- Pressure controlled intermittent mandatory ventilation
-
Pressure Controlled Intermittent Mandatory Ventilation (PC-IMV) is any mode of mechanical ventilation with preset inspiratory pressure (Pressure Control) and inspiratory time (Ti). Spontaneous breaths (i.e., inspiration is patient triggered and patient cycled) can exist between mandatory breaths (denoted by the term "intermittent"). In other words, PC-IMV means a mode of ventilation where the pressure is controlled and has an allowance for patient triggered breaths without providing an assisted breath as seen in pressure controlled continuous mandatory ventilation, but instead it allows the additional breaths to co-exist with ventilator breaths.
Contents
Pressure regulated volume control
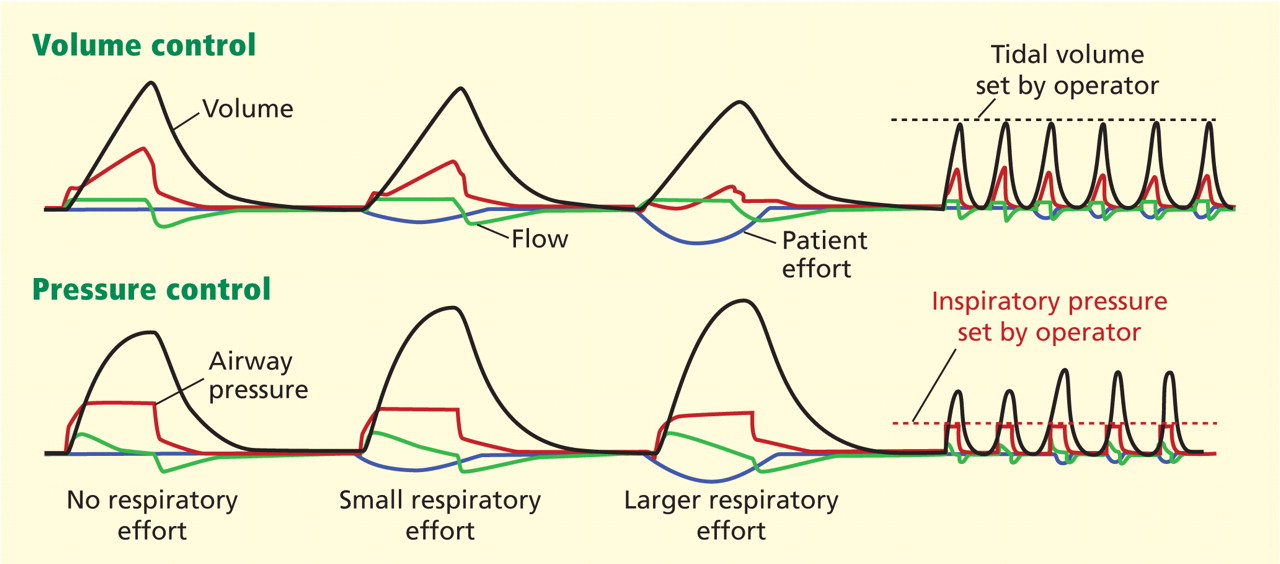
PRVC — Pressure regulated volume control is a pressure controlled mode (even though "volume control" is used in the name) with a VT set as a goal amount. Pressure varies with a peak pressure limit included to reduce lung trauma and use only the minimum pressure required to deliver the goal tidal volume (VT). Pressure regulated volume control is a mode of mechanical ventilation where the breaths are delivered mandatorily to assure preset volumes, with a constant inspiratory pressure continuously adapting to the patient's condition. The flow pattern is decelerating. This mode is a form of intermittent mandatory ventilation, the breaths can either be ventilator initiated or patient initiated. This mode combines the advantages of volume controlled and pressure controlled ventilation.
