- Laryngomalacia
Infobox_Disease
Name = PAGENAME
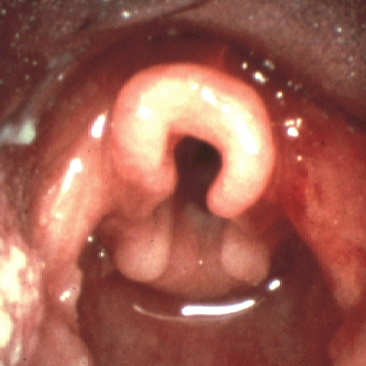
Caption = Omega shaped epiglottis, seen in laryngomalacia
DiseasesDB = 29421
ICD10 = ICD10|Q|31|5|q|30
ICD9 = ICD9|748.3
ICDO =
OMIM = 150280
MedlinePlus =
eMedicineSubj = ped
eMedicineTopic = 1280
MeshID =Laryngomalacia (literally, "soft
larynx ") is a very common condition of infancy, in which the soft, immaturecartilage of the upper larynx collapses inward during inhalation, causing airway obstruction. It can also be seen in older patients, especially those with neuromuscular conditions resulting in weakness of the muscles of the throat. However, the infantile form is much more common.Presentation
In infantile laryngomalacia, the supraglottic
larynx (the part above thevocal cords ) is tightly curled, with a short band holding the cartilage shield in the front (theepiglottis ) tightly to the mobile cartilage in the back of the larynx (the arytenoids). These bands are known as the aryepiglottic folds; they create the movements that opens and closes the vocal cords for phonation. The shortened aryepiglottic folds cause the epiglottis to be furled on itself. This is the well known "omega shaped" epiglottis in laryngomalacia.Laryngomalacia results in partial airway obstruction, most commonly causing a characteristic high-pitched squeaking noise on inhalation (inspiratory
stridor ). Some infants have feeding difficulties related to this problem. Rarely, children will have significant life threatening airway obstruction. The vast majority, however, will only have stridor without other more serious symptoms.The conventional wisdom about laryngomalacia is that the noise is more pronounced when the patient is on his or her back (with gravity making the epiglottis fall backwards). This, however, is a more common finding in older patients rather than in infants.
Causes
Although laryngomalacia is not associated with a specific gene, there is evidence that some cases may be inherited. [cite journal |author=Shulman JB, Hollister DW, Thibeault DW, Krugman ME |title=Familial laryngomalacia: a case report |journal=Laryngoscope |volume=86 |issue=1 |pages=84–91 |year=1976 |pmid=1256207 |doi=] [cite journal |author=Shohat M, Sivan Y, Taub E, Davidson S |title=Autosomal dominant congenital laryngomalacia |journal=Am. J. Med. Genet. |volume=42 |issue=6 |pages=813–4 |year=1992 |pmid=1554019 |doi=10.1002/ajmg.1320420613]
Prognosis
Laryngomalacia becomes symptomatic after the first few weeks of life, and may get louder over the first year, as the child moves air more vigorously. It generally resolves spontaneously by the second year of life.
Treatment
In rare cases, surgery is necessary. [cite journal |author=Holinger LD, Konior RJ |title=Surgical management of severe laryngomalacia |journal=Laryngoscope |volume=99 |issue=2 |pages=136–42 |year=1989 |pmid=2913424 |doi=] [cite journal |author=Zalzal GH |title=Stridor and airway compromise |journal=Pediatr. Clin. North Am. |volume=36 |issue=6 |pages=1389–402 |year=1989 |pmid=2685719 |doi=] [cite journal |author=Solomons NB, Prescott CA |title=Laryngomalacia. A review and the surgical management for severe cases |journal=Int. J. Pediatr. Otorhinolaryngol. |volume=13 |issue=1 |pages=31–9 |year=1987 |pmid=3305399 |doi=] Most commonly, this involves cutting the aryepiglottic folds to let the supraglottic airway spring open. Treatment of
gastroesophageal reflux disease can also help in the treatment of laryngomalacia, since gastric contents can cause the back part of the larynx to swell and collapse even further into the airway. In severe cases, a temporarytracheotomy may be necessary.References
Wikimedia Foundation. 2010.