- Enalapril
drugbox
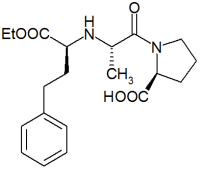
IUPAC_name = 1- [2-(1-ethoxycarbonyl-3-phenyl-propyl) aminopropanoyl] pyrrolidine-2-carboxylic acid.
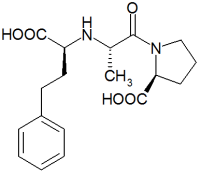
(Diagrams above are enalpril and enalaprilat, respectively. Data below refers to enalapril unless indicated)
width = 200
CAS_number = 75847-73-3
ATC_prefix = C09
ATC_suffix = AA02
ATC_supplemental =
PubChem = 5362032
DrugBank = APRD00510
C=20 | H=28 | N=2 | O=5
molecular_weight = 376.447 g/mol
bioavailability = 60% (oral)
protein_bound =
metabolism = hepatic (to enalaprilat)
elimination_half-life = 11 hours (enalaprilat)
pregnancy_AU = 5
pregnancy_US =
pregnancy_category =
legal_status = Rx-only
routes_of_administration =
excretion = renalEnalapril is an angiotensin converting enzyme (ACE) inhibitor used in the treatment of
hypertension and some types of chronicheart failure . Enalapril was the first member of the group of ACE inhibitors known as the dicarboxylate-containing ACE inhibitors. It is marketed byMerck & Co. (Merck, Sharp & Dohme) under the trade names, "Renitec" and "Vasotec". The primary effect of enalapril, as with all ACE inhibitors, is to lower blood pressure.Development
Enalapril was developed by researchers at
Merck & Co. as part of their efforts to develop novel treatments for hypertension by modulating the renin-angiotensin-aldosterone (RAS) system.The success of Squibb in developing the first inhibitor,
captopril , provided a major impetus for Merck's research laboratories to develop a competing product. Captopril was not without its problems, however, as it was believed (and shown to be true) that thesulfhydryl -moiety of captopril was responsible for such adverse effects as metallic taste.Enalaprilat
Enalaprilat, the first dicarboxylate-containing ACE inhibitor, was developed partly to overcome these limitations of captopril. The sulfhydryl-moiety was replaced by a carboxylate-moiety, but additional modifications were required in its structure-based design to achieve a similar potency to captopril.
Enalaprilat itself, however, was not without its problems. The consequence of the structural modifications was that it proved to have unfavourable ionisation characteristics to allow sufficient potency for oral administration (in tablets). Thus enalaprilat was only suitable for
intravenous administration. This was overcome by the researchers at Merck by theesterification of enalaprilat with ethanol to produce enalapril.As a
prodrug , enalapril is metabolised "in vivo" to the active form enalaprilat by variousesterase s. Peak plasma enalaprilat concentrations occur 2 to 4 hours after oral enalapril administration. Elimination thereafter is biphasic, with an initial phase which reflects renal filtration (elimination half-life 2 to 6 hours) and a subsequent prolonged phase (elimination half-life 36 hours), the latter representing equilibration of drug from tissue distribution sites.The prolonged phase does not contribute to drug accumulation on repeated administration but is thought to be of pharmacological significance in mediating drug effects. Renal impairment [particularly creatinine clearance < 20 ml/min (< 1.2 L/h)] results in significant accumulation of enalaprilat and necessitates dosage reduction. Accumulation is probably the cause of reduced elimination in healthy elderly individuals and in patients with concomitant diabetes, hypertension and heart failure.
A prototype for others
Most importantly, perhaps, the
QSAR -based modifications in structure serendipitously led to an improved understanding of the structure of ACE which aided in the development of subsequentcarboxylate -containing ACE inhibitors.ide-effects
*
External links
* [http://www.biovail.com/local/files/VasotecPI.pdf Prescribing Information for VASOTEC]
Wikimedia Foundation. 2010.