The first breath delivered to the patient is a volume controlled breath. The measured plateau pressure is used as the pressure level for the next breath. The pressure is constant during the set inspiratory time and the flow is decelerating. The set tidal volume is achieved by automatic, breath-by-breath pressure regulation. The ventilator will adjust the inspiratory pressure control level, according to the mechanical properties of the airways/lung/thorax, to the lowest possible level to guarantee the preset tidal volume. If the measured tidal volume increases above the preset, the pressure level decreases in steps of maximum 3 cmH2O (300 Pa) between consecutive breaths until the preset tidal volume is delivered. Maximum available pressure level is 5 cmH2O (500 Pa) below a preset upper pressure limit.
Advantages
- Maintains a minimum positive pressure(PIP)
- Guaranteed tidal volume (VT)
- Patient has very little work of breathing (WOB) requirement.
- Allows patient control of respiratory rate Decelerating flow waveform for improved gas distribution
- Breath by breath analysis
Disadvantages
- Varying mean airway pressure
- May cause or worsen autoPEEP
- When patient demand is increased, pressure level may diminish when support is needed
- May be tolerated poorly in awake non-sedated patients
- A sudden increase in respiratory rate and demand may result in a decrease in ventilator support
Proportional Assist Ventilation
PAV — Proportional assist ventilation is a mode in which the ventilator guarantees the percentage of work regardless of changes in pulmonary compliance and resistance.[1] The ventilator varies the tidal volume and pressure based on the patients work of breathing, the amount it delivers is proportional to the percentage of assistance it is set to give.
Adaptive Support Ventilation
Adaptive Support Ventilation (ASV) — ASV is a positive pressure mode of mechanical ventilation that is closed-loop controlled. In this mode, the frequency and tidal volume of breaths of a patient on the ventilator are automatically adjusted based on the patient’s requirements. The lung mechanics data are used to adjust the depth and rate of breaths to minimize the work rate of breathing. In the ASV mode, every breath is synchronized with patient effort if such an effort exists, and otherwise, full mechanical ventilation is provided to the patient.
ASV is a patented technology originally described as one of the embodiments of US Patent No. 4986268.[2] In this invention, the control algorithm computes the optimal rate of respiration to minimize the work rate of breathing. The rationale is to make the patient's breathing pattern comfortable and natural within safe limits, and thereby stimulate spontaneous breathing and reduce the weaning time.
Airway pressure release ventilation
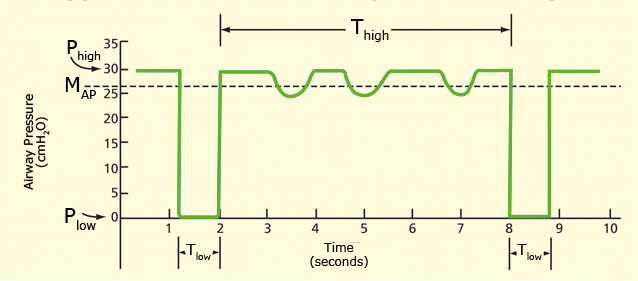
Airway pressure release ventilation (APRV) — is a relatively new strategy of ventilation that became commercially available in the United States in the mid-1990s. APRV differs fundamentally from that of conventional positive-pressure ventilation. Whereas conventional modes of mechanical ventilation begin the breathing cycle at a baseline pressure and elevate airway pressure (PIP) to accomplish tidal ventilation (VT), APRV begins at a pressure higher than the baseline pressure and follows with a deflation to accomplish tidal ventilation[3]. Fundamentally APRV is a time-cycled alternant between two levels of positive airway pressure, with the main time on the high level and a brief expiratory release to facilitate ventilation.[4]
This is a type of inverse ratio ventilation. The exhalation time (Tlow) is shortened to usually less than one second to maintain alveoli inflation. Fundamentally this is a continuous pressure with a brief release. APRV currently the most efficient conventional mode for lung protective ventilation.[5]
Settings and measurements
Settings are sometimes brand specific and the term for the individual settings may differ, however generally the settings listed here are a fundamental explanation of the purpose of the settings within the APRV mode.
- Phigh — This is the inspiratory pressure (just like in pressure control).
- Thigh — This value is the number of seconds during the inhalation phase.
- Tpeep — Also known as the Tlow, this is the time allotted for expiration.
- FiO2 — The fractional O2 percentage that is being added to the delivered air.
Perceptions and Receptions
Different perceptions of this mode may exist around the globe. While 'APRV' is common to users in North America, a very similar mode, biphasic positive airway pressure (BIPAP), was introduced in Europe.[6] The term APRV has also been used in American journals where, from the ventilation characteristics, BIPAP would have been the appropriate terminology[7]. To further confusion, BiPAP© is a registered trade-mark for a noninvasive ventilation mode in a specific ventilator (Respironics Inc.). Other names (BILEVEL, DUOPAP, BIVENT) have been created for legal reasons. Although similar in modality, these terms describe how a mode is intended to inflate the lung, rather than defining the characteristics of synchronization or the way spontaneous breathing efforts are supported.
Other terms
APRV is used by many brands and models of mechanical ventilators under different names. Most names are copyrighted as trademarks and do not represent nomenclature of mechanical ventilation but may be referred to clinically by the brand name.
Some of these names include:
- BiVent - (Servo-i ventilator by Maquet)
- BiLevel
- DuoPAP
Further reading
- Kaplan LJ. Bailey H. Formosa V. “Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome” Critical Care (London). 5(4):221-6, 2001 Aug.
- Wrigge H. Zinserling J. Hering R. Schwalfenberg N. Stuber F. von Spiegel T. Schroeder S. Hedenstierna G. Putensen C. “Cardiorespiratory effects of automatic tube compensation during airway pressure release ventilation in patients with acute lung injury.” Anesthesiology. 95(2):382-9, 2001 Aug
- Räsänen J, Cane RD, Downs JB, Hurst JM, Jousela IT, Kirby RR, Rogove HJ “Airway pressure release ventilation during acute lung injury: A prospective multicenter trial” Crit Care Med 1991; 19: 1234–41
- Putensen C. Mutz NJ. Putensen-Himmer G. Zinserling J. “Spontaneous breathing during ventilatory support improves ventilation-perfusion distributions in patients with acute respiratory distress syndrome.” American Journal of Respiratory & Critical Care Medicine. 159(4 Pt 1):1241-8, 1999 Apr.
- Sydow M. Burchardi H. Ephraim E. Zielmann S. Crozier TA. “Long-term effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation.” American Journal of Respiratory & Critical Care Medicine. 149(6):1550-6, 1994 Ju
See also
- Modes of mechanical ventilation
- Volume Controlled Continuous Mandatory Ventilation
- Volume Controlled Intermittent Mandatory Ventilation
- Pressure Controlled Continuous Mandatory Ventilation
- Pressure Controlled Intermittent Mandatory Ventilation
- Continuous Spontaneous Ventilation
References
- ^ Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145(1):114-120.
- ^ Tehrani, Fleur T., “Method and Apparatus for Controlling an Artificial Resirator,” US Patent No. 4986268, issued Jan. 22, 1991.
- ^ Frawley PM, Habashi NM (2001) Airway pressure release ventilation: theory and practice. AACN Clin Issues 12:234-246
- ^ Dietrich Henzler (2011). "What on earth is APRV?". Critical care (London, England) 15 (1): 115. doi:10.1186/cc9419. PMID 21345265.
- ^ Adrian A. Maung & Lewis J. Kaplan (July 2011). "Airway pressure release ventilation in acute respiratory distress syndrome". Critical care clinics 27 (3): 501–509. doi:10.1016/j.ccc.2011.05.003. PMID 21742214.
- ^ M. Baum, H. Benzer, C. Putensen, W. Koller & G. Putz (September 1989). "[Biphasic positive airway pressure (BIPAP)--a new form of augmented ventilation]". Der Anaesthesist 38 (9): 452–458. PMID 2686487.
- ^ C. Putensen, S. Zech, H. Wrigge, J. Zinserling, F. Stuber, T. Von Spiegel & N. Mutz (July 2001). "Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury". American journal of respiratory and critical care medicine 164 (1): 43–49. PMID 11435237.
Mechanical ventilation Fundamentals Modes of mechanical ventilation • Mechanical ventilation in emergencies • Mechanical ventilation in neonates • Nomenclature of mechanical ventilationModes Volume controlled continuous mandatory ventilation • Volume controlled intermittent mandatory ventilation • Pressure controlled continuous mandatory ventilation • Pressure controlled intermittent mandatory ventilation • Continuous spontaneous ventilation • High-frequency ventilation (passive) • High-frequency ventilation (active)Related illness ARDS • Pulmonary barotrauma • Pulmonary volutrauma • Ventilator-associated pneumonia • Oxygen toxicity • Ventilator-associated lung injurySettings Ventilation
Wikimedia Foundation. 2010.
Look at other dictionaries:
Volume controlled intermittent mandatory ventilation — (VC IMV) refers to any mode of mechanical ventilation with preset tidal volume (VT) and inspiratory flow. Spontaneous breaths (i.e., inspiration is patient triggered and patient cycled) can exist between mandatory breaths. For intermittent… … Wikipedia
Volume controlled continuous mandatory ventilation — (VC CMV) is a mode of mechanical ventilation where breaths are delivered based on set variables. The patient may initate breaths by attempting to breathe. Once a breath is initated, either by the patient or by the ventilator the set tidal volume… … Wikipedia
Mechanical ventilation — In architecture and climate control, mechanical or forced ventilation is the use of powered equipment, e.g. fans and blowers, to move air see ventilation (architecture). Mechanical ventilation Intervention … Wikipedia
Modes of mechanical ventilation — Contents 1 Positive and negative pressure ventilation 1.1 Negative pressure ventilation 1.1.1 Types of negat … Wikipedia
Nomenclature of mechanical ventilation — Contents 1 Volume Controlled Continuous Mandatory Ventilation 1.1 Terms replaced by VC CMV 2 … Wikipedia
Continuous spontaneous ventilation — Uses Gives assisting pressure and flow during inhalation. Trigger Flow, Volume or Pressure Limit Pressure Inspiratory Cycle Flow Servo no Settings … Wikipedia
Ventilation — The exchange of air between the lungs and the atmosphere so that oxygen can be exchanged for carbon dioxide in the alveoli (the tiny air sacs in the lungs). In pulmonary medicine, a distinction is made between pulmonary and alveolar ventilation.… … Medical dictionary
Neurally adjusted ventilatory assist — NAVA Neurally Adjusted Ventilatory Assist is a mode of mechanical ventilation. NAVA delivers assist in proportion to and in synchrony with the patient s respiratory efforts, as reflected by the Edi signal. This signal represents the electrical… … Wikipedia
Искусственное дыхание — Эту статью следует викифицировать. Пожалуйста, оформите её согласно правилам оформления статей. Искусственное дыхание (искусственная вентиляция легких, ИВЛ) комплекс мер, направленных на поддержание оборота в … Википедия
Beatmung — dient der Unterstützung oder dem Ersatz unzureichender oder nicht vorhandener Spontanatmung. Ihre lebenserhaltende Funktion ist zentraler Bestandteil in der Anästhesiologie, der Notfallmedizin und der Intensivmedizin. Es wird unterschieden… … Deutsch Wikipedia
 18+© Academic, 2000-2025
18+© Academic, 2000-2025- Contact us: Technical Support, Advertising
Dictionaries export, created on PHP, Joomla, Drupal, WordPress, MODx.