- Legg–Calvé–Perthes syndrome
Infobox_Disease
Name = Legg–Calvé–Perthes syndrome
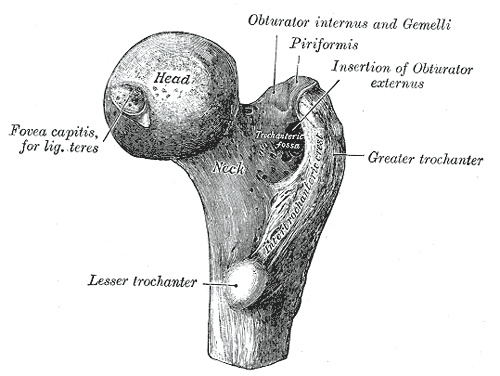
Caption = Upper extremity of right femur viewed from behind and above.
DiseasesDB = 9891
ICD10 = ICD10|M|91|1|m|91
ICD9 = ICD9|732.1
ICDO =
OMIM =
MedlinePlus = 001264
eMedicineSubj = radio
eMedicineTopic = 387
MeshID = D007873Legg–Calvé–Perthes syndrome is a
degenerative disease of thehip joint , where a loss ofbone mass leads to some degree of collapse of the hip joint, that is, to deformity of the ball of the femur and the surface of the hip socket. The disease is typically found in young children and small dogs, and it can lead to osteoarthritis in adults. Perthes can also sometimes continue into adulthood.It is the
idiopathic avascularosteonecrosis of the capital femoralepiphysis of thefemoral head . It is caused by an interruption to the blood supply of the head of thefemur close to thehip joint . It is equivalent to adultavascular necrosis .It is also known as Perthes disease, [G. Perthes. Über Arthritis deformans juvenilis. Deutsche Zeitschrift für Chirurgie, Leipzig, 1910, 107: 111-159.] ischemic necrosis of the hip, coxa plana, osteochondritis and avascular necrosis of the femoral head, or Legg–Perthes Disease or Legg–Calve-Perthes Disease (LCPD).
Cause
The direct cause is a reduction in
blood flow to the joint, though what causes this is unknown. It is thought that the artery of theligamentum teres femoris closes too early, not allowing time for themedial circumflex femoral artery to take over. Fact|date=May 2008Genetics does not appear to be a determining factor, though it may be involved. When the disease is genetic in origin, it typically runs along the male line. Some evidence suggests that parental smoking may be a factor, though this is not yet proven, or more recently that a deficiency of some blood factors used to disperse blood clots may lead to blockages in the vessels supplying the joint, but that, too, has not been proven.igns and symptoms
Symptoms are hip, knee, or groin pain, exacerbated by hip/leg movement. There is a reduced
range of motion at the hip joint and a painful orantalgic gait . There may be atrophy of thigh muscles from disuse and an inequality of leg length. In some cases, some activity can cause severe irritation or inflammation of the damaged area including standing, walking, running, kneeling, or stooping repeatedly for an extended period of time.The first signs are complaints of soreness from the child, which are often dismissed as
growing pains , and limping or other guarding of the joint, particularly when tired. The pain is usually in the hip, though can also be felt in the knee (so-called 'referred pain '). In some cases, pain is felt in the unaffected hip and leg. Fact|date=May 2008 This is due to the child favoring the injured side and placing the majority of the weight on the "good" leg. It is predominantly a disease of boys (4:1 ratio). Whereas Perthes is generally diagnosed between 5 and 12 years of age, it has been diagnosed in children as young as infants. Typically the disease is only seen in one hip, bilateral perthes is seen in about 8-10% of children diagnosed.Diagnosis
X-Ray s of the hip joint are absolutely necessary. X-rays will show asmall, flattened and fragmented head of femur. Abone scan may be useful in helping determine the extent of the avascular changes. A hip aspiration may be performed if there is suspicion of aseptic arthritis .Diagnosis is made predominantly by
X-ray study, together with physical examination (MRI s have also been found useful for judging the extent of the deformity). Sufferers typically have limited range of motion in their hip, particularly when rotating the joint.Treatment
The goal of treatment is to avoid severe degenerative arthritis.
