- Lambert-Eaton myasthenic syndrome
Infobox Disease
Name = PAGENAME
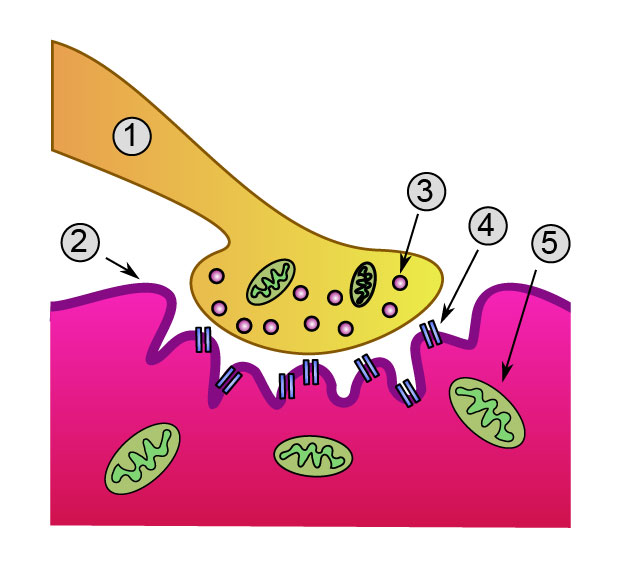
Caption = Detailed view of a neuromuscular junction:
1.Presynaptic terminal
2.Sarcolemma
3.Synaptic vesicle
4.Nicotinic acetylcholine receptor
5.Mitochondrion
DiseasesDB = 4030
ICD10 = ICD10|G|73|1|g|70
ICD9 = ICD9|358.1
ICDO =
OMIM =
MedlinePlus = 000710
eMedicineSubj = neuro
eMedicineTopic = 181
eMedicine_mult = eMedicine2|emerg|292
MeshID = D015624Lambert-Eaton myasthenic syndrome (LEMS) is a rare
autoimmune disorder which affects calcium channels of the nerve-muscle (neuromuscular) junction. Theetiology of LEMS may resemblemyasthenia gravis , but there are substantial differences between the clinical presentation and pathogenetic features of the two disorders.While children and young adults may be affected, the disease is usually observed in middle aged and older individuals. The incidence of the disease is difficult to determine due to its low frequency.
History
Anderson was the first person to mention a case with possible clinical findings of LEMS in 1953, but Lambert, Eaton and Rooke were the first physicians to substantially describe the clinical and electrophysiological findings of the disease in 1966. [WhoNamedIt|synd|2738|Lambert-Eaton-Rooke syndrome] [E. H. Lambert, L. M. Eaton, E. D. Rooke. Defect of neuromuscular conduction associated with malignant neoplasms.American Journal of Physiology, Bethesda, Maryland, 1956, 187: 612-613.]
It is usually associated with auto-immune self antibodies to the pre-synaptic
voltage gated calcium channel s,cite journal |author=Newsom-Davis J |title=Lambert-Eaton myasthenic syndrome |journal=Rev. Neurol. (Paris) |volume=160 |issue=2 |pages=177–80 |year=2004 |month=February |pmid=15034474 |doi= |url=http://www.masson.fr/masson/MDOI-RN-02-2004-160-2-0035-3787-101019-ART04] which leads to neuromuscular block.Causes
While LEMS may be found as a solitary disease, 50% of cases have an associated malignancy. Malignancies that may be found with LEMS may include small-cell
lung cancer ,lymphoma ,non-Hodgkin's lymphoma ,T-cell leukemia ,non-small cell lung cancer ,prostate cancer , and transitional cell carcinoma of the bladder. The myasthenic syndrome associated with thymoma is actually true myasthenia gravis, where weakness worsens with repeated activity (as opposed to LEMS, where weakness improves with repeated activity). [ Monden et al. Ann Thoracic Surg, 1984:46-52.]Whether solitary or cancer-associated, the disease is believed to be of
autoimmune origin. In 1989, the previously anticipated antibodies were demonstrated to be directed against presynapticcalcium channels , which are located in neuromuscular junction (seesynapse ) and are responsible for the efficient release ofacetylcholine .Fact|date=May 2008 The calcium channel antibodies prevent the opening of calcium channels and thus prevent the release of acetylcholine.There are some patients that do not carry these antibodies in their serum samples and the exact cause of disease in these cases still remains to be determined.Fact|date=May 2008 In cases with both LEMS and lung cancer (usually small cell type), the antibodies are suggested to be aimed at cancer cells and to bind and affect the antigens in neuromuscular junction accidentally.
Clinical findings
The major clinical finding is progressive weakness that does not usually involve the respiratory muscles and the muscles of face. In patients with affected ocular and respiratory muscles, the involvement is not as severe as
myasthenia gravis . The proximal parts of the legs and arms are predominantly affected. Many patients have autonomic symptoms likedry mouth orimpotence .Reflexes are usually reduced or absent.Diagnosis
The diagnosis is established by clinical and laboratory findings (
chest x-ray for a possible lung malignancy, antibodies tocalcium channels , incremental response in repetitive nerve stimulation). Incremental response is an increased response of muscle fibers to very high frequencies of electrical stimulation. Observed increase in the response of muscle fibers proves that there is a difficulty with the release of acetylcholine and this difficulty can be overwhelmed by intensive stimulation.Treatment
Corticosteroids ,azathioprine and3,4-diaminopyridine are used in treatment of LEMS with limited success. In some cases with a progressive and intractable course,plasma exchange or intravenous immunoglobulin can be tried.3,4 diaminopyridine work by blocking K+ channel efflux in nerve terminal so that
action potential duration is increased. Ca2+ channels can then be open for longer time and allow greater acetylcholine release to stimulate muscle at end plate.References
Wikimedia Foundation. 2010.