approach to improve therapeutic efficacy in breast cancer". Expert Opinion on Drug Delivery 7 (10): 1159–73. doi:10.1517/17425247.2010.513968. PMID 20738211.
- Wang, Bin; Scott, Robert C.; Pattillo, Christopher B.; Prabhakarpandian, Balabhaskar; Sundaram, Shankar; Kiani, Mohammad F. (2008). "Modeling Oxygenation and Selective Delivery of Drug Carriers Post-Myocardial Infarction". In Kang, Kyung A.; Harrison, David K.; Bruley, Duane F.. Oxygen Transport to Tissue XXIX. Advances in Experimental Medicine and Biology. 614. Springer. pp. 333–43. doi:10.1007/978-0-387-74911-2_37. ISBN 978-0-387-74910-5. PMID 18290344.
External links

This pharmacology-related article is a stub. You can help Wikipedia by expanding it.