Orthopedic assessment is crucial. Younger children have a better prognosis than older children. Currently, there are studies conducted onbisphosphonates [Intravenenous Bisphosphonate Therapy for Traumatic Osteonecrosis of the Femoral Head. Manoj Ramachandran, FRCS(Tr&Orth), Kate Ward, MPH, Richard R. Brown, FRCS(Tr&Orth), Craig F. Munns, FRACP, Christopher T. Cowell, FRACP and David G. Little, FRACS(Orth) ] for treatment of Perthes. Analgesic medication may be given as necessary.Treatment has traditionally centered on removing pressure from the joint until the disease has run its course. Options have included
bed rest and traction (to separate the femur from the pelvis and reduce wear), often for several months or even years. Plaster casts were also popular, again to isolate the joint. Recent evidence suggests that these methods are not effective, and treatment seems to be moving towards a mixture of careful monitoring,physiotherapy , and surgical intervention when necessary.To maintain activities of daily living, a custom orthoses may be used. These devices internally rotate the femoral head and abduct the leg(s) at 45 degrees. Orthoses can start as proximal as the lumbar spine (LSO),and extend the length of the limbs to the floor. Most functional bracing is achieved using a waist belt and thigh cuffs derived from the Scottish-Rite Orthosis [Katz, Jacob. Legg–Calve-Perthes-Disease. Praeger, New York. 1984.] . These devices are typically prescribed by aphysician and implemented by a certifiedorthotist . For older children, the distraction method has been found to be a successful treatment by using anexternal fixator which relieves the hip from carrying the body's weight. This allows room for the top of the femur to regrow and shape better.Modern treatment focuses on removing pressure from the joint in concert with physiotherapy. Pressure is minimized on the hip through use of
crutch es or acane , and the avoidance of running-based sports.Swimming is highly recommended - it allows exercise of the hip muscles with the full range of motion, while reducing the stress to a minimum. Physiotherapy treatment generally involves a daily series of exercises, with weekly meetings with a physiotherapist to monitor progress. These exercises focus on improving and maintaining a full range of motion of the femur within the hip socket. Performing these exercises during the healing process is essential to ensure that the femur and hip socket have a perfectly smooth interface. This will minimize the long term effects of the disease.Perthes is a long-term problem - treatment is aimed at minimizing damage while the disease runs its course, not at 'curing' the disease. As sufferers age, problems in the knee and back can arise secondary to abnormal posture and stride adopted to protect the affected joint. The condition is also linked to arthritis of the hip and other joints, though this appears not to be an inevitable consequence. Hip replacements are relatively common as the already damaged hip suffers routine wear; this varies by individual, but generally is required any time after age 50.
Incidence
Perthes is a relatively unusual condition, with only 1 in 1200 children being affected. Fact|date=May 2008
Caucasians are affected more frequently than other races, males are affected 4-5 times more often than females, suggesting a partial sex-linked genetic inheratance of the syndrome. Fact|date=May 2008 1 in 100 male children of adults with Legg–Calvé–Perthes syndrome also exhibit the syndrome. It is most commonly seen in persons aged 3-12 years, with a median of 6 years of age. Fact|date=May 2008In the US, 1 in 1200 children younger than 15 years will have this disease while in the UK the incidence is higher, with Ireland having the highest percentage. Fact|date=May 2008 It is also found in Latin Americans, Asians and Inuit Indians.
Prognosis
Children younger than 6 or 7 have the best prognosis since they have time for the dead bone to revascularize and remodel. Children that have been diagnosed with Perthes' Disease after the age of 10 are at a very high risk of developing
osteoarthritis andCoxa Magna .Legg–Calvé–Perthes disease in dogs
This is also known as aseptic necrosis of the femoral head. Toy and small breeds, particularly Toy
Poodles ,Yorkshire Terrier s,Pug s,Jack Russell Terrier s, andDachshund s can be affected. Hip pain is usually seen by the age of 6 to 8 months.cite book|author=Ettinger, Stephen J.;Feldman, Edward C.|title=Textbook of Veterinary Internal Medicine|volume=2|pages=1873, v|edition=5th ed.|publisher=W.B. Saunders Company|year=2000|id=ISBN 0721672582] The disease is bilateral in 12 to 16 percent of cases.cite journal |author=Demko J, McLaughlin R |title=Developmental orthopedic disease |journal=Vet Clin North Am Small Anim Pract |volume=35 |issue=5 |pages=1111–35, v |year=2005 |pmid=16129135 |doi=10.1016/j.cvsm.2005.05.002]X-ray s are necessary to make the diagnosis and show increased opacity and focal lysis in the head of the femur, and later in the disease, collapse and fracture of the neck of the femur. The recommended treatment is surgical removal of the head of the femur, but conservative treatment (rest, exercise restriction, and pain medication) may be effective in a limited number of cases (less than 25 percent, according to some studies). The prognosis is excellent with surgery.References
External links
* [http://health.groups.yahoo.com/group/intl_perthes_support/ Legg Perthes Support Group International] , Yahoo group
* [http://www.perthes.org.uk Perthes Association (UK)]
*
* [http://www.perthesnz.bravehost.com - information about therapies, treatments and a comprehensive medical glossary in plain english]
Wikimedia Foundation. 2